Femoral bypass
Reading File
Finding Sources
Finding Sources
Searching PubMed
"femoral bypass" OR "femoropopliteal bypass"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material. Here is the full answer:
Femoral Bypass
Femoral bypass procedures restore blood flow to the lower extremities when native arterial pathways are occluded or stenosed. There are several distinct types based on the inflow source and the outflow target.
1. Femoral-Femoral (Cross-Femoral) Bypass
Indication
Used for unilateral iliac artery occlusive disease. A patent contralateral iliac system without hemodynamically significant disease is essential to graft success. With advances in endovascular technology, it is seldom used today.
- Fischer's Mastery of Surgery, 8e
Concept
This is an extra-anatomic bypass: unilateral iliac inflow perfuses both lower extremities via a subcutaneously tunneled graft crossing the pubic region.
Operative Steps
- The abdomen and both groins to mid-thigh are prepped and draped.
- Standard vertical or transverse groin incisions are made, placed slightly more distal than usual - the inguinal ligament is visualized at the uppermost extent but otherwise avoided.
- Anastomoses are placed far enough distally on the femoral arteries to prevent acute angulation of the graft as it courses across the lower abdominal wall.
- A subcutaneous, prefascial tunnel is created in an arc between the groins to prevent kinking.
- Crossing lymphatics must be carefully ligated - any wound complication with a subcutaneously tunneled prosthetic graft can be catastrophic.
Key technical point: Anastomosis placed too close to the inguinal ligament is prone to angulation/kinking with hip flexion or when the abdominal panniculus "sags" when standing. The anastomosis should be placed further distally.
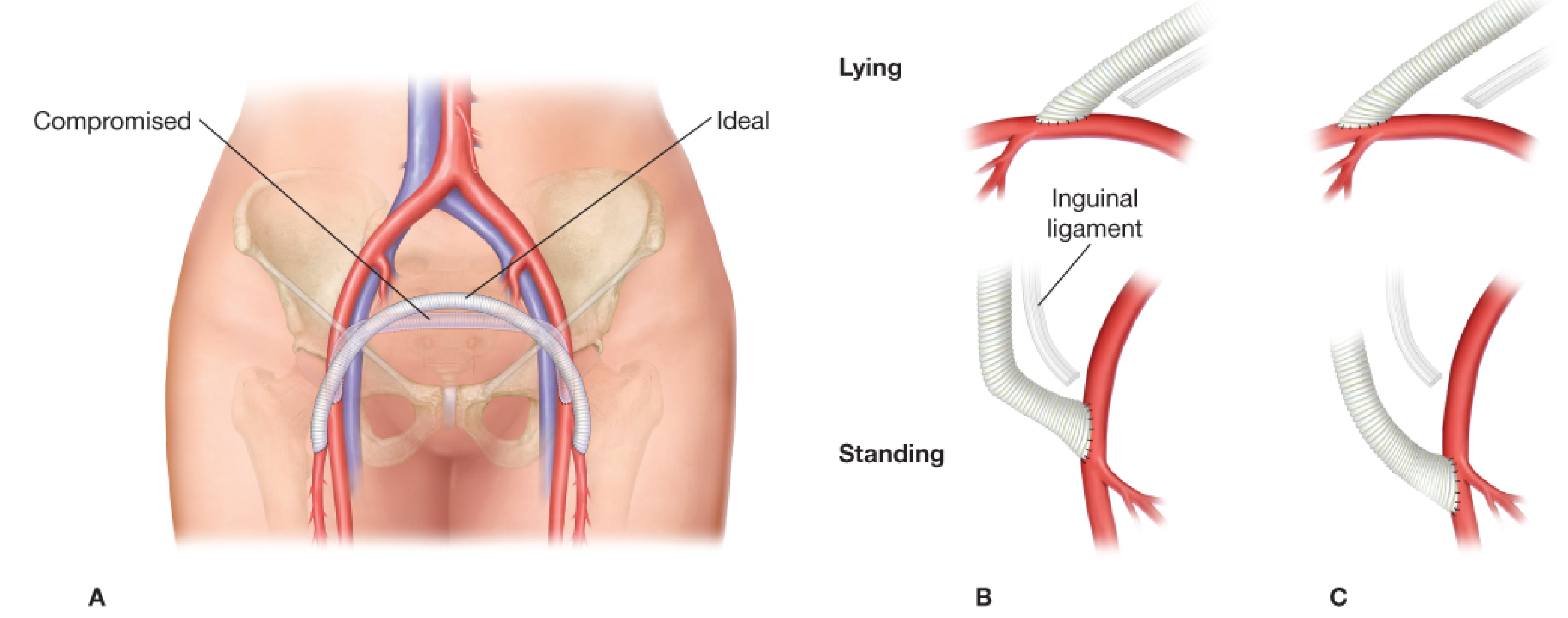
Panel A: Graft arc showing "compromised" vs "ideal" anastomotic position. Panels B-C: How placement too close to the inguinal ligament (B) causes kinking with standing, whereas distal placement (C) prevents this.
Patency
5-year primary patency: 73-75%
- Sabiston Textbook of Surgery
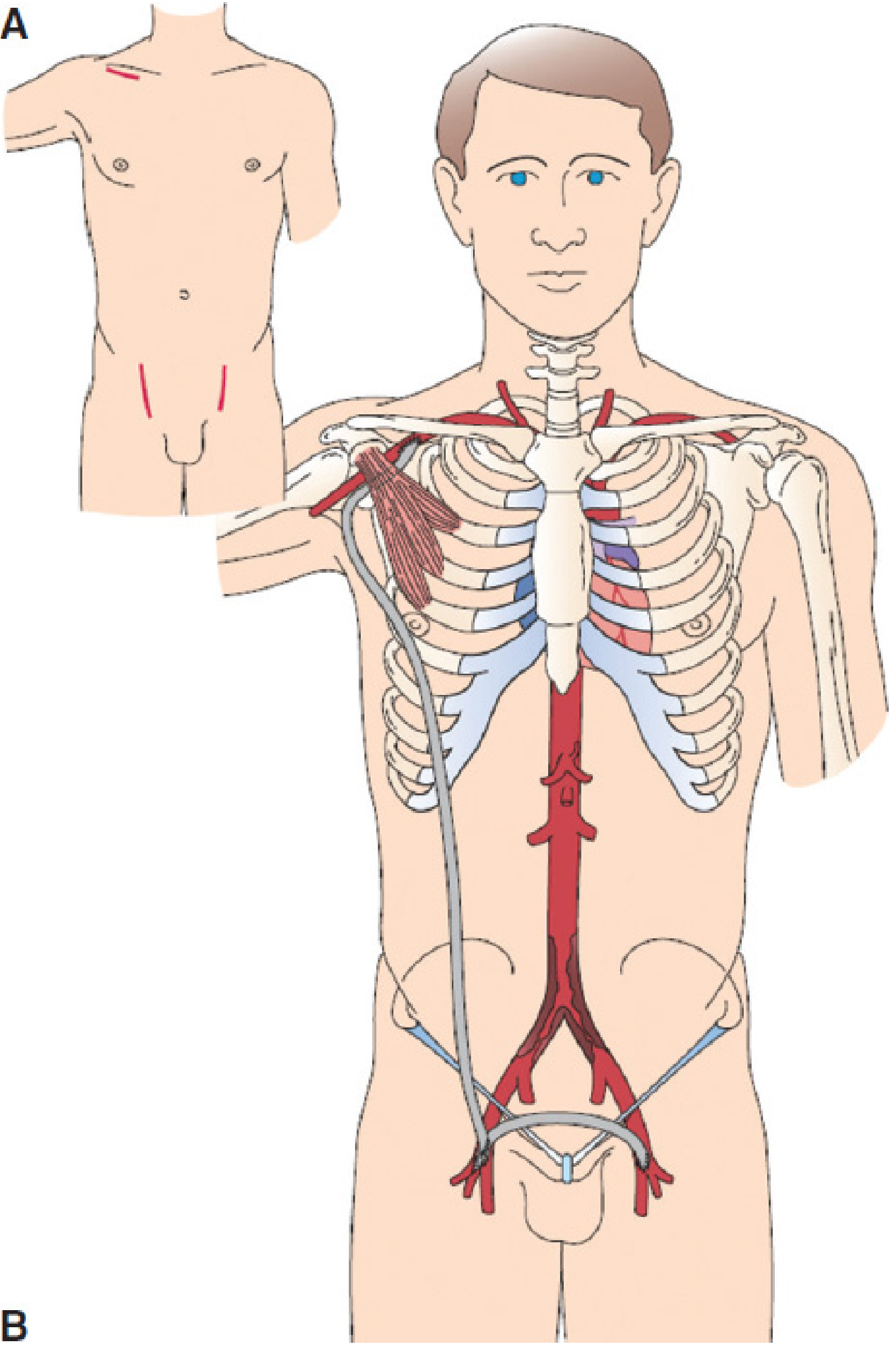
2. Axillofemoral Bypass (and Axillobifemoral Bypass)
This is another extra-anatomic option for high-risk patients with severe comorbidities or a "hostile" abdomen where aortic surgery is too dangerous.
Inflow selection
The axillary artery with the higher brachial blood pressure is chosen (usually right). A weak brachial/radial pulse or lower BP mandates preoperative CTA or DSA to rule out proximal stenosis.
Operative Steps
- A transverse infraclavicular incision exposes the first part of the axillary artery by splitting the pectoralis major and minor muscles.
- An 8-mm externally supported ePTFE graft is tunneled from the axillary artery in the anterior axillary line down to the ipsilateral groin (posterior to pectoralis minor).
- Some graft redundancy is left in the axilla to reduce traction on the anastomosis with arm abduction.
- The contralateral groin is then revascularized with a femoral-femoral (cross-femoral) bypass, completing the axillobifemoral configuration.
Why bifemoral > unifemoral?
Providing flow to both femoral arteries (axillobifemoral) increases flow velocities within the long main shaft of the graft, improving long-term patency.
Patency
5-year primary patency: 51-84% for axillofemoral grafts (lower than direct aortic reconstruction)
- Sabiston Textbook of Surgery
When it is used
Reserved for patients with critical limb ischemia (CLI) and very poor surgical risk or limited life expectancy - NOT for claudication alone, because of lower patency.
3. Infrainguinal Bypass: Femoropopliteal and Femorotibial
These address infrainguinal occlusive disease (SFA, popliteal, tibial segments).
Conduit of choice
Autologous great saphenous vein (GSV) - either reversed or in-situ - is the gold standard for all infrainguinal bypasses due to superior patency compared to prosthetic. Arm vein or spliced vein may be used when GSV is unavailable.
Femoropopliteal Bypass (Above-knee vs Below-knee)
Above-knee popliteal (AKP) bypass:
- Popliteal artery exposed medially; the tunnel runs in the subsartorial plane.
- Prosthetic (ePTFE or Dacron) is acceptable for above-knee targets when vein is unavailable.
Below-knee popliteal (BKP) bypass:
- Exposed through a longitudinal incision 1-2 cm posterior to the medial edge of the tibia.
- Pes anserinus tendon is divided; the posterior fascia is divided longitudinally.
- The medial head of the gastrocnemius is bluntly mobilized and retracted posteriorly.
- The tunneler is advanced from the popliteal fossa between the heads of the gastrocnemius to the groin.
- Vein is the strongly preferred conduit for below-knee targets.
- Fischer's Mastery of Surgery, 8e
Femorotibial Bypass
- Indicated for limb-threatening ischemia when popliteal artery is not a suitable outflow target.
- Tibial arteries in diabetics are often heavily calcified - vessels should NOT be clamped; use a tourniquet or intraluminal control (Fogarty catheters, Flo-Rester devices).
- Avoid formal endarterectomy; remove loose calcified fragments.
- Running 6-0 or 7-0 Prolene sutures on a CC (calcified coronary) needle is very helpful.
- In redo settings, the graft is tunneled in a deep subcutaneous plane beneath intact skin to avoid wound complications.
4. Extra-Anatomic Bypass for Infected Grafts
When an aortic or femoral graft becomes infected, extra-anatomic bypass (typically axillobifemoral with femoral-femoral component) through clean tissue planes is considered the gold standard:
- All infected prosthetic material is completely excised with debridement to healthy margins.
- New ePTFE conduit is placed through uninfected tissue planes.
- If groin infection is present, saphenous vein or cryopreserved conduit replaces prosthetic for the femoral-femoral component.
- Outflow can be to SFA or profunda femoris (approached laterally via the sartorius to avoid contaminated femoral triangle).
- Current Surgical Therapy, 14e
5. Summary Table
| Procedure | Indication | Inflow | Conduit | 5-yr Patency |
|---|---|---|---|---|
| Femoral-femoral | Unilateral iliac occlusion | Contralateral femoral | ePTFE | 73-75% |
| Axillofemoral | Advanced aortoiliac, poor surgical risk | Axillary artery | Externally supported ePTFE (8mm) | 51-84% |
| Femoropopliteal (AK) | SFA occlusion, good AK target | Common femoral | Vein (preferred) or ePTFE | ~65-80% (5yr) |
| Femoropopliteal (BK) | SFA occlusion, BK target | Common femoral | Vein strongly preferred | ~60-70% (5yr) |
| Femorotibial | CLI, no suitable popliteal target | Common femoral | Autologous vein only | Variable |
Recent Evidence
A 2024 systematic review and meta-analysis (PMID 38582218) evaluated heparin-bonded expanded PTFE grafts for below-the-knee femoral bypass surgery, an area of active investigation for improving prosthetic graft performance when autologous vein is unavailable.
Sources: Fischer's Mastery of Surgery (8e), Sabiston Textbook of Surgery, Mulholland and Greenfield's Surgery (7e), Current Surgical Therapy (14e).
This is a shared conversation. Sign in to Orris to start your own chat.