Acute correction of hyponatrimia
Reading File
Finding Sources
Finding Sources
Searching PubMed
hyponatremia treatment correction guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent content from multiple authoritative sources. Let me compile the full, comprehensive answer.
Acute Correction of Hyponatremia
Hyponatremia (serum Na+ < 135 mEq/L) is the most common electrolyte disorder. Acute correction refers to raising serum sodium in a timely, controlled fashion - urgency and rate depend on symptom severity and duration of hyponatremia.
Key Principle: Symptom-Driven Approach
Treatment is guided primarily by neurologic symptomatology, not just the serum sodium level or chronicity (though duration matters). The central risk trade-off is:
- Under-correction of acute hyponatremia → fatal cerebral edema and brain herniation
- Over-correction of chronic hyponatremia → osmotic demyelination syndrome (ODS)
Classification by Duration
| Type | Definition | Primary Danger |
|---|---|---|
| Acute | Developed within < 48 hours | Cerebral edema, herniation |
| Chronic | Developed over > 48 hours or unknown duration | ODS if corrected too fast |
Management Algorithm
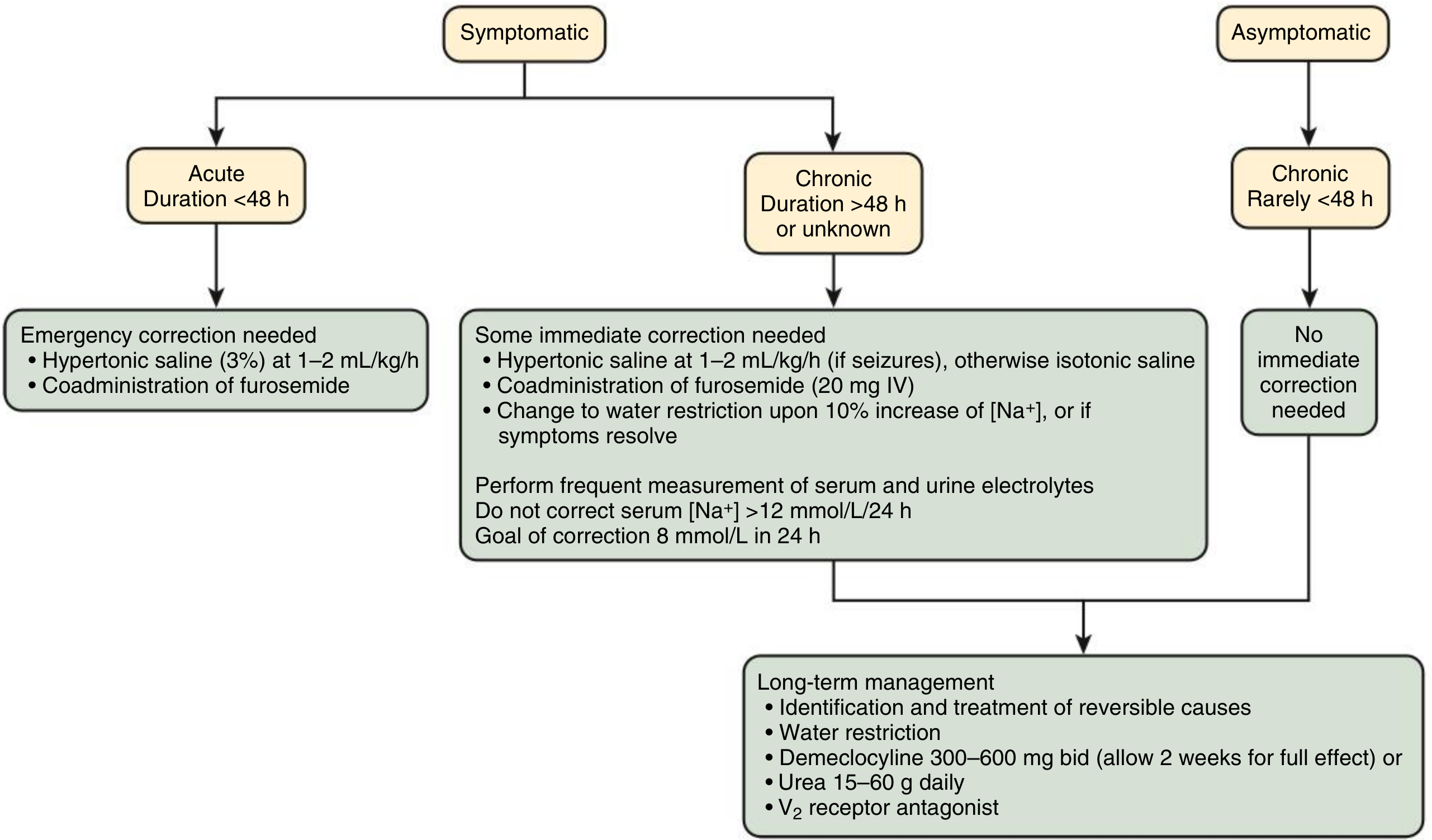
1. Acute Symptomatic Hyponatremia (< 48 hours)
These patients are at immediate risk of cerebral edema and brain herniation. The risk of acute cerebral edema far exceeds the risk of ODS, so prompt correction is mandatory.
Clinical Features Demanding Emergency Treatment
- Severe symptoms: coma, obtundation, seizures, respiratory distress/arrest
- Moderate symptoms: altered mental status, confusion, unexplained nausea, gait instability
Treatment: Hypertonic (3%) Saline
3% NaCl (Na+ = 513 mEq/L) is the first-line agent.
Two approaches:
A. Bolus method (preferred for severe/acute symptoms):
- 100 mL of 3% NaCl IV over 10 minutes
- May repeat ×2 (every 10 minutes) if no clinical improvement
- Each 100 mL bolus raises serum Na+ by approximately 2-4 mEq/L
- A rapid increment of 4-6 mmol/L within the first 6 hours is sufficient to reverse cerebral edema; correction to normal is unnecessary
B. Continuous infusion method:
- Rate estimation formula (Brenner & Rector):
Patient weight (kg) × desired correction rate (mEq/L/h) = infusion rate of 3% NaCl (mL/h)
- For severe neurologic symptoms (seizures, coma): 4-6 mL/kg/h
- For mild-moderate symptoms: 0.5-2 mL/kg/h or 1-2 mL/kg/h
Coadminister furosemide (20 mg IV) - enhances free water excretion and hastens normalization of serum Na+.
Monitor: serum electrolytes every 1-2 hours until goal is met.
- Comprehensive Clinical Nephrology, 7th ed., p. 149
- Brenner and Rector's The Kidney, p. 675
2. Chronic Symptomatic Hyponatremia (> 48 hours or unknown)
Brain astrocytes have had time to extrude osmols and lower intracellular osmolality (brain volume regulation). This adaptive response means:
- Correction must be slower and more cautious
- Rapid correction renders serum hypertonic relative to astrocytes → water efflux → cytoskeletal and DNA damage → ODS
Treatment Goals (Chronic Hyponatremia)
| Parameter | Target | Maximum Limit |
|---|---|---|
| Daily correction | 4-6 mEq/L/day | ≤ 6-8 mEq/L/24 h |
| Safe upper limit (most guidelines) | 8 mmol/L in 24 h | ≤ 12 mEq/L/24 h |
| Asymptomatic/mild | 0.5 mEq/L/h | Max 12 mEq/L/day |
If seizures are present in chronic hyponatremia: Use 3% NaCl at 1-2 mL/kg/h; otherwise isotonic saline.
Switch to water restriction upon achieving a 10% increase in [Na+] or when symptoms resolve.
- Symptom to Diagnosis, 4th ed., Table 24-2
- Comprehensive Clinical Nephrology, 7th ed., p. 149
3. Sodium Deficit Formula
The Adrogue-Madias formula estimates how much sodium is needed:
Sodium deficit (mEq) = TBW × (desired Na+ - current Na+) TBW = 0.6 × weight (kg) in men; 0.5 × weight in women
This is a starting estimate - frequent monitoring and titration are always required.
4. Choice of IV Fluid by Volume Status
| Volume Status | First-line Fluid | Rationale |
|---|---|---|
| Hypovolemic (depleted) | Isotonic (0.9%) NaCl | Restore ECF volume; urine Na+ usually < 20-30 mEq/L |
| Euvolemic (SIADH) | 3% NaCl (symptomatic) or fluid restriction | Isotonic saline may worsen SIADH hyponatremia |
| Hypervolemic (HF, cirrhosis) | Avoid saline; diuretics + fluid/Na restriction | Adding Na+ worsens volume overload |
- Brenner and Rector's The Kidney, p. 676
5. Osmotic Demyelination Syndrome (ODS) - Key Warning
ODS is the most feared complication of hyponatremia management.
Risk factors for ODS:
- Serum Na+ ≤ 120 mEq/L (especially ≤ 105 mEq/L) for > 48 hours
- Hypovolemic or diuretic-associated hyponatremia
- Hypokalemia, alcohol abuse, malnutrition, advanced liver disease
- Vaptans, treated cortisol deficiency
Clinical features (develop 2-6 days after correction):
- Spastic quadriparesis, pseudobulbar palsy (dysarthria, dysphagia, diplopia)
- Coma, seizures, movement disorders, ataxia, death
- MRI lesions may not appear for up to 4 weeks after symptoms begin
Reversal if overcorrection occurs:
-
Desmopressin 2-4 mcg IV every 8 hours +
-
D5W 3 mL/kg IV over 1 hour (repeat until Na+ within safe range)
-
Stop any vaptans
-
Monitor Na+ hourly
-
Symptom to Diagnosis, 4th ed., Table 24-3
6. Severity Classification and Treatment Summary
| Symptom Level | Clinical Features | Approach |
|---|---|---|
| Severe | Seizures, coma, respiratory arrest | Immediate 3% NaCl bolus (100 mL over 10 min × up to 3 doses) |
| Moderate | Confusion, gait instability, nausea | 3% NaCl at lower rate (0.5-2 mL/kg/h); monitor closely |
| Mild/Absent | Headache, irritability, mood change | Cautious treatment; fluid restriction; address etiology |
7. Special Scenarios
Acute hyponatremia in postoperative patients / marathon runners / MDMA use: High-risk for rapid progression to seizures and brain herniation - treat aggressively with 3% NaCl even if only moderate symptoms. Female patients are at higher risk due to hormonal inhibition of the brain volume adaptive response.
SIADH: Fluid restriction is first-line for chronic mild-moderate cases; vaptans (tolvaptan, conivaptan) are second-line options but carry high ODS risk with overcorrection and should be used cautiously.
Recent Evidence (2024-2026)
Two recent systematic reviews are relevant to current practice:
- Ayus et al. (JAMA Intern Med, 2025) - examined correction rates and clinical outcomes in hospitalized adults with severe hyponatremia [PMID: 39556338]. Evidence suggests outcomes data on optimal correction rates.
- Schneider et al. (J Gen Intern Med, 2026) - reviewed outcomes with sodium overcorrection in chronic hyponatremia [PMID: 41652262]. These findings may refine the currently recommended 10-12 mEq/L/24 h upper limit.
⚠️ These recent meta-analyses (2025-2026) may update or refine existing correction rate thresholds. Consult the full papers for the latest guidance if clinical decisions are at stake.
Sources:
- Brenner and Rector's The Kidney, 2-Volume Set, pp. 674-679
- Comprehensive Clinical Nephrology, 7th Edition, pp. 149-150
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed., Tables 24-2 and 24-3
Acute correction of hyponatrimia
I already covered this topic in detail just above. Here is a concise structured summary you can reference:
Acute Correction of Hyponatremia - Quick Reference
Core Principle
Treatment is symptom-driven, not solely number-driven. The two competing dangers are:
- Under-correction → cerebral edema, brain herniation (acute hyponatremia)
- Over-correction → osmotic demyelination syndrome / ODS (chronic hyponatremia)
Step 1: Is it Acute (< 48 h) or Chronic (> 48 h / unknown)?
| Duration | Primary Risk | Urgency |
|---|---|---|
| Acute < 48 h | Cerebral edema / herniation | Treat aggressively |
| Chronic > 48 h or unknown | ODS if corrected too fast | Treat cautiously |
Step 2: Severity of Symptoms
| Level | Symptoms | Action |
|---|---|---|
| Severe | Seizures, coma, respiratory arrest | Emergency - bolus 3% NaCl now |
| Moderate | Confusion, gait instability, nausea | Urgent - infuse 3% NaCl at lower rate |
| Mild / None | Headache, irritability, mood changes | Cautious - fluid restrict, treat cause |
Step 3: Treatment by Scenario
Acute Symptomatic (< 48 h) - Aggressive Correction
Drug of choice: 3% NaCl (hypertonic saline)
-
Bolus method (severe symptoms - seizures, coma):
- 100 mL of 3% NaCl IV over 10 minutes
- Repeat ×2 (every 10 min) if no improvement
- Each 100 mL bolus raises Na+ by ~2-4 mEq/L
- Target: raise Na+ by 4-6 mEq/L within first 6 hours - enough to reverse cerebral edema
-
Infusion method (moderate symptoms):
- Rate = weight (kg) × desired correction rate (mEq/L/h) = mL/h of 3% NaCl
- Severe neuro symptoms: 4-6 mL/kg/h
- Mild-moderate: 0.5-2 mL/kg/h
-
Add furosemide 20 mg IV to enhance free water excretion
-
Check electrolytes every 1-2 hours
Chronic Symptomatic (> 48 h) - Cautious Correction
| Goal | Rate |
|---|---|
| Target correction | 4-6 mEq/L/day |
| Safe maximum | ≤ 8 mEq/L/24 h (most guidelines) |
| Hard ceiling | ≤ 10-12 mEq/L/24 h (never exceed) |
- If seizures present: 3% NaCl at 1-2 mL/kg/h temporarily
- Otherwise: isotonic saline (if hypovolemic) or fluid restriction (if euvolemic/SIADH)
- Switch to fluid restriction once Na+ rises by 10% or symptoms resolve
Step 4: Fluid Choice by Volume Status
| Volume Status | IV Fluid | Why |
|---|---|---|
| Hypovolemic | 0.9% (isotonic) NaCl | Restore ECF volume |
| Euvolemic (SIADH) | 3% NaCl if symptomatic; fluid restrict otherwise | Isotonic saline can worsen SIADH |
| Hypervolemic (HF, cirrhosis) | No saline; diuretics + restrict Na+ and water | Saline worsens volume overload |
Sodium Deficit Formula
Na+ deficit (mEq) = TBW × (target Na+ - current Na+) TBW = 0.6 × weight (kg) men | 0.5 × weight (kg) women
Use only as a starting estimate - always titrate based on repeated measurements.
ODS (Osmotic Demyelination Syndrome) - Danger of Overcorrection
Highest risk: Na+ ≤ 105 mEq/L, chronic duration, liver disease, alcoholism, malnutrition, hypokalemia
Symptoms (appear 2-6 days after overcorrection): quadriparesis, dysarthria, dysphagia, coma, seizures - MRI may be negative for up to 4 weeks
Reversal if overcorrection detected:
- Desmopressin 2-4 mcg IV every 8 h
- D5W 3 mL/kg IV over 1 hour - repeat until Na+ back within safe range
- Stop vaptans; monitor Na+ hourly
Special High-Risk Groups for Acute Hyponatremia
- Postoperative patients (receiving hypotonic fluids)
- Marathon runners, MDMA/ecstasy use, psychogenic polydipsia
- Females (hormones inhibit brain volume adaptation)
- These groups can deteriorate rapidly - treat aggressively even with moderate symptoms
Sources: Brenner & Rector's The Kidney | Comprehensive Clinical Nephrology, 7th ed. | Symptom to Diagnosis, 4th ed. | Recent meta-analyses: Ayus et al. JAMA Intern Med 2025 [PMID: 39556338]; Schneider et al. J Gen Intern Med 2026 [PMID: 41652262]
Acute correction of hyponatrimia in neonates
Reading File
Finding Sources
Finding Sources
Searching PubMed
hyponatremia neonate treatment correction
Finding Sources
Finding Sources
Searching PubMed
hyponatremia neonate newborn sodium
Finding Sources
Finding Sources
Reading Article
PMID: 21942597
Reading Article
PMID: 25155728
Finding Sources
Reading Article
PMID: 37115978
Searching the Web
acute hyponatremia correction neonates 3% NaCl dose rate guidelines NICU
Finding Sources
Reading Web Page
https://www.anmfonline.org/wp-content/uploads/2021/06/sodium…
I now have comprehensive neonatal-specific data from multiple authoritative neonatal clinical guidelines. Let me compile the full answer.
Acute Correction of Hyponatremia in Neonates
Important caveat: The evidence base for neonatal hyponatremia treatment is limited. Most recommendations are expert-consensus extrapolated from adult guidelines, adjusted for neonatal physiology. Always involve a Neonatologist before initiating 3% NaCl.
Definition in Neonates
| Severity | Serum Sodium |
|---|---|
| Mild hyponatremia | 130-134 mEq/L |
| Moderate | 125-129 mEq/L |
| Severe | < 125 mEq/L |
| Late-onset hyponatremia (premature) | ≤ 132 mEq/L (or 133-135 if on Na+ supplementation) |
Normal neonatal serum sodium: 135-145 mEq/L
Why Neonates Are Different
1. Higher total body water (TBW):
- Adults/older children: TBW = weight × 0.6
- Neonates/newborns: TBW = weight × 0.75 (must use this in all calculations)
2. Immature kidneys:
- Low GFR, tubular immaturity, impaired sodium conservation
- High extrarenal fluid losses (especially in preterm infants)
- Cannot concentrate or dilute urine effectively
3. Active brain myelination:
- Rapid correction during brain myelination carries a higher risk of neurological damage
- Correction ≥ 0.5 mmol/L/h in neonates has shown a trend toward higher rates of abnormal neurological examination and IVH/PVL
- ODS (osmotic demyelination) risk exists, though classical "central pontine myelinolysis" is less well-described in neonates than adults
4. Common neonatal-specific causes:
- Excess free water from hypotonic IV fluids
- Acute kidney injury / oliguric renal failure
- SIADH (perinatal asphyxia, meningitis, IVH, pneumothorax, pneumonia, opioids)
- Adrenal insufficiency / congenital adrenal hyperplasia (CAH)
- Late-onset hyponatremia of prematurity (inadequate Na+ intake + renal wasting)
- Dilutional hyponatremia from excessive breast milk or maternal hyponatremia
Indications for Acute (Active) IV Correction
Active IV correction with 3% NaCl is reserved for:
- Symptomatic hyponatremia regardless of level (seizures, apnea, altered tone, coma)
- Severe hyponatremia: serum Na+ < 120 mmol/L even if currently asymptomatic
- Requires Neonatologist approval - this is a HIGH RISK medication in the neonate
Treatment must always be tailored to the cause. Fluid restriction - not sodium supplementation - is appropriate for dilutional/SIADH hyponatremia.
Drug: 3% NaCl (Hypertonic Saline) - Neonatal Protocol
Concentration: 3% NaCl = 0.513 mmol Na+ per mL | Osmolarity: 1027 mOsmol/L
Step 1: Calculate Sodium Deficit
Formula (CHEO / PedMed neonatal formulary):
Na+ deficit (mmol) = [desired Na+ - actual Na+] × 0.7 L/kg × weight (kg)
- For acute correction, use desired Na+ = 125 mmol/L (not full correction to normal)
- TBW factor in neonates = 0.7 L/kg (some protocols use 0.75)
Convert mmol to mL of 3% NaCl:
Volume (mL) = Na+ deficit (mmol) ÷ 0.513 mmol/mL
Maximum volume cap: 6 mL/kg
Step 2: Infusion Rate by Clinical Status
| Clinical Status | Dose / Rate | Goal |
|---|---|---|
| Symptomatic (seizures, apnea, coma) | 1-3 mL/kg of 3% NaCl over 15 minutes (KEMH) OR 0.5 mmol/kg/h (1 mL/kg/h) (ANMF) | Stop when symptoms abate or Na+ ≥ 120 mmol/L |
| Asymptomatic, severe (Na+ < 120) | 1-2 mL/kg/h (0.5-1 mmol/kg/h) max | Slow correction to 125 mmol/L |
| After initial stabilization | 0.15 mmol/kg/h (slow maintenance rate) | Gradual correction over 24-48 h |
Alternative KEMH fast-correction rate:
- 3% NaCl at 2 mL/kg/hour raises serum Na+ by approximately 2 mmol/L/hour
Step 3: Correction Rate Targets (Neonatal)
| Timeframe | Target Rise | Maximum Limit |
|---|---|---|
| First 1-6 hours (acute/symptomatic) | 1-2 mmol/L/h until symptoms stop or Na+ ≥ 120 | Stop active correction once safe level reached |
| First 24 hours (after stabilization) | 6-8 mmol/L | ≤ 8 mmol/L/24 h |
| 48 hours | 12-14 mmol/L total | - |
| 72 hours | 14-16 mmol/L total | - |
Hyponatremic seizures usually stop with a correction of only 3-5 mmol/L - do not push for full normalization acutely.
Never exceed 8 mmol/L increase in serum Na+ over 24 hours in neonates - rapid correction can cause brain damage, especially during active myelination.
Administration Route
| Route | Comment |
|---|---|
| Central line (UVC/PICC) | Preferred - if using UVC, confirm tip is NOT in the heart or liver |
| Peripheral IV | Acceptable in emergency; monitor carefully for extravasation and tissue necrosis (osmolarity > 1000 mOsmol/L causes vein damage) |
Monitoring
- Serum electrolytes every 2-4 hours during active correction
- Watch for: fluid overload, pulmonary edema, infusion site extravasation
- Monitor urine output, weight, blood pressure
- Reassess Na+ before giving further correction doses
- Once symptoms resolve and Na+ > 120 mmol/L: switch to slow maintenance correction over 24 hours
Approach by Cause (Neonatal)
| Cause | Treatment |
|---|---|
| SIADH (AKI, asphyxia, meningitis) | Fluid restriction is first-line; 3% NaCl only if symptomatic/severe |
| Sodium deficit (late-onset prematurity) | Oral/enteral Na+ supplementation; 3% NaCl if severe/symptomatic |
| Dilutional (excess hypotonic fluids) | Stop/reduce hypotonic fluids; increase tonicity of IV fluids |
| Adrenal insufficiency / CAH | Hydrocortisone replacement; NaCl supplementation |
| Maternal hyponatremia | Usually self-correcting; monitor closely |
| AKI / oliguric failure | Fluid restriction ± dialysis if refractory |
Special Consideration: Late-Onset Hyponatremia of Prematurity
- Occurs at 2+ weeks of age in premature infants
- Caused by inadequate Na+ intake + renal Na+ wasting
- Risk: poor somatic growth, neurodevelopmental delay, BPD, severe ROP
- Management: primarily enteral/oral sodium supplementation (not IV 3% NaCl), targeting Na+ 135-145 mEq/L
- Spot urine Na+ helps guide therapy (low urine Na+ = total body Na+ deficit)
ODS Risk in Neonates
While classical osmotic demyelination is less documented than in adults, rapid correction in neonates carries neurological risk due to:
- Active brain myelination
- Studies show correction ≥ 0.5 mmol/L/h trends toward higher IVH/PVL and abnormal neurological examinations
- Strict adherence to the ≤ 8 mmol/L/24 h ceiling is mandatory
Summary Protocol Card
Neonate with Na+ < 120 mmol/L OR symptomatic hyponatremia
↓
Involve Neonatologist (mandatory)
↓
Determine cause: SIADH? Na+ deficit? Dilutional? AKI?
↓
Symptomatic (seizures/apnea)?
YES → 3% NaCl 1-3 mL/kg over 15 min (STAT bolus)
Target: stop symptoms / Na+ ≥ 120 mmol/L
Then switch to slow correction
NO (severe, asymptomatic) → 3% NaCl 1-2 mL/kg/h
Calculate: deficit = (125 - actual Na) × 0.7 × kg
Volume (mL) = deficit ÷ 0.513 | Max 6 mL/kg
↓
Check Na+ every 2-4 hours
Limit total rise: ≤ 8 mmol/L in 24 h
Once Na+ > 120 + symptoms gone → slow 24h correction
Sources:
- ANMF Consensus Group - NaCl 3% Newborn Protocol (2021)
- KEMH/Perth Children's Hospital Neonatal Monograph (2020)
- CHEO Neonatal Drug Therapy Manual - NaCl 3% hypertonic
- Marcialis et al. J Matern Fetal Neonatal Med 2011 [PMID: 21942597] - Neonatal hyponatremia: differential diagnosis and treatment
- Bockenhauer & Zieg, Clin Perinatol 2014 [PMID: 25155728] - Electrolyte disorders in neonates
- Marin et al. J Perinat Neonatal Nurs 2023 [PMID: 37115978] - Late-onset hyponatremia in premature infants
This is a shared conversation. Sign in to Orris to start your own chat.