Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough, textbook-based answer. Here is the complete discussion:
Case Scenario 4: Endometrial Carcinoma - Full Discussion
1. Most Likely Diagnosis
Endometrial adenocarcinoma - Type I (Endometrioid adenocarcinoma, Grade 1)
The biopsy confirms this. The clinical picture is textbook Type I disease: a postmenopausal woman with the classic triad of obesity, diabetes mellitus, and hypertension presenting with painless postmenopausal bleeding, an enlarged uterus, and a thickened endometrium (14 mm - well above the 4-5 mm threshold used in postmenopausal women).
2. Risk Factors
All risk factors relate to prolonged unopposed estrogen stimulation of the endometrium:
| Risk Factor | Present in This Patient |
|---|---|
| Obesity | Yes - peripheral conversion of androgens to estrogen in adipose tissue |
| Type 2 diabetes mellitus | Yes |
| Hypertension | Yes |
| Nulliparity | Not mentioned, possibly present |
| Late menopause | Not applicable here |
| Anovulatory cycles / PCOS | Common in obese patients |
| Estrogen therapy without progestin | Not present (protective factor absent) |
| Estrogen-producing ovarian tumor | Needs to be excluded |
| Tamoxifen use | Not mentioned |
The association with obesity, hypertension, and diabetes is so consistent that these are sometimes called the "endometrial cancer triad." As noted in Robbins, Cotran & Kumar - Pathologic Basis of Disease: obesity, hypertension, and type 2 diabetes commonly co-occur with endometrial carcinoma because they all link back to the same metabolic milieu of hyperestrogenism.
3. Role of Unopposed Estrogen in Pathogenesis
This is the central mechanism of Type I endometrial carcinoma:
Normal state: Estrogen stimulates endometrial glandular proliferation. Progesterone (produced after ovulation in the luteal phase) counteracts this by inducing secretory differentiation and limiting proliferation.
Unopposed estrogen state:
- In obesity, adipose tissue contains the enzyme aromatase, which converts adrenal androgens (androstenedione) into estrone - a biologically active estrogen. Obese postmenopausal women therefore have persistently elevated circulating estrogen with no balancing progesterone (since they are anovulatory/postmenopausal).
- This drives continuous proliferation of the endometrial glands.
- Over time, the proliferating epithelium accumulates somatic mutations (in PTEN, KRAS, PIK3CA, ARID1A, MLH1, etc.), progressing stepwise:
Normal endometrium → Simple hyperplasia → Complex hyperplasia → Atypical complex hyperplasia (the true precursor) → Endometrioid carcinoma
- PI3K/AKT signaling, which is augmented by estrogen receptor-dependent pathways, is the molecular hallmark of endometrioid carcinoma. Multiple successive mutations in PTEN, PIK3CA, and KRAS all converge on this pathway, progressively amplifying proliferative signaling.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 933
4. Precursor Lesions of Endometrial Carcinoma
The established precursor to Type I (endometrioid) carcinoma is:
Endometrial Hyperplasia - classified by cytologic atypia:
| Classification | Risk of Progression to Carcinoma |
|---|---|
| Hyperplasia without atypia | Low (~1-3%) |
| Atypical (complex) hyperplasia | High (~25-50%) |
- Atypical complex hyperplasia (EIN - Endometrial Intraepithelial Neoplasia) is the recognized direct precursor. Studies of hysterectomy specimens containing both atypical hyperplasia and carcinoma show identical mutations in PTEN, ARID1A, PIK3CA, and KRAS in both components - confirming the precursor relationship and the fact that mutations begin before overt carcinoma is present.
For Type II (serous) carcinoma:
- The precursor is Serous Endometrial Intraepithelial Carcinoma (SEIC) - a noninvasive lesion arising on a background of atrophic endometrium (the opposite of Type I), with early TP53 mutations.
- Robbins & Kumar Basic Pathology; Berek & Novak's Gynecology, p. 2173
5. Treatment for Early-Stage Disease
This patient has Grade 1 endometrioid carcinoma - which is early-stage, low-grade disease with an excellent prognosis (5-year survival >85%).
Standard Treatment: Surgical Staging + Hysterectomy
-
Total extrafascial hysterectomy + bilateral salpingo-oophorectomy (BSO)
- This is the cornerstone of treatment for Stage I disease.
- Radical hysterectomy does NOT improve survival over simple hysterectomy + BSO and adds unnecessary morbidity - it should not be performed for apparent early disease.
-
Surgical staging - includes:
- Peritoneal washings
- Pelvic and para-aortic lymph node assessment (sentinel node biopsy is now standard)
- Inspection for peritoneal/adnexal metastases
- Lymph node involvement defines Stage IIIC disease
-
Approach:
- Minimally invasive surgery (laparoscopic or robotic-assisted) is preferred, especially in obese patients (like this patient), and shows equivalent oncologic outcomes to laparotomy (GOG trial: 3-year recurrence 11.4% laparoscopy vs. 10.2% open; 5-year survival 90% in both arms).
Adjuvant Therapy by Risk Category (Stage I):
| Risk Group | Adjuvant Treatment |
|---|---|
| Low-grade (G1-2), superficial invasion (<50% myometrium) | Observation only after surgery |
| High-grade (G3) or deep invasion (>50%, Stage IB) | Intravaginal brachytherapy |
| Node-positive (Stage IIIC) | Immunochemotherapy |
For this patient (Grade 1, likely Stage IA), observation after total hysterectomy + BSO is the expected recommendation, provided surgical staging confirms no deep invasion or nodal involvement.
All endometrial cancers should be routinely tested for microsatellite instability (MSI) - MSI-high tumors (often associated with Lynch syndrome) respond to PD-1 checkpoint inhibitors when recurrent or advanced.
- Harrison's Principles of Internal Medicine 22E, p. 758; Berek & Novak's Gynecology; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 934
Histopathology Grades (for reference):
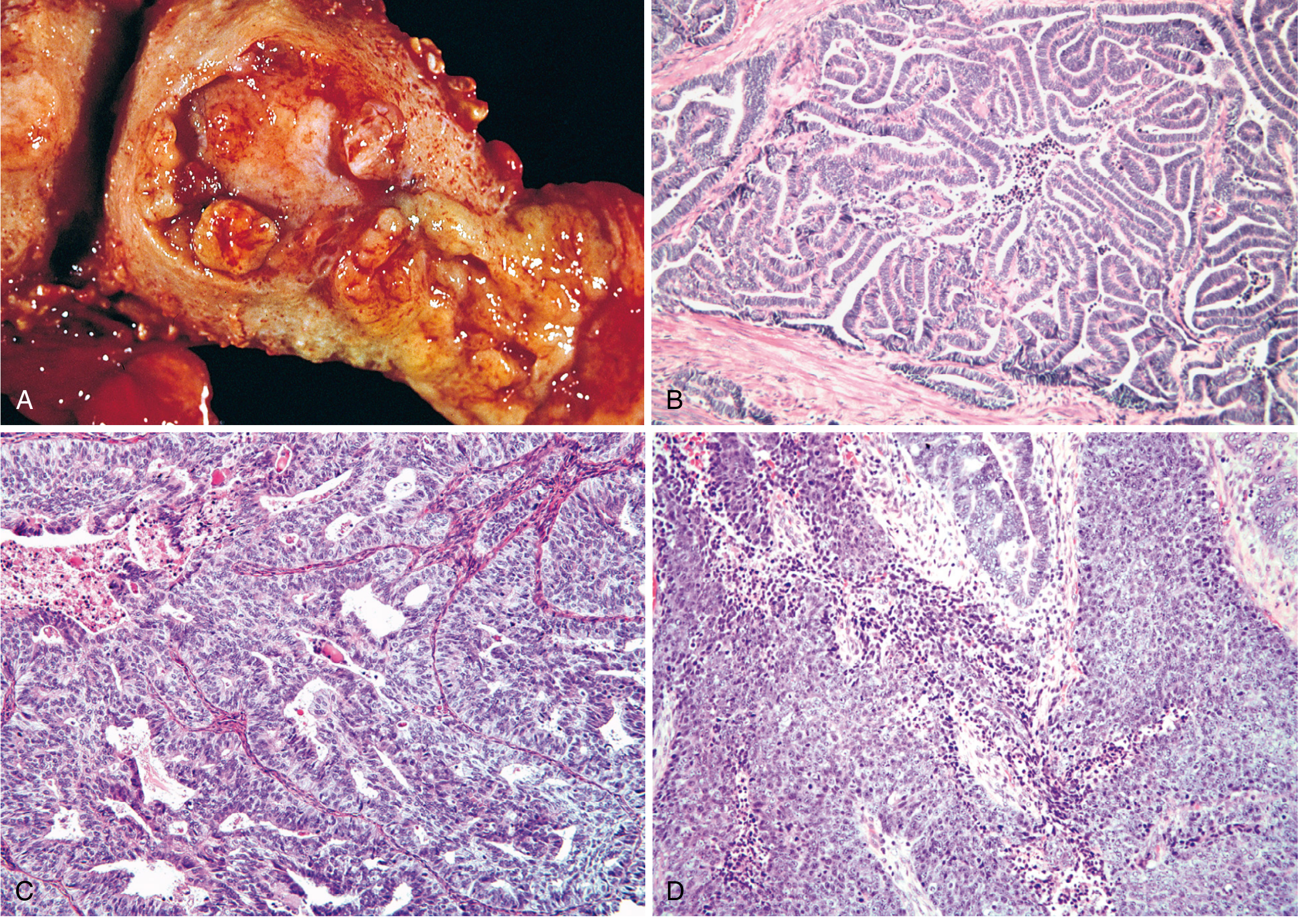
Fig. 22.24 from Robbins, Cotran & Kumar - Endometrioid carcinoma grades. (A) Fungating mass in fundus. (B) Grade 1: well-formed glands, no solid areas. (C) Grade 2: glandular + solid (≤50% solid). (D) Grade 3: >50% solid growth pattern.
This patient's biopsy shows Grade 1 - corresponding to panel B above - which carries the best prognosis.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have all the information needed from authoritative sources. Here is the complete answer:
Clinical Scenario 5: Endometrial Carcinoma - Full Discussion
Case Summary
A 62-year-old postmenopausal woman with nulliparity, 6 years of tamoxifen therapy for breast cancer, presenting with intermittent vaginal bleeding x 3 months + watery discharge. Investigations: Hb 9.8 g/dL, endometrial thickness 16 mm with irregular lining on TVUS, biopsy showing endometrioid adenocarcinoma, MRI confirming tumor confined to uterus with <50% myometrial invasion (Stage IA) and no lymphadenopathy.
1. Most Likely Diagnosis
Endometrial adenocarcinoma - Type I (Endometrioid), FIGO Stage IA
The MRI finding of tumor confined to the uterus with less than 50% myometrial invasion defines FIGO Stage IA disease. This is the most favorable stage and carries an excellent prognosis (5-year survival >85%).
2. Risk Factors Present in This Patient
This patient has multiple, stacked risk factors - all related to prolonged unopposed estrogen stimulation:
| Risk Factor | Relative Risk | Present? |
|---|---|---|
| Nulliparity | 2-3x | Yes |
| Tamoxifen therapy | 2-3x | Yes - 6 years |
| Obesity (implied by context, not stated) | 3-10x | Not specified |
| Diabetes mellitus | 2.8x | Not stated |
| Late menopause | 2.4x | Menopause at age 50 - borderline |
The two key risk factors in this particular case are:
Nulliparity
Nulliparous women have 2-3 times the risk of parous women. Infertility and anovulatory cycles mean prolonged estrogen exposure without sufficient progesterone counterbalance throughout the reproductive years. - Berek & Novak's Gynecology, p. 2144
Tamoxifen Therapy (6 years)
Tamoxifen is a selective estrogen receptor modulator (SERM) - it acts as an estrogen antagonist in breast tissue but as an estrogen agonist in the endometrium. Long-term tamoxifen use for breast cancer is associated with a 2-3 fold increased risk of endometrial cancer. This risk is particularly significant in postmenopausal women and correlates with duration of use. It promotes endometrial polyps, hyperplasia, and carcinoma. - Berek & Novak's Gynecology, p. 2144; Lippincott Pharmacology
Note: Raloxifene (another SERM) does not carry this risk, as it lacks estrogenic activity in the endometrium.
3. Why is Postmenopausal Bleeding an Important Warning Symptom?
Postmenopausal bleeding (PMB) is defined as any uterine bleeding occurring 12+ months after the last menstrual period. It is considered a red flag symptom because:
-
High association with endometrial malignancy: Approximately 10% of women with PMB have endometrial carcinoma. In women with additional risk factors (as in this case), this probability is significantly higher.
-
Endometrium should be quiescent: After menopause, estrogen levels drop and the endometrium becomes atrophic. Any bleeding indicates abnormal stimulation - either from a hormonal source, an anatomic lesion, or malignancy.
-
Early presentation of cancer: Endometrial carcinoma fortunately tends to cause bleeding early (even before deep invasion), making PMB a useful early warning. Most women present at Stage I, contributing to the relatively good overall prognosis of this cancer.
-
Other causes must also be excluded: Atrophic vaginitis (most common), endometrial polyps, submucosal fibroids, and exogenous estrogen use - but malignancy must always be ruled out first.
All postmenopausal women with any vaginal bleeding should be evaluated for endometrial cancer with pelvic examination, transvaginal ultrasound, and endometrial biopsy. - Washington Manual of Medical Therapeutics
4. Role of Transvaginal Ultrasonography (TVUS) in Evaluating PMB
TVUS is the first-line imaging investigation in a woman presenting with postmenopausal bleeding. Its roles are:
Endometrial Thickness Measurement
- In postmenopausal women not on HRT, a normal endometrial stripe should be ≤4 mm.
- Thickness >4-5 mm requires further investigation (endometrial biopsy).
- In women on tamoxifen, the threshold is less clear because tamoxifen causes subendometrial changes that artificially thicken the apparent endometrial stripe; biopsy is recommended regardless of thickness in symptomatic tamoxifen users.
- This patient's 16 mm with irregular lining is markedly abnormal and strongly suspicious for malignancy.
- Meta-analysis data show that 96% of women with endometrial cancer had an endometrial stripe >5 mm on TVUS. - Swanson's Family Medicine Review
Additional TVUS Findings
- Endometrial morphology: irregular, heterogeneous, polypoid lesions raise suspicion
- Myometrial invasion: can be estimated (though MRI is superior for this)
- Adnexal masses or ovarian pathology
- Uterine size and contour
Limitations
- Cannot definitively diagnose or grade endometrial carcinoma - tissue biopsy is still required
- Limited in obese patients (transvaginal approach improves this)
- Tamoxifen users have subendometrial cysts that make thickness measurement unreliable
5. Gold Standard Investigation for Confirming the Diagnosis
The gold standard for confirming endometrial carcinoma is endometrial biopsy (tissue histopathology).
Methods:
-
Office endometrial aspiration/pipelle biopsy - first-line, outpatient procedure
- Sensitivity ~90% for endometrial carcinoma when adequate tissue obtained
- Accepted as the standard first step in evaluating abnormal uterine bleeding
- - Berek & Novak's Gynecology (KEY POINTS)
-
Hysteroscopy-directed biopsy / D&C (dilatation and curettage)
- Performed when office biopsy is inadequate, inconclusive, or technically difficult
- Hysteroscopy allows direct visualization of the endometrial cavity
- More sensitive than blind sampling
What Biopsy Provides:
- Histological type (endometrioid, serous, clear cell, etc.)
- Grade (G1 = well differentiated, G2 = moderate, G3 = poorly differentiated)
- Presence of atypical features or precursor lesions
This patient's biopsy confirmed endometrioid adenocarcinoma - the most common type (~80-85% of cases).
Role of MRI (Staging Imaging - Not Diagnostic)
After tissue diagnosis, MRI pelvis is the preferred imaging for surgical planning because it accurately assesses:
- Depth of myometrial invasion (<50% = Stage IA vs. ≥50% = Stage IB)
- Cervical stromal invasion (Stage II)
- Parametrial/adnexal involvement (Stage III)
- Lymph node status
This patient's MRI confirmed Stage IA with no lymphadenopathy - critical for treatment planning.
6. Standard Treatment for This Stage (FIGO Stage IA Endometrioid Carcinoma)
Primary Treatment: Surgery
Total extrafascial hysterectomy + bilateral salpingo-oophorectomy (BSO) with surgical staging
This is the cornerstone of treatment. For this patient (Stage IA, Grade 1-2 endometrioid), the standard components are:
- Total hysterectomy + BSO - removes the primary tumor and eliminates the source of estrogen (ovaries)
- Peritoneal washings for cytology
- Sentinel lymph node biopsy (now standard at most centers) - provides staging without full lymphadenectomy
- Lymph node involvement upgrades to Stage IIIC and mandates systemic therapy
Radical hysterectomy (with parametrial resection) does not improve survival over simple hysterectomy in Stage I disease and should NOT be performed. - Berek & Novak's Gynecology, p. 2176
Surgical Approach
- Minimally invasive (laparoscopic or robotic-assisted) is preferred
- Equivalent oncologic outcomes to open surgery (GOG trial: 5-year survival 90% in both arms)
- Robotic approach is especially useful in obese patients, offering reduced blood loss, shorter hospital stay, and higher lymph node yields
Adjuvant Therapy by Risk (Stage IA):
| Risk Group | Adjuvant Therapy |
|---|---|
| Stage IA, Grade 1-2, no LVSI | Observation only - no adjuvant therapy needed |
| Stage IA, Grade 3 or LVSI present | Intravaginal brachytherapy (VBT) |
| Stage IB | Vaginal brachytherapy ± external beam radiation |
| Stage II+ | External beam pelvic radiation ± chemotherapy |
| Stage III-IV | Systemic chemotherapy (carboplatin + paclitaxel) ± immunotherapy |
For this patient (Stage IA, <50% myometrial invasion), observation after surgery is the expected standard - no adjuvant radiation or chemotherapy is needed. - Washington Manual of Medical Therapeutics, p. 855
Important Additional Considerations:
- Stop tamoxifen - this is essential. She should be switched to an aromatase inhibitor for her breast cancer (which, unlike tamoxifen, reduces endometrial stimulation).
- MSI/MMR testing: All endometrial cancers should now routinely be tested for microsatellite instability. MSI-high tumors (Lynch syndrome or sporadic) qualify for pembrolizumab (PD-1 inhibitor) if recurrence occurs.
- Her anemia (Hb 9.8 g/dL) from chronic blood loss should be addressed preoperatively.
Summary Table
| Feature | This Patient |
|---|---|
| Diagnosis | Endometrioid adenocarcinoma |
| FIGO Stage | IA (<50% myometrial invasion, confined to uterus) |
| Key Risk Factors | Nulliparity, 6-year tamoxifen use |
| Diagnostic Gold Standard | Endometrial biopsy (histopathology) |
| TVUS Threshold for Concern | >4-5 mm (this patient: 16 mm - markedly elevated) |
| Primary Treatment | Total hysterectomy + BSO + surgical staging (minimally invasive preferred) |
| Adjuvant Therapy | Observation only (Stage IA, low-grade) |
| Additional Action | Discontinue tamoxifen; switch to aromatase inhibitor |
This is a shared conversation. Sign in to Orris to start your own chat.