medicine symptom and investigation for jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have enough comprehensive content now to write a thorough answer. Let me compile the full response:
Jaundice: Symptoms and Investigations
Definition
Jaundice (icterus) is the yellowish staining of the skin, sclera, and mucous membranes caused by elevated serum bilirubin. It becomes clinically detectable when serum bilirubin rises above 2.5-3 mg/dL (normal: 0.3-1.0 mg/dL). Hyperbilirubinemia arises from overproduction of bilirubin, impaired uptake/conjugation/excretion, or regurgitation from damaged hepatocytes or bile ducts. - Harrison's Principles of Internal Medicine 22E, p. 366
Classification by Mechanism
| Type | Bilirubin | Cause Location |
|---|---|---|
| Pre-hepatic | Unconjugated (indirect) | Before liver - excess bilirubin production |
| Hepatic (intrahepatic) | Mixed | Within liver - hepatocellular damage or cholestasis |
| Post-hepatic | Conjugated (direct) | After liver - biliary obstruction |
Symptoms
General Symptoms (All Types)
- Yellow discoloration of skin, sclera (best seen in natural light), and mucous membranes
- Dark urine (bilirubinuria - tea/cola colored) - indicates conjugated hyperbilirubinemia
- Pale/clay-coloured stools (acholic stools) - indicates obstructed bile flow
- Pruritus (itching) - from bile salt deposition in skin; commonly accompanies cholestatic jaundice
Symptoms by Cause
Pre-hepatic (Hemolytic):
- Pallor (anemia)
- Splenomegaly
- No dark urine, no pale stools (unconjugated bilirubin not excreted in urine)
- Family history of hemolytic disorders (sickle cell, thalassemia, spherocytosis)
Hepatic (Hepatocellular):
- Fatigue, malaise, anorexia
- Nausea, vomiting
- Right upper quadrant (RUQ) discomfort or pain
- Fever (viral hepatitis, alcoholic hepatitis)
- Signs of liver failure: spider nevi, palmar erythema, gynecomastia, asterixis (flap), encephalopathy
- History of alcohol use, drugs, blood transfusions, IV drug use, sexual exposure
- Weight loss (in malignancy)
Post-hepatic (Obstructive):
- Painless jaundice - classic presentation of pancreatic head cancer / periampullary tumors
- Painful jaundice with fever and rigors - Charcot's triad of ascending cholangitis (stones)
- Courvoisier's sign: palpable, non-tender gallbladder (suggests malignant obstruction)
- Steatorrhea (malabsorption of fat due to lack of bile in duodenum)
- Weight loss in malignancy
- Dark urine and pale stools prominent
Key clinical distinction: Conjugated (direct) bilirubin crosses into urine giving dark urine. Unconjugated (indirect) bilirubin is albumin-bound and does NOT appear in urine.
Investigations
Step 1 - Baseline Blood Tests (First Line for All Patients)
| Test | Purpose |
|---|---|
| Serum bilirubin (total, direct, indirect) | Quantify jaundice; determine conjugated vs unconjugated |
| ALT / AST (transaminases) | Hepatocellular injury pattern |
| ALP / GGT (alkaline phosphatase) | Cholestatic pattern |
| Prothrombin time (PT/INR) | Synthetic function of liver |
| Serum albumin | Chronic liver disease marker |
| Full blood count (FBC/CBC) | Hemolysis, infection, thrombocytopenia (hypersplenism) |
Interpreting the Pattern
- Hepatocellular pattern: ALT/AST elevated out of proportion to ALP
- Cholestatic pattern: ALP elevated out of proportion to ALT/AST
- Isolated unconjugated hyperbilirubinemia: Think hemolysis, Gilbert's, Crigler-Najjar
- Isolated conjugated hyperbilirubinemia: Think Dubin-Johnson, Rotor syndrome
Step 2 - Further Tests Based on Pattern
A. If Unconjugated Hyperbilirubinemia (Pre-hepatic / Hemolytic Pattern)
- Peripheral blood smear - spherocytes, sickle cells, schistocytes
- Reticulocyte count - elevated in hemolysis
- Coombs test (direct antiglobulin) - positive in immune-mediated hemolysis
- LDH, haptoglobin - LDH elevated, haptoglobin decreased in hemolysis
- Hemoglobin electrophoresis - sickle cell, thalassemia
Gilbert's syndrome: Mild unconjugated hyperbilirubinemia (<6 mg/dL), worsened by fasting/illness/stress, affects 3-7% of population, benign condition. - Harrison's 22E
Crigler-Najjar Type I: Severe unconjugated jaundice (>20 mg/dL) in neonates due to complete absence of bilirubin-UDPGT; kernicterus common.
B. If Hepatocellular Pattern (ALT/AST predominant)
-
Viral serologies:
- Hepatitis A IgM
- Hepatitis B surface antigen (HBsAg) + HBc IgM
- Hepatitis C RNA (HCV RNA)
- Hepatitis E IgM (if indicated - developing countries)
- CMV DNA, EBV capsid antigen (if initial screen negative)
- Hepatitis D antibody (if HBV positive)
-
Toxicology screen - paracetamol/acetaminophen level
-
Ceruloplasmin and 24-hr urine copper - Wilson's disease (if patient <40 years)
-
Autoimmune markers:
- ANA (antinuclear antibody)
- SMA (smooth muscle antibody)
- Anti-LKM1 (liver-kidney microsomal antibody)
- SPEP (serum protein electrophoresis) - elevated IgG in autoimmune hepatitis
-
Liver biopsy - if above investigations are negative
C. If Cholestatic Pattern (ALP predominant) - Ultrasound First
- Abdominal ultrasound is the essential FIRST imaging step
- If bile ducts are dilated → extrahepatic cholestasis → proceed to CT/MRCP/ERCP
- If bile ducts are NOT dilated → intrahepatic cholestasis
- Check: AMA (anti-mitochondrial antibody) for Primary Biliary Cholangitis (PBC)
- Hepatitis serologies, drugs review
- If AMA positive → liver biopsy
- If AMA negative → MRCP + liver biopsy
Step 3 - Imaging
| Modality | Role |
|---|---|
| Abdominal Ultrasound | First-line; detects dilated ducts, gallstones, liver lesions, cirrhosis |
| CT abdomen (with contrast) | Better for pancreatic lesions, malignancy staging |
| MRCP (MR Cholangiopancreatography) | Non-invasive biliary tree imaging - best for choledocholithiasis, PSC, strictures |
| ERCP | Invasive; diagnostic AND therapeutic (stone extraction, stenting) |
| Liver biopsy | Definitive histological diagnosis when non-invasive tests inconclusive |
Ultrasound is excellent for biliary pathology and focal lesions; inexpensive, widely available, no radiation. Limitations include incomplete visualization with obesity and overlying bowel gas. - Schwartz's Principles of Surgery, 11E
Diagnostic Flowchart
Here is the evidence-based diagnostic approach (Harrison's 22E, Fig. 52-1):
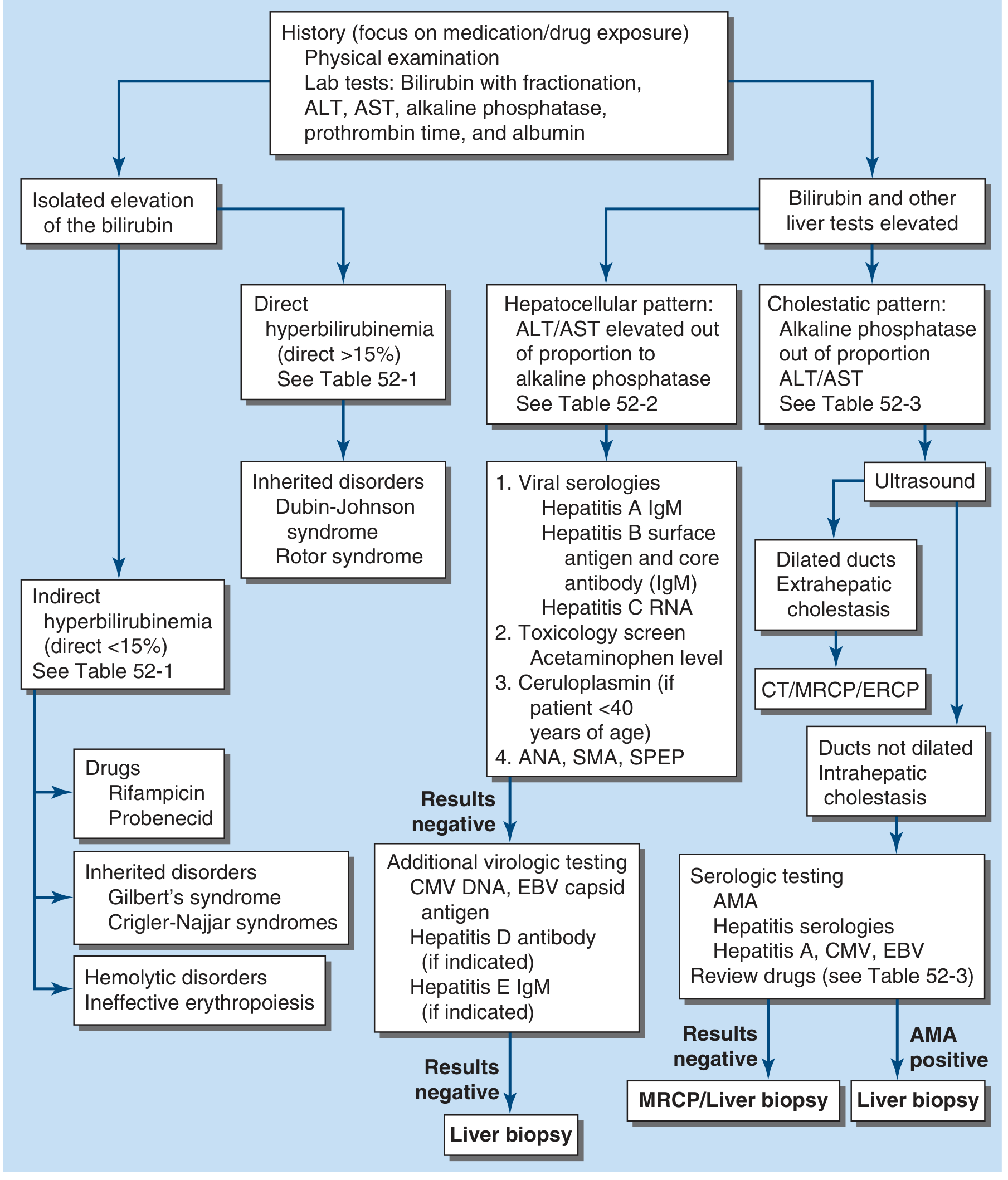
Flowchart from Harrison's Principles of Internal Medicine 22E - showing the step-by-step approach from bilirubin fractionation to liver biopsy
Common Causes Summary
| Category | Examples |
|---|---|
| Pre-hepatic | Hereditary spherocytosis, sickle cell disease, thalassemia, G6PD deficiency, autoimmune hemolysis, malaria |
| Hepatic - Inherited | Gilbert's syndrome, Crigler-Najjar (unconjugated); Dubin-Johnson, Rotor (conjugated) |
| Hepatic - Acquired | Viral hepatitis (A, B, C, D, E), alcoholic liver disease, drug-induced (paracetamol, INH, rifampicin), autoimmune hepatitis, Wilson's disease, ischemic hepatitis |
| Post-hepatic - Benign | Choledocholithiasis (most common extrahepatic cause), primary sclerosing cholangitis (PSC), strictures |
| Post-hepatic - Malignant | Pancreatic head carcinoma (classic painless jaundice), cholangiocarcinoma, ampullary carcinoma, gallbladder carcinoma |
In developing countries, infections (viral hepatitis, malaria, leptospirosis, typhoid) remain the leading cause of jaundice. In developed countries, drugs and extrahepatic biliary obstruction are more common. - Harrison's 22E
Sources: Harrison's Principles of Internal Medicine 22E (Ch. 52) | Schwartz's Principles of Surgery 11E | Sleisenger & Fordtran's Gastrointestinal and Liver Disease
medicine
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.