Cardiopulmonary bypass
Reading File
Finding Sources
Searching PubMed
"cardiopulmonary bypass"[MeSH Terms] AND complications
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have extensive, high-quality information from multiple authoritative textbooks. Let me compile the full answer.
Cardiopulmonary Bypass (CPB)
Definition and Purpose
Cardiopulmonary bypass is a technique that temporarily assumes the functions of both the heart and the lungs during cardiac surgery. It diverts venous blood away from the heart, adds oxygen and removes CO2, then returns the blood through a large artery - allowing the surgeon to operate on a still, bloodless heart. When fully established, CPB provides both artificial ventilation and circulation via the systemic vasculature. - Morgan and Mikhail's Clinical Anesthesiology, 7e
The CPB Circuit
The circuit has six basic components:
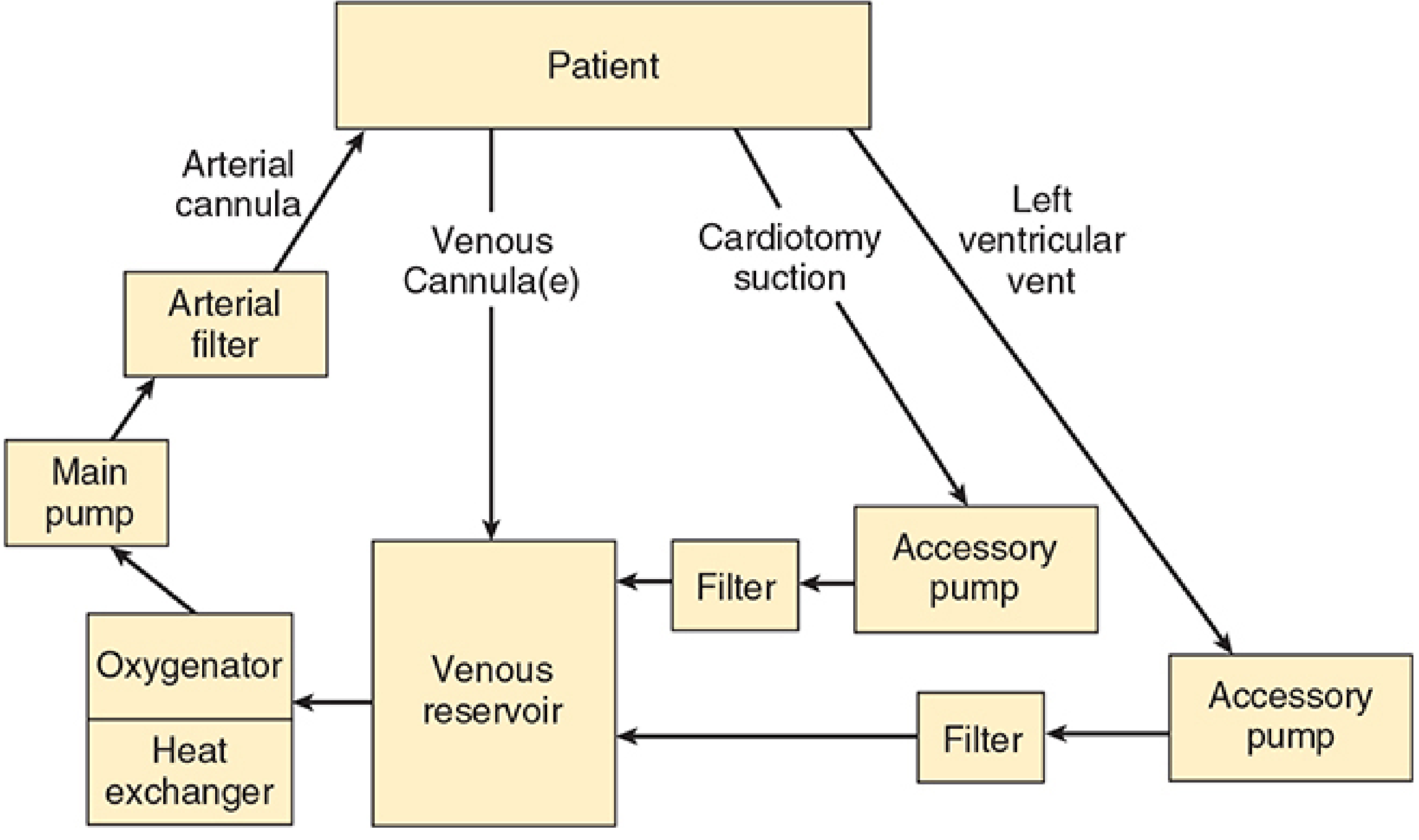
Figure: The basic design of the CPB machine, showing blood flow from patient through venous cannula(e) to the venous reservoir, then through the oxygenator/heat exchanger, main pump, arterial filter, and back to the patient via arterial cannula. - Morgan and Mikhail's Clinical Anesthesiology, 7e
1. Venous Reservoir
- Receives deoxygenated blood from the patient via cannulae placed in the right atrium, SVC, IVC, or femoral vein
- Blood returns by gravity drainage (siphon effect); flow depends on the height difference between patient and reservoir and cannula resistance
- Acts as a buffer to accommodate fluctuations in venous return
2. Oxygenator
- Adds O2 and removes CO2 from the blood
- Two types:
- Bubble oxygenator: oxygen froths directly with blood; settling chambers allow froth to coalesce back to blood
- Membrane oxygenator (now standard): blood contacts oxygen across a thin membrane - no foaming, less trauma to blood elements
- Pye's Surgical Handicraft, 22nd ed.
3. Heat Exchanger
- Blood cools below 37°C during CPB
- The heat exchanger (essentially a water bath) restores or adjusts temperature
- Used to induce deliberate hypothermia and to rewarm at the end of bypass
4. Main Pump (Roller Pump)
- The roller pump is the standard type; output is variable according to motor speed
- Centrifugal pumps are an alternative (less hemolysis, less risk of air embolism)
- Flow is characteristically non-pulsatile, which has physiological consequences (see Complications)
5. Arterial Line Filter
- A very fine mesh filter (pore size 20-30 μm) removes debris including air, fatty particles, and aggregated blood cells before blood is returned to the patient
- Critical for preventing microvascular embolism
6. Arterial Cannula
- Oxygenated blood is returned to the patient, usually via the ascending aorta (most common) or a femoral artery
- When inserted into the ascending aorta, blood flows retrograde, stopped at the closed aortic valve, and perfuses the coronary arteries and all systemic arteries
- Pye's Surgical Handicraft, 22nd ed.
Circuit Prime
Before use, the CPB circuit is primed with 1200-1800 mL of fluid (adults) to displace all air. A balanced salt solution (typically lactated Ringer's) is standard, often supplemented with:
- Colloid (albumin or starch)
- Mannitol (promotes diuresis)
- Heparin (500-5000 units)
- Bicarbonate
This hemodilution reduces the hematocrit to roughly 22-27% at bypass onset in adults. Blood is added to priming solutions for neonates, infants, or severely anemic adults. - Morgan and Mikhail's, 7e
Anticoagulation
- Heparin is given before cannulation (typically 300-400 units/kg) to prevent clotting in the circuit
- Adequacy is confirmed by the activated clotting time (ACT) - a target of >480 seconds is usual
- After bypass, heparin is reversed with protamine sulfate (1 mg per 100 units of heparin given)
- Matching heparin and protamine doses can be difficult; over- or under-dosing contributes to postoperative coagulopathy
Systemic Hypothermia
Core body temperature is often reduced to 20-32°C during CPB:
- Metabolic O2 requirements roughly halve with each 10°C drop in temperature
- Allows safer periods of reduced perfusion and protects organs
- "Tepid bypass" (30-35°C drift) is increasingly used for shorter cases
- Deep hypothermic circulatory arrest (DHCA): cooling to 15-18°C allows total cessation of CPB flow for up to 60 minutes - used for complex aortic arch repairs and pediatric congenital surgery
- Adverse effects: platelet dysfunction, coagulopathy, depression of myocardial contractility
- Rewarming via the heat exchanger restores normothermia at procedure end - Morgan and Mikhail's, 7e
Myocardial Protection
The heart is most vulnerable during the period of aortic cross-clamping, when coronary flow ceases entirely. Several strategies are employed:
Cardioplegia
- Potassium cardioplegia is the standard: a K+-rich solution (10-40 mEq/L) is infused into the coronary circulation, raising extracellular K+, reducing transmembrane potential, and arresting the heart in diastole
- Can be delivered:
- Antegrade: through a catheter in the proximal aorta (between the cross-clamp and aortic valve)
- Retrograde: through a catheter in the coronary sinus
- Repeated every ~30 minutes due to gradual washout and rewarming
- Solution also contains reduced Na+ (<140 mEq/L), calcium (0.7-1.2 mmol/L), magnesium (1.5-15 mmol/L), and a buffer (bicarbonate or histidine)
- Blood cardioplegia (4:1 blood:crystalloid) is increasingly preferred for its oxygen-carrying capacity and buffering
Topical Hypothermia
- Ice slush bathing the heart maintains myocardial temperature at 10-15°C
- Reduces basal metabolic O2 consumption
Ischemia and Reperfusion Injury
- Aortic cross-clamp times >120 minutes significantly increase risk
- Reperfusion after ischemia generates reactive oxygen species, intracellular Ca2+ overload, and endothelial-leukocyte interactions
- Myocardial stunning (reversible systolic and diastolic dysfunction) is common; responds to inotropes
- Myocardial necrosis is irreversible - Morgan and Mikhail's, 7e
Physiological Changes During CPB
CPB creates profoundly non-physiological conditions:
| Parameter | Effect during CPB |
|---|---|
| Blood flow | Non-pulsatile (most circuits) |
| MAP | Typically lower than normal |
| Temperature | Variable (often hypothermic) |
| Hematocrit | Reduced by hemodilution (~22-27%) |
| Hormonal | Renin-angiotensin activation → vasoconstriction |
| Drug concentrations | Altered by hemodilution, hypothermia, protein binding changes |
| EEG | Changes from hypothermia, hypotension, altered drug levels |
Non-pulsatile flow activates the renin-angiotensin system, leading to arteriolar vasoconstriction and impaired capillary perfusion - contributing to postoperative organ dysfunction. - Pye's Surgical Handicraft
Neurological Monitoring During CPB
- EEG / Processed EEG: hypothermia, hemodilution, and drug changes all alter EEG, making ischemia detection difficult; approximate entropy analysis can help quantify temperature-related changes
- Transcranial Doppler (TCD): monitors cerebral blood flow, detects emboli, and can identify misplaced cannulae; limited by probe instability and signal absence in some patients
- NIRS (Near-Infrared Spectroscopy): non-invasive cerebral oximetry; combined with TCD identifies patients with impaired autoregulation who are at higher risk for postoperative cognitive dysfunction and stroke. These patients may benefit from higher MAP during CPB
- NIRS + TCD combined is the most useful approach; neither modality alone has convincing outcome data for improving neurological results
- Miller's Anesthesia, 10e
Complications of CPB
1. Hemorrhage
- The clotting cascade is disrupted at multiple points: heparin/protamine dosing mismatches, protein degradation from O2 exposure, reduced platelet numbers and function
- A haemorrhagic tendency post-surgery is common
- Thresholds for re-exploration: >500 mL loss in 1 hour, or >300 mL/hour for 3 consecutive hours
- Treatment: protamine, platelet transfusion, fresh frozen plasma, desmopressin, or fresh blood (<8 hours old)
- Pye's Surgical Handicraft; PMID: 40473511 - recent meta-analysis on desmopressin efficacy (2025)
2. Organ Dysfunction (Post-Pump Syndrome)
- Non-pulsatile flow + small micro-emboli (20-40 μm; air, fat, aggregated cells) impair precapillary arteriolar flow
- Results in mild tissue hypoxia affecting virtually every organ system:
- Brain: confusion, delayed awakening, nightmares, or (rarely) stroke
- Kidneys/Liver: transient or (rarely) permanent dysfunction
- Lungs: impaired oxygenation ("post-pump lung")
- Heart: reduced myocardial contractility
- GI tract: ileus is common for 1-2 days post-op
- Organ damage increases with bypass duration; damage mild at 2 hours may be lethal at 4 hours
- Prevention: arterial line filter, hemodilution with crystalloid prime
- Pye's Surgical Handicraft
3. Cerebral Air Embolism
- When the heart is opened (e.g., valve surgery), air fills the cardiac chambers
- Even with meticulous de-airing, residual air enters the arterial circulation at heart restart
- Air emboli preferentially enter the right coronary ostium (superior position in supine patient)
- Consequences range from delayed awakening to irreversible widespread cerebral damage and death
- Considered the major hazard of open cardiac surgery
- Management: supportive care, steroids for cerebral oedema; no specific reversal
4. Vasoplegic Syndrome
- Post-CPB distributive shock from systemic inflammatory response to CPB
- Refractory to vasopressors; treated with methylene blue or hydroxocobalamin
- A 2024 systematic review (PMID: 39438181) found both agents effective for vasoplegic shock after CPB
5. Myocardial Damage
- Inadequate preservation, reperfusion injury, coronary embolism, graft vasospasm
- Manifests as reduced cardiac output, arrhythmias, or TEE-detected ventricular dysfunction at bypass termination
6. Inflammatory Response
- Blood-surface contact activates complement and inflammatory cascades
- Particularly pronounced in children (large surface area relative to blood volume)
- Managed with corticosteroids; in pediatric patients, modified ultrafiltration post-CPB removes cytokines and vasoactive substances while correcting hemodilution
Weaning from CPB
- Core temperature restored to normothermia via heat exchanger
- Cardiac rhythm confirmed (defibrillation if needed)
- Ventilation recommenced
- Venous inflow to bypass reservoir is gradually reduced while the heart takes over ejection
- TEE is used to assess ventricular function and identify residual surgical defects
- Inotropic support (dopamine, epinephrine, milrinone) if weaning is difficult
- Protamine is administered to reverse heparin anticoagulation
Special Considerations
Pediatric CPB
- Circuit prime volume is often 200-300% of the infant's blood volume → blood must be added to prime
- Higher flow rates required (up to 200 mL/kg/min)
- pH-stat management (maintaining pH by adding CO2 under hypothermia) may yield better neurological outcomes in children undergoing circulatory arrest
- DHCA at 15°C allows up to 60 minutes of complete circulatory arrest for complex repairs
- Calcium homeostasis is more often impaired; ionized calcium monitoring is essential
Off-Pump Cardiac Surgery (OPCAB)
- Coronary bypass can be performed on the beating heart without CPB, avoiding its systemic effects
- Requires specialized stabilizer devices; technically demanding
- Reduces risk of CPB-associated complications but not universally applicable
Key Points Summary
| Aspect | Key Fact |
|---|---|
| Anticoagulation | Heparin; ACT target >480 s; reversed with protamine |
| Pump prime (adult) | 1200-1800 mL; reduces HCT to 22-27% |
| Oxygenator | Membrane type (standard); bubble type (older) |
| Hypothermia range | 20-32°C routine; 15-18°C for DHCA |
| Safe aortic cross-clamp | <120 min preferred |
| Cardioplegia | High-K+ solution (10-40 mEq/L); arrests heart in diastole |
| DHCA duration limit | ~60 min at 15-18°C |
| Post-CPB coagulopathy | Heparin, platelet dysfunction, clotting factor dilution |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, Chapter 22
- Pye's Surgical Handicraft, 22nd Edition, Chapter 17
- Miller's Anesthesia, 10e, Chapter 14 (neurological monitoring)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
- Recent evidence: vasoplegic shock after CPB - hydroxocobalamin vs. methylene blue (PMID: 39438181, J Cardiothorac Vasc Anesth, 2024); desmopressin for bleeding reduction (PMID: 40473511, Heart Lung Circ, 2025); nitric oxide for organ protection (PMID: 40610908, BMC Anesthesiol, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.