Varicose vein. Associate with syndrome and family history
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
varicose veins genetics family history risk factors
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is the complete synthesis:
Varicose Veins: Associated Syndromes and Family History
Definition and Classification
Varicose veins are dilated, tortuous superficial veins measuring at least 3 mm in diameter in the upright position. They are classified as:
- Primary - originate in the superficial system due to defective valve structure, intrinsic vein wall weakness, or high intraluminal pressure
- Secondary - result from deep-venous hypertension, deep-venous obstruction, or incompetent perforating veins; also caused by arteriovenous fistulas
The CEAP classification system (revised 2020) stages chronic venous disease from C0 (no visible veins) to C6 (active venous ulcer), with C2 representing varicose veins.
- Current Surgical Therapy 14e
- Harrison's Principles of Internal Medicine 22E
Family History and Genetic Predisposition
Approximately 50% of patients with primary varicose veins have a positive family history. This is one of the strongest risk factors.
- Harrison's Principles of Internal Medicine 22E states directly: "Approximately one-half of these patients have a family history of varicose veins."
- Mulholland and Greenfield's Surgery confirms: "Relevant risk factors for varicose veins are advanced age, a positive family history, female gender, multiparity, and obesity."
- Current Surgical Therapy 14e lists family history as a primary risk factor for venous valvular dysfunction, alongside female gender, activity level, and occupation.
- Mulholland references a 2012 Circ Cardiovasc Genet review on "familial, genetic, and congenital aspects of primary varicose vein disease," which confirms a clear hereditary component.
- Mulholland also notes that hereditary varicose veins tend to appear during the second decade of life, earlier than the typical adult-onset pattern.
- Gray's Anatomy for Students notes that "some individuals have a genetic predisposition to developing varicose veins."
Specific genetic/connective tissue associations:
| Condition | Mechanism |
|---|---|
| Ehlers-Danlos syndrome | Connective tissue dysregulation leads to vein wall weakness and varicose veins |
| CADASIL gene mutation | Mentioned as one of the rarer genetic contributors |
| Clonal trisomies | Listed as a congenital etiology to screen for |
Syndromes Associated with Varicose Veins
1. Klippel-Trenaunay Syndrome (KTS)
The most classic syndrome associated with varicose veins.
Classic triad:
- Cutaneous port-wine capillary naevus involving the lower limb
- Varicose veins - unilateral, appearing at birth or in childhood
- Soft tissue and bony hypertrophy (hemihypertrophy) of the involved limb
Additional features:
- Deep veins may be hypoplastic or aplastic
- Associated lymphatic obstruction
- Visceral lesions in ~20% of patients (GI tract, bladder, kidney, lung)
- GI bleeding (most common site: distal colon and rectum)
- Genetic defects in the regulation of angiogenic factor VG5Q have been demonstrated in KTS patients
- Not familial (mesodermal developmental abnormality)
- Increased risk of VTE - LMWH prophylaxis mandatory for surgery

- Bailey & Love's Short Practice of Surgery 28e
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
2. Parkes-Weber Syndrome
Closely related to KTS but distinguished by:
-
Multiple arteriovenous fistulas causing venous hypertension
-
Higher-flow AV shunting (vs. KTS which is a pure low-flow condition)
-
Can lead to venous ulceration and high-output cardiac failure
-
Presents in childhood
-
Bailey & Love's Short Practice of Surgery 28e
-
Harrison's Principles of Internal Medicine 22E
3. May-Thurner Syndrome (Iliac Vein Compression Syndrome)
-
Left common iliac vein compressed by the overlying right common iliac artery
-
Causes secondary deep-venous insufficiency and varicose veins
-
May present with left-leg varicosities, DVT, edema, and venous ulcers
-
Nonthrombotic stenosis may be a "permissive lesion" before becoming clinically significant
-
Harrison's Principles of Internal Medicine 22E
-
Mulholland and Greenfield's Surgery
4. Nutcracker Syndrome (Renal Vein Compression)
-
Compression of the left renal vein between the aorta and superior mesenteric artery
-
Associated with scrotal varicosities (varicocele) due to gonadal vein incompetence
-
Perineal and vulvar varicosities may also signal pelvic venous insufficiency or iliac obstruction
-
Sabiston Textbook of Surgery
-
Current Surgical Therapy 14e
5. Pelvic Congestion Syndrome
-
Seen in multiparous women with pelvic varicosities
-
Varicosities of the leg in conjunction with chronic pelvic pain, dyspareunia, and bladder fullness on standing
-
Caused by ovarian or pelvic venous insufficiency
-
Diagnosed with MR venous imaging (MRVI) or conventional pelvic venography
-
Treatment ranges from hormonal suppression to ovarian vein embolization
-
Sabiston Textbook of Surgery
6. Ehlers-Danlos Syndrome (Type IV)
-
Connective tissue dysregulation weakens the vein wall
-
Varicose veins are a direct consequence of the structural defect
-
Also associated with arterial rupture and small bowel ischemia
-
Mulholland and Greenfield's Surgery
-
Current Surgical Therapy 14e
7. Post-Thrombotic Syndrome (Post-Phlebitic Syndrome)
-
Secondary varicose veins following deep-vein thrombosis
-
DVT causes valve scarring; recanalization fails to restore valve function
-
Results in chronic venous hypertension, varicosities, edema, and ulceration
-
Approximately 50% of deep venous valvular dysfunction is secondary to DVT
-
Mulholland and Greenfield's Surgery
8. Other Associations
- Leg telangiectasias may signal systemic autoimmune diseases: SLE, dermatomyositis, and xeroderma pigmentosum - Sabiston Textbook of Surgery
- Maffucci syndrome - venous malformations with hemangiomas associated with varicose veins - Dermatology 5e
Summary Table
| Syndrome | Key Feature | Varicose Vein Pattern |
|---|---|---|
| Klippel-Trenaunay | Port-wine naevus + limb hypertrophy | Unilateral, congenital, lateral |
| Parkes-Weber | AV fistulas + limb hypertrophy | High-flow, with cardiac failure |
| May-Thurner | Left iliac vein compression | Left leg, with DVT risk |
| Nutcracker | Left renal vein compression | Scrotal/varicocele |
| Pelvic Congestion | Ovarian vein incompetence | Perineal/vulvar, pelvic pain |
| Ehlers-Danlos | Connective tissue defect | Early onset, diffuse |
| Post-Phlebitic | Prior DVT, valve destruction | Secondary, post-thrombotic |
| Primary (familial) | Genetic predisposition | Typical GSV/SSV distribution, onset 2nd decade |
Lymphatic how spread to opposite breast how they communicate ans
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from all major surgical textbooks. Let me compile the complete answer.
Breast Lymphatic Drainage: Communication with the Opposite Breast
Overview of Normal Breast Lymphatic Drainage
The lymphatic vessels of the breast arise in the interlobular connective tissue and in the walls of the lactiferous ducts, communicating with the subareolar plexus (also called the Sappey plexus, described by the anatomist Sappey in 1874/1885). Lymph flows from the skin and lobules toward this central plexus, then outward via efferent collecting routes.
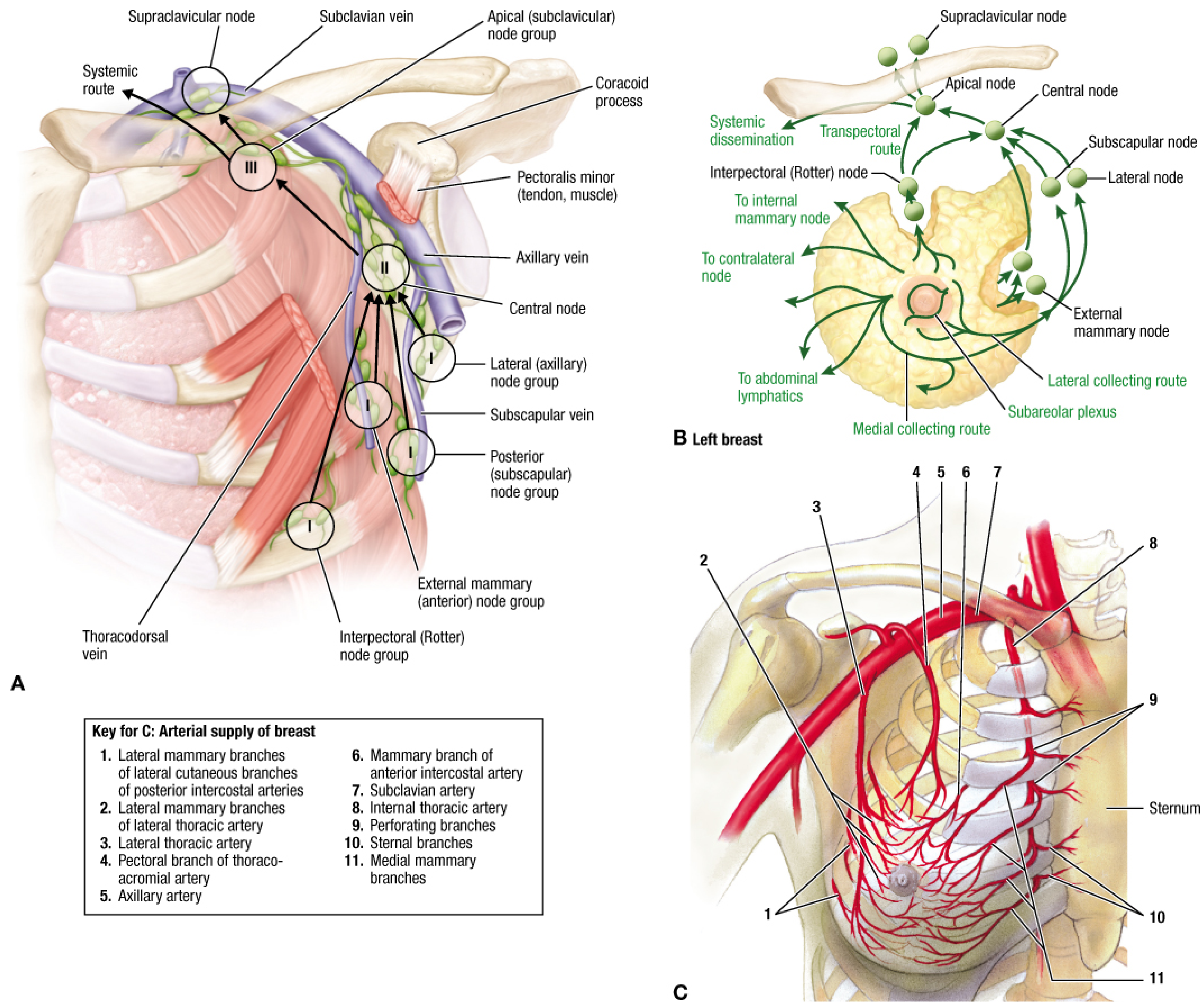
Primary drainage routes (from subareolar plexus):
| Route | % of Drainage | Destination |
|---|---|---|
| Axillary nodes | ~75-98% | External mammary (anterior/pectoral) nodes → Level I → II → III |
| Internal mammary (parasternal) nodes | 20-35% | Along internal mammary vessels, deep to parietal pleura |
| Supraclavicular nodes | ~3% | Via apical axillary nodes |
| Infraclavicular nodes | ~1% | Directly |
| Interpectoral (Rotter's) nodes | ~0.7% | Between pectoralis major and minor |
| Contralateral breast/nodes | Minor | Via subareolar plexus and medial routes |
| Abdominal lymphatics | Minor | Inferior phrenic nodes |
- Sabiston Textbook of Surgery
- Schwartz's Principles of Surgery 11e
- Fischer's Mastery of Surgery 8e
How Lymphatics Communicate with the Opposite (Contralateral) Breast
This is the key question. There are two main anatomical pathways by which lymph - and therefore tumor cells in breast cancer - can reach the contralateral breast:
Pathway 1: Via the Internal Mammary (Parasternal) Nodes - The Most Important Route
This is the primary mechanism for cross-midline spread.
- Lymph from the medial quadrants of the breast drains through lymph vessels that accompany the perforating branches of the internal mammary artery, piercing the intercostal spaces (predominantly 2nd, 3rd, 4th).
- These vessels enter the parasternal (internal mammary) lymph nodes, which lie along both sides of the sternum.
- The parasternal nodes on both sides of the midline are interconnected by lymphatic anastomoses across the anterior chest wall and pre-sternal region.
- From the parasternal nodes on one side, tumor cells may spread across the midline to the opposite parasternal nodes, and from there to the contralateral breast lymphatics or contralateral axilla.
The Thieme Atlas of Anatomy states explicitly:
"The parasternal lymph nodes, which are distributed along the thoracic vessels, chiefly drain the medial portion of the breast. From there, tumor cells may spread across the midline to the opposite side."
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy
Pathway 2: Via the Subareolar (Sappey's) Plexus - Direct Cross Communication
The subareolar lymphatic plexus is a rich dermal and subdermal lymphatic network centered beneath the nipple-areolar complex. This plexus:
- Communicates freely with both the right and left subareolar plexuses via the anterior chest wall skin lymphatics and the pre-sternal lymphatic network
- Acts as a "crossroads" allowing lymph to flow to the contralateral breast directly
As shown clearly in the Fischer's diagram above, "To contralateral node" is labeled as a direct route emerging from the subareolar plexus via the medial collecting route.
Fischer's Mastery of Surgery confirms:
"The subareolar lymphatic plexus drains... also to interpectoral, deltopectoral, supraclavicular, and parasternal nodes, opposite breast, abdominal lymph nodes."
- Fischer's Mastery of Surgery 8e
Summary Diagram of Cross-Breast Communication
LEFT BREAST
↓
Subareolar Plexus (Sappey's plexus)
|
├── Medial collecting route
| ↓
| Internal Mammary / Parasternal Nodes (LEFT)
| ↓
| ←── Anastomosis across STERNUM ───→
| ↓
| Internal Mammary / Parasternal Nodes (RIGHT)
| ↓
| RIGHT BREAST lymphatics / contralateral axilla
|
└── Pre-sternal skin lymphatics
↓
Direct to RIGHT subareolar plexus
↓
RIGHT BREAST
Clinical Importance in Breast Cancer
-
Medial quadrant tumors are more likely to drain to internal mammary nodes and therefore have a higher risk of contralateral spread - they may be understaged if only the axilla is assessed.
-
Contralateral axillary node metastasis is classified as distant disease (M1) in the AJCC TNM staging system, not regional disease - Mulholland and Greenfield's Surgery 7e
-
After sentinel lymph node biopsy (SLNB) or axillary dissection, altered lymphatic drainage can redirect lymph to the contralateral axilla or internal mammary nodes as alternative routes - Current Surgical Therapy 14e
-
Radiocolloid mapping (99mTc sulfur microcolloid scintigraphy) used in sentinel node mapping can sometimes reveal unexpected drainage to the contralateral axilla, especially in medial or central breast tumors.
-
Internal mammary node involvement (via the cross-midline parasternal route) has important prognostic and radiotherapy planning implications - the internal mammary chain is included in regional nodal irradiation protocols for this reason.
Key Anatomical Points to Remember
- The subareolar (Sappey's) plexus is the central hub of all breast lymphatic drainage
- Medial breast drains preferentially to internal mammary nodes (main contralateral pathway)
- Lateral breast drains preferentially to axillary nodes
- The pre-sternal dermis contains lymphatics that freely communicate across the midline
- Parasternal nodes on both sides are connected by trans-sternal anastomoses
- Contralateral spread is a minor route under normal flow but becomes clinically relevant when primary routes are blocked (e.g., post-surgery, post-radiation, or by tumor obstruction)
This is a shared conversation. Sign in to Orris to start your own chat.