Tracheoesophageal fistula
Reading File
Finding Sources
Searching PubMed
"tracheoesophageal fistula" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Tracheoesophageal Fistula (TEF)
Definition & Embryology
A tracheoesophageal fistula is an abnormal communication between the trachea and esophagus resulting from incomplete division of the cranial foregut into its respiratory and digestive components during the 4th week of gestation. A diverticulum forms off the anterior proximal foregut, and incomplete fusion of the tracheoesophageal folds leads to a defective tracheoesophageal septum. TEF is the most common congenital birth defect of the lower respiratory tract, occurring in approximately 1 in 3,000-4,500 live births, with a slight male predominance.
- The Developing Human: Clinically Oriented Embryology, p. 576
- Schwartz's Principles of Surgery, p. 1744
Anatomic Classification (5 Types)
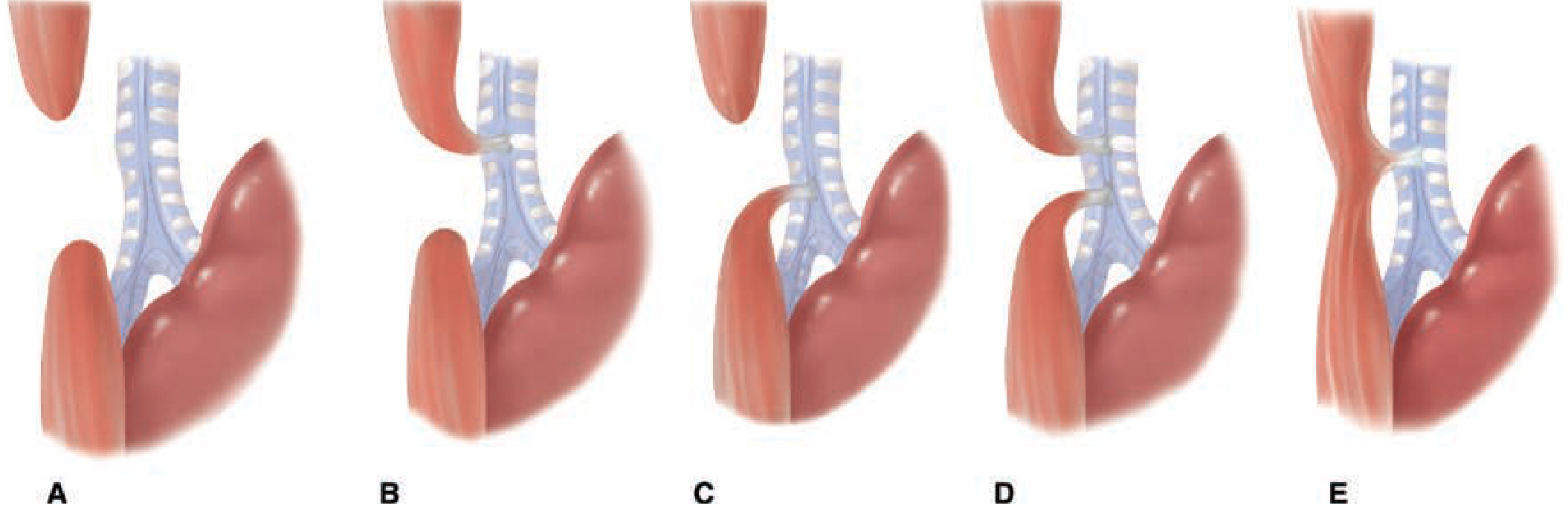
Figure: The five varieties of esophageal atresia (EA) and tracheoesophageal fistula (TEF) - Schwartz's Principles of Surgery
| Type | Description | Frequency |
|---|---|---|
| A | Isolated esophageal atresia (no fistula) | 8-10% |
| B | EA with proximal TEF (proximal esophagus connects to trachea) | ~1% |
| C | EA with distal TEF (most common) - blind upper pouch, lower esophagus connects near carina | ~85% |
| D | EA with both proximal and distal TEF | ~2% |
| E | H-type fistula - TEF without esophageal atresia | ~4% |
- Schwartz's Principles of Surgery, p. 1745
- Tintinalli's Emergency Medicine, p. 3986
Associated Anomalies
TEF occurs in isolation or as part of broader syndromes. Up to 50% of patients have other congenital anomalies, most commonly cardiovascular.
- VACTERL association: Vertebral anomalies, Anal atresia, Cardiac defects, Tracheoesophageal fistula, Esophageal atresia, Renal anomalies, Limb anomalies
- CHARGE syndrome: Coloboma, Heart defects, Atresia choanae, Retardation of growth, Genital/urinary abnormalities, Ear abnormalities
- Specific breakdown in EA-TEF patients:
- Cardiac defects: 38%
- Skeletal defects: 19%
- Neurological defects: 15%
- Renal defects: 15%
- Anorectal defects: 8%
Any child with TEF should undergo echocardiography (to assess for cardiac disease and aortic arch sidedness) and abdominal ultrasound (to detect renal anomalies) prior to surgical repair.
- Schwartz's Principles of Surgery, p. 1745; Miller's Anesthesia, p. 10638
Clinical Presentation
Presentation depends on the anatomic type:
Types A, B, C, D (with esophageal atresia):
- Excessive drooling from birth (unable to swallow secretions)
- Choking/coughing immediately upon feeding
- Cyanotic episodes during nursing
- Abdominal distention (air enters stomach via fistula during crying/coughing)
- Respiratory distress from aspiration - chemical pneumonitis from refluxed gastric acid passing through fistula into the trachea
Type E (H-type, no atresia):
- Presents later in infancy/childhood (esophagus is patent)
- Recurrent respiratory tract infections
- Chronic cough, particularly with feeds
Prenatal clues: Polyhydramnios (fetus cannot swallow amniotic fluid for absorption); failure to visualize the stomach on ultrasound.
- The Developing Human, p. 576; Cummings Otolaryngology, p. 2755
Diagnosis
- Inability to pass an orogastric/NG tube into the stomach - tube coils in the upper pouch (stops 9-13 cm from nares). This is the classic bedside test.
- Chest X-ray: Shows the coiled tube in the upper pouch; gastric bubble confirms a distal fistula (Type C); right upper lobe pneumonia from aspiration is common.
- Contrast esophagram: Diagnostic - demonstrates the fistula and/or atresia. For H-type fistulas, a barium study is particularly useful.
- Endoscopy: Useful as an alternative to contrast studies, especially to avoid aspiration risk.
- Bronchoscopy: Used intraoperatively to confirm fistula size and location before repair.
Important differential: Esophageal perforation from traumatic NG tube insertion - typically occurs at the piriform sinus.
- Schwartz's Principles of Surgery, p. 1745; K.J. Lee's Essential Otolaryngology, p. 1131
Management
Preoperative / Initial Stabilization
- Withhold feeds; maintain upright (head-up, prone) positioning
- Place a Replogle tube (double-lumen sump catheter) in the upper esophageal pouch for continuous low-pressure suction of secretions
- IV fluids, antibiotics if pneumonitis is suspected
- Workup for associated anomalies (echo, abdominal US, spinal films)
Surgical Repair
Definitive repair is rarely an emergency - can proceed within 1-2 days once the infant is stabilized and associated anomalies are assessed.
- Primary anastomosis via right thoracotomy (or thoracoscopy) with ligation of the fistula at the trachea followed by esophageal anastomosis - this is the current standard approach
- Thoracoscopic repair is now the preferred approach in most centers
- Long-gap EA (gap >3 cm, or height of 2 vertebrae) is more challenging and may require:
- Foker technique - external traction sutures to elongate the esophagus prior to anastomosis
- Staged repair: gastrostomy followed by delayed primary anastomosis at ~3 months
- Esophageal substitution: colonic interposition, gastric transposition, or free jejunal graft
Endoscopic Treatment
For H-type fistulas and recurrent/acquired TEFs, endoscopic closure with cauterization or trichloroacetic acid has shown promising early results, though multiple treatments are often needed.
- Schwartz's Principles of Surgery, p. 1745; Cummings Otolaryngology, p. 2762
Anesthetic Considerations
Key challenges during repair:
- Aspiration pneumonitis - compromises baseline respiratory function
- Positive-pressure mask ventilation - forces air through the fistula into the stomach, causing gastric distention that splints the diaphragm and reduces FRC, making ventilation worse
- ETT malplacement - the tube can inadvertently enter the fistula rather than the trachea
Anesthetic strategy:
- Inhalational induction with spontaneous ventilation maintained until fistula is ligated
- Bronchoscopy after induction to assess fistula size and location; a balloon embolectomy catheter may be placed in the fistula to occlude it
- ETT placed distal to the fistula - can be done by advancing into a main bronchus then withdrawing until bilateral air entry is confirmed
- If large fistula or poor lung compliance: urgent transcutaneous gastric decompression or intra-abdominal clamping of the distal esophagus may be needed
- Invasive arterial BP monitoring recommended
- Pre- and post-ductal pulse oximetry to detect intracardiac shunting
Postoperative pain: wound infiltration, caudal catheter threaded to thoracic level, or paravertebral catheter.
- Miller's Anesthesia, pp. 10638-10639
Complications
Early:
- Anastomotic leak
- Esophageal stricture (most common - occurs in ~30-40%)
- Recurrent fistula
Late:
- Esophageal dysmotility
- GERD (very common)
- Tracheomalacia (TM)
- Only ~20% of patients with repaired EA have normal pulmonary function at long-term follow-up (Helsinki study)
Prognosis
Overall survival is 60-80% in uncomplicated cases. Survival drops to approximately 22% when significant cardiac or genitourinary anomalies are present. Historically, virtually all infants with TEF died; survival improved dramatically following Haight's first successful primary anastomosis in Ann Arbor, and has continued to improve with modern neonatal surgical and intensive care.
- K.J. Lee's Essential Otolaryngology, p. 1133; Schwartz's Principles of Surgery, p. 1744
Anaesthetic management of a neonate with tracheoesophageal fistula
Finding Sources
Searching PubMed
"tracheoesophageal fistula" AND "anesthetic management" AND neonate
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive, detailed anaesthesia-specific content from four major textbooks. Let me compile the full answer.
Anaesthetic Management of a Neonate with Tracheoesophageal Fistula
1. Preoperative Assessment
Understanding the Pathophysiology - Why It Matters for Anaesthesia
The major anaesthetic hazards stem directly from the anatomy:
- Aspiration pneumonitis - gastric contents reflux up the distal esophagus and enter the trachea through the fistula; saliva pools in the upper pouch and overflows
- Positive-pressure ventilation (PPV) before fistula ligation - gas preferentially takes the path of least resistance through the fistula into the stomach, causing progressive gastric distention that:
- Splints the diaphragm and reduces functional residual capacity (FRC)
- Makes lung ventilation progressively harder, causing a vicious cycle
- Risk is proportional to fistula size and inversely proportional to lung compliance
- ETT malplacement into the fistula - the fistula orifice is usually on the posterior membranous wall of the trachea, just proximal to the carina; the ETT tip can enter it
- Coexisting congenital heart disease - present in 15-38% of cases; can profoundly alter anaesthetic conduct
Preoperative Workup (Before Anaesthesia)
| Investigation | Rationale |
|---|---|
| Echocardiogram | Exclude congenital heart disease; determine aortic arch sidedness (right arch influences surgical approach) |
| Abdominal ultrasound | Detect major renal anomalies (part of VACTERL) |
| Chest X-ray | Assess degree of aspiration pneumonitis; confirm tube position |
| Plain skeletal X-rays | Vertebral anomalies |
| Electrolytes/blood gas | Dehydration is common due to inability to feed |
| Full blood count + cross-match | Blood must be immediately available |
Optimisation Before Theatre
- Nil by mouth - feeds withheld
- Replogle tube (sump catheter) placed in the upper esophageal pouch on continuous low-pressure suction - prevents aspiration of pooled saliva
- Positioning - nurse upright prone (head-up, prone position) to reduce gastric reflux through the fistula into the trachea
- IV antibiotics if aspiration pneumonitis is present
- IV fluids for hydration and electrolyte correction
- Rarely, if pneumonitis is severe, a gastrostomy under local anaesthesia may be performed first to protect the pulmonary system, followed by delayed definitive repair
Definitive repair is rarely a surgical emergency. If the infant is haemodynamically stable and oxygenating well, repair may proceed within 24-48 hours - this allows time for full anomaly workup and assembly of an experienced team.
- Barash's Clinical Anesthesia, p. 3664-3665; Morgan & Mikhail's Clinical Anesthesiology, p. 1715
2. Monitoring
-
Precordial (or oesophageal) stethoscope placed in the dependent (left) axilla - during right thoracotomy with the infant in the left lateral position, surgical retraction can obstruct the left mainstem bronchus; a sudden drop in breath sounds signals the need to re-expand the retracted lung
-
Invasive arterial line (usually right radial) - for beat-to-beat BP monitoring; surgical retraction can compress great vessels causing sudden hypotension
-
Pre- and post-ductal pulse oximetry (right hand = preductal; foot = postductal) - detects intracardiac shunting
-
SpO₂ continuous
-
Capnography (ETCO₂)
-
Temperature monitoring - neonates are at high risk of hypothermia
-
Urinary catheter
-
Miller's Anesthesia, p. 10639; Morgan & Mikhail's, p. 1716
3. Induction and Airway Management
This is the most critical and technically demanding phase.
The Core Principle
Avoid positive-pressure ventilation by mask before the ETT is placed distal to the fistula (or the fistula is occluded).
Three Accepted Approaches to Intubation
Option 1 - Inhalational induction with spontaneous ventilation maintained (preferred)
- Inhalation induction with sevoflurane or halothane in oxygen
- Topical lidocaine spray to the larynx
- Intubate while spontaneous ventilation is maintained - no muscle relaxant
- Spontaneous breathing throughout until fistula is ligated
Option 2 - IV or inhalational induction followed by muscle paralysis and controlled intubation
- Risk: controlled ventilation via mask before ETT placement will distend stomach via fistula
- If this route is used, minimize mask ventilation time and use gentle pressures
- Gastrostomy tube (if present) must be left open to air to vent stomach distension
Option 3 - Awake intubation with mild sedation
- Protects airway while reducing aspiration risk
- Useful in very sick or extremely premature neonates
Modern practice generally favours Option 1 (inhalational induction, spontaneous ventilation). Options 2 or 3 may be necessary when spontaneous ventilation is not achievable.
- Barash's Clinical Anesthesia, p. 3665; Morgan & Mikhail's, p. 1715-1716
ETT Positioning - The Critical Step
Goal: ETT tip distal to the fistula, proximal to the carina
Since the fistula usually arises on the posterior membranous tracheal wall just proximal to the carina, the technique is:
- Advance the ETT deliberately into a mainstem bronchus (unilateral chest expansion + unilateral breath sounds confirm endobronchial position)
- Slowly withdraw until bilateral chest movement and bilateral breath sounds are confirmed
- The tip is now distal to the fistula but proximal to the carina
Bronchoscopy: Typically performed after induction to:
- Confirm fistula location and size
- Guide ETT placement
- A balloon embolectomy (Fogarty) catheter may be passed directly into the fistula to occlude it - this is particularly useful when the fistula is large or when adequate ventilation cannot be maintained
If ETT enters the fistula (suspect if: increased ventilation difficulty + falling SpO₂ + falling ETCO₂ + rapid gastric distension):
-
Withdraw the tube immediately
-
The surgeon can confirm by palpating the tube tip in the fistula
-
If gasric distension is extreme and ventilation impossible:
- Transcutaneous gastric decompression (needle/trocar)
- Intra-abdominal clamping of the distal esophagus via abdominal incision
- Emergent thoracotomy with fistula ligation as a last resort
-
Barash's Clinical Anesthesia, p. 3665-3666; Miller's Anesthesia, p. 10638-10639
4. Maintenance of Anaesthesia
- Volatile agent (sevoflurane/isoflurane) in oxygen - most neonates with TEF require 100% oxygen or high FiO₂ due to pre-existing pulmonary compromise
- Spontaneous ventilation is maintained until the fistula is ligated; after ligation, controlled ventilation with the lowest effective pressures and tidal volumes
- Muscle relaxants are used cautiously and only after fistula ligation in most cases; if used before ligation, the gastrostomy tube must be open
- Gastrostomy tube (if present) - kept open to air at the head of the table under the anaesthetist's direct observation; prevents kinking or obstruction; allows venting of gastric air during PPV
- Opioids - used sparingly in neonates planned for early extubation; moderate doses may necessitate postoperative ventilation
- Neuraxial anaesthesia (caudal catheter threaded to thoracic level, or paravertebral block) - adjunct to reduce volatile agent requirements, limit muscle relaxant use, reduce opioid need, and facilitate early extubation
Surgical Position and Intraoperative Concerns
- Patient in left lateral decubitus position for right thoracotomy (conventional left-sided aortic arch)
- For right-sided aortic arch, approach is based on surgeon preference (either side)
- During surgery: retraction of mediastinal structures can cause:
- Obstruction of left mainstem bronchus - detected by precordial stethoscope in left axilla
- Compression of great vessels (hypotension) - detected by arterial line
- Compression of vagus nerve (bradycardia)
- Lung retraction causing desaturation - surgeon must re-expand lung as needed
Thoracoscopic (VATS) Repair
-
Now the most common approach at experienced centres
-
Anaesthetic principles are the same
-
Additional challenges: single-lung ventilation in a neonate is technically demanding; hypercapnia and hypothermia are more pronounced; CO₂ insufflation for thoracoscopy can worsen hypercapnia and reduce venous return
-
Barash's Clinical Anesthesia, p. 3665-3666; Morgan & Mikhail's, p. 1715-1716; Miller's Anesthesia, p. 10639
5. Special Situation: H-Type (Type E) Fistula
The H-type fistula (no esophageal atresia) presents unique localisation challenges:
- Direct laryngoscopy and rigid bronchoscopy under spontaneous ventilation to identify the fistula
- A guidewire is passed through the fistula tract into the esophagus
- The infant is intubated carefully, without dislodging the wire
- Esophagoscopy is performed; the guidewire is visualised and brought out through the mouth
- Fluoroscopy determines the fistula level and guides choice of cervical vs. thoracic surgical approach
- Intraoperatively, the anaesthetist applies traction to the wire loop to help the surgeon localise the fistula
- Barash's Clinical Anesthesia, p. 3666
6. Management of the Premature Neonate with TEF
The ventilated premature neonate with TEF and hyaline membrane disease (RDS) is the highest-risk scenario:
-
High airway pressures required for RDS force large volumes of air through the fistula into the stomach
-
Progressive gastric distension further compromises already poor lung compliance
-
Moving the ETT tip distal to the fistula or placing a balloon catheter in the fistula may improve ventilation
-
Emergent gastrostomy (tube placed to water seal, analogous to a chest drain) can allow fistula air to escape while permitting some positive pressure ventilation
-
May require urgent thoracotomy with fistula ligation before full stabilisation
-
Sabiston Textbook of Surgery, p. 2679
7. Postoperative Management
Extubation Decision
| Favourable for early extubation | Requires continued ventilation |
|---|---|
| Robust, term neonate | Premature infant |
| No significant pneumonitis preoperatively | Significant aspiration pneumonitis |
| No major congenital heart disease | Complex congenital heart disease |
| Neuraxial/regional anaesthesia used | High opioid dose given |
| Short, uncomplicated procedure | Long gap EA, complex repair |
- If extubation is planned at end of surgery, tailor the anaesthetic technique accordingly: neuraxial analgesia + low volatile + minimal relaxants + minimal/no opioids
- If postoperative ventilation is required: keep head in neutral position; avoid neck extension; PEEP as appropriate
Critical Postoperative Precautions
- Neck extension is strictly avoided - can disrupt the esophageal anastomosis
- Esophageal instrumentation (e.g., NG tube advancement) is prohibited until cleared by the surgeon - blind suctioning past the anastomosis can disrupt the repair
- Gastrostomy tube remains in situ if placed; used for feeds while anastomosis heals
Postoperative Analgesia
- Wound infiltration with local anaesthetic
- Caudal catheter threaded to thoracic level - continuous infusion or intermittent bolus of local anaesthetic
- Paravertebral block (ultrasound-guided, unilateral) - excellent for ipsilateral hemithorax
- Systemic opioids used sparingly given respiratory concerns
Postoperative Complications to Monitor
| Complication | Features |
|---|---|
| Anastomotic leak | Fever, respiratory deterioration, pleural effusion |
| Esophageal stricture (~30-40%) | Dysphagia, feeding intolerance weeks later |
| Recurrent TEF | Coughing/choking with feeds |
| Tracheomalacia | Barking cough, expiratory stridor, "dying spells" |
| GERD | Very common; treat medically or surgically |
| Aspiration pneumonia | Ongoing pulmonary compromise |
- Barash's Clinical Anesthesia, p. 3666-3667; Morgan & Mikhail's, p. 1716
Summary: Key Anaesthetic Principles at a Glance
| Phase | Key Principle |
|---|---|
| Preoperative | Echocardiogram mandatory; Replogle tube in pouch; head-up prone positioning; correct dehydration |
| Induction | Avoid mask PPV; inhalational induction with spontaneous ventilation preferred |
| Intubation | ETT tip distal to fistula (advance into bronchus, then withdraw until bilateral sounds); bronchoscopy confirms; Fogarty catheter can occlude fistula |
| Maintenance | 100% O₂ often needed; keep spontaneous ventilation until fistula ligated; invasive BP monitoring; precordial stethoscope in left axilla |
| VATS-specific | Hypercapnia and hypothermia more likely; same ETT placement principles apply |
| Postoperative | Extubation decision based on fitness; avoid neck extension; neuraxial/regional analgesia to avoid opioids; nurse cautiously with anastomosis |
Evaluation, preparation and anaesthetic management of a pregnant patient with severe anaemia posted for elective lscs
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.