Trichomycosis axillaris treatment and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
trichomycosis axillaris treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
I have comprehensive data from multiple authoritative sources. Here is a complete, well-structured answer:
Trichomycosis Axillaris — Treatment & Management
Also known as: Trichobacteriosis axillaris
Overview
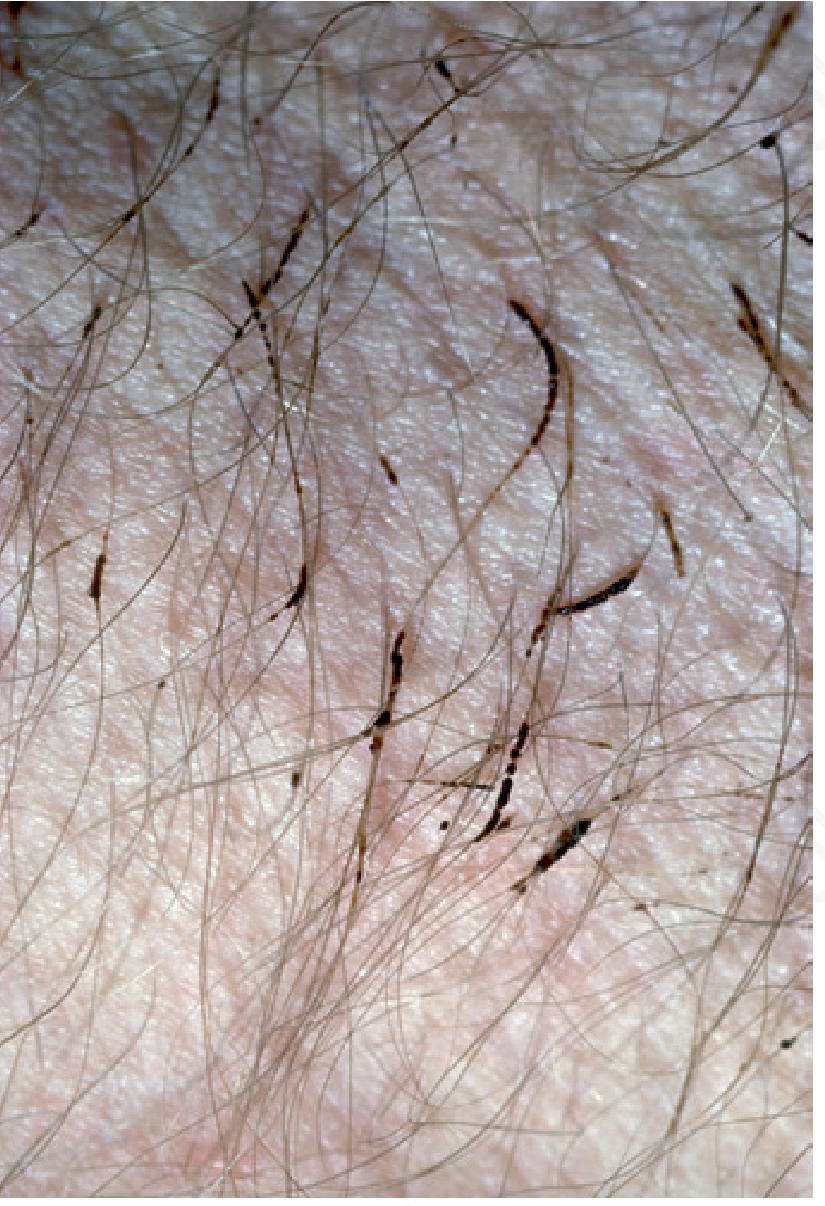
Trichomycosis axillaris is a superficial bacterial infection of axillary (and less often pubic or scalp) hair caused by Corynebacterium species. It is characterized by discrete 1–2 mm nodules or cylindrical sheaths adherent to the hair shafts, which appear yellow, red, or black. Associated features include hyperhidrosis, characteristic odor, and occasionally red-stained sweat that discolors clothing. It frequently coexists with erythrasma and pitted keratolysis (the "corynebacterial triad").
Diagnosis Pointers
| Feature | Detail |
|---|---|
| Wood's lamp | Pale yellow fluorescence (helps distinguish from erythrasma's coral-red) |
| Gram stain | Gram-positive rods in concretions |
| Microscopy | Differentiates from white piedra, nits, hair casts, lice |
| Nodule size | Usually smaller than piedra nodules |
Treatment
1. Shaving (First-line / Fastest)
Shaving the affected hair provides immediate cure — it is the single fastest and most effective intervention. This is the preferred approach when rapid resolution is desired.
2. Topical Antibiotics
- Clindamycin 1% solution or gel — effective topical option for axillary and pubic trichomycosis
- Erythromycin topical — well-established option
- Bacitracin — effective for pubic involvement
3. Other Topical Agents
- Benzoyl peroxide — antibacterial, useful as treatment and adjunct
- Naftifine — has antibacterial properties alongside its antifungal action; effective in combination
- Antimicrobial/antibacterial soaps — help treat and prevent recurrences
4. Addressing Hyperhidrosis
Because hyperhidrosis is the key predisposing factor, any modality that reduces sweating should be combined with antibiotic therapy:
- Topical aluminum chloride (antiperspirant)
- This addresses the underlying microenvironment that supports bacterial overgrowth
5. Oral Antibiotics (Selected Cases)
- Oral erythromycin — reserved for more resistant or extensive cases, particularly pubic involvement
Prevention of Recurrence
- Regular use of antimicrobial soaps
- Management of hyperhidrosis (aluminum chloride antiperspirants)
- Good axillary hygiene and keeping the area dry
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| White piedra | Larger, softer nodules; fungal hyphae on microscopy |
| Black piedra | Hard, gritty nodules; perpendicularly arranged hyphae |
| Pediculosis | Nits visible; lice detectable |
| Hair casts | Microscopy differentiates |
| Erythrasma | Skin patches (not hair), coral-red fluorescence on Wood's lamp |
Summary of Treatment Options
| Approach | Role |
|---|---|
| Shaving | Fastest cure — first-line |
| Clindamycin topical | Topical antibiotic — first-line |
| Erythromycin topical | Topical antibiotic — first-line |
| Benzoyl peroxide | Effective alternative |
| Naftifine | Dual antibacterial/antifungal |
| Aluminum chloride | Treats underlying hyperhidrosis |
| Oral erythromycin | Resistant/extensive cases |
| Antibacterial soaps | Prevention of recurrence |
Sources: Andrews' Diseases of the Skin, p. 62–69 | Dermatology 2-Volume Set 5e (Elsevier), p. 5320–5322 | Campbell-Walsh-Wein Urology, p. 1779–1785
Recent literature note: A 2023 review (PMID 37900398) in Cureus highlights that this condition remains widely underdiagnosed and emphasizes the preferred terminology "trichobacteriosis," reinforcing shaving and topical antibiotics as the mainstay of management — consistent with textbook guidance above.
This is a shared conversation. Sign in to Orris to start your own chat.