A 48 years old female with a history of knee pain originating from patella radiating to the lateral aspect of the lower limb, with pain during flexion of knee with Difficulty climbing stairs
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
patellofemoral pain syndrome treatment
Reading File
Reading File
Searching Images
patellofemoral pain syndrome knee anatomy diagram
I now have comprehensive information to provide a thorough clinical analysis. Let me compile the answer.
Clinical Assessment: 48-Year-Old Female with Patellar Pain Radiating Laterally
Primary Diagnosis: Patellofemoral Pain Syndrome (PFPS) with Iliotibial Band (ITB) Involvement
This presentation is consistent with two co-existing conditions that frequently overlap:
1. Patellofemoral Pain Syndrome (PFPS)
Pathophysiology
PFPS arises from abnormal stresses at the patellofemoral articulation, often due to patellar malalignment, cartilage softening (chondromalacia patellae), or muscular imbalance. Pain originates from subchondral bone, synovium, and lateral retinacular structures under the patella. — ROSEN's Emergency Medicine
The lateral patellar facet compression syndrome is a specific subtype relevant here: a tight lateral retinaculum causes excessive lateral patellar tilt, generating lateral-sided patellar and peripatellar pain. — Miller's Review of Orthopaedics
Why This Patient Fits
| Feature | This Patient |
|---|---|
| Female sex | ✅ Women more commonly affected |
| Age 48 | ✅ Occurs in athletes and older patients with patellofemoral arthritis |
| Pain at/around patella | ✅ Patellar origin of pain |
| Worse with knee flexion | ✅ Classic — "movie sign" (prolonged flexion) |
| Difficulty climbing stairs | ✅ Hallmark symptom — stair climbing increases patellofemoral joint reaction forces |
| Insidious onset | ✅ Typical presentation |
Risk Factors to Assess in This Patient
- Gluteal and quadriceps weakness (most common predisposing factors)
- Patellar subluxation or increased Q-angle
- VMO (vastus medialis oblique) atrophy
- Hip abductor weakness → dynamic valgus → lateral patellar shift
2. Iliotibial Band (ITB) Syndrome — Explaining the Lateral Radiation
The radiation of pain to the lateral aspect of the lower limb points toward coexisting ITB syndrome or lateral retinacular tightness.
The ITB is a lateral thickening of the fascia lata running from the ilium to Gerdy's tubercle on the lateral tibia. During knee flexion, the ITB slides posteriorly over the lateral femoral condyle, causing friction and inflammation — producing lateral knee and lateral leg pain that can radiate toward the hip or distally. — Gray's Anatomy for Students; Harrison's Principles of Internal Medicine 22E
Physical Examination Findings to Elicit
For PFPS
- Patellar grind/Clarke's test: Reproduce pain by compressing patella against femoral condyle during quadriceps contraction
- Single-leg squat test: Reproduction of anterior/lateral knee pain
- Patellar tilt test: Assess lateral retinacular tightness
- Patellar glide: Lateral glide >3 quadrants suggests instability
- J-sign: Lateral patellar displacement at terminal extension
- Q-angle: >18° in females suggests increased lateral patellar pull
- VMO bulk and tone assessment
For ITB Syndrome
- Ober test: Patient in lateral decubitus on unaffected side; affected hip abducted, knee extended, then allowed to adduct — failure to fully adduct or lateral knee pain = positive
- Noble compression test: Compression of lateral femoral condyle at ~30° flexion reproduces pain
- Point tenderness at lateral femoral epicondyle
Investigations
| Test | Purpose |
|---|---|
| Weight-bearing X-ray (AP, lateral, skyline/Merchant view) | Assess patellofemoral joint space, tilt, arthritis |
| MRI knee | Evaluate cartilage integrity, lateral retinaculum, ITB, rule out meniscal pathology |
| CT axial (if X-ray inconclusive) | Measure patellar tilt angle and TT-TG distance |
PFPS is primarily a clinical diagnosis. Imaging rules out concurrent pathology. — ROSEN's Emergency Medicine
Differential Diagnoses to Consider
| Condition | Distinguishing Feature |
|---|---|
| Lateral meniscus tear | Joint-line tenderness, McMurray's test positive |
| Osteoarthritis (lateral compartment) | Osteophytes on X-ray, joint space narrowing |
| Popliteus tendinopathy | Pain posterolateral, worsened by downhill running |
| Common peroneal nerve compression | Paresthesia, foot drop, Tinel's at fibular head |
| Bipartite patella | Seen on X-ray (superolateral fragment), pain at fragment site |
Management
Non-Operative (First-Line)
1. Physical Therapy (cornerstone of treatment)
- Hip abductor + gluteal strengthening — current evidence shows superior outcomes when hip muscles are targeted in addition to quadriceps strengthening (BJSM 2024 best practice guide; Musculoskeletal Care 2025 meta-analysis)
- VMO-focused quadriceps strengthening (terminal knee extensions, step-ups)
- Core stability training
- Hip abductor and ITB stretching (for the lateral component)
- Gait/biomechanics retraining
2. NSAIDs: Short-term use (e.g., ibuprofen, naproxen) to reduce inflammation and enable participation in PT — ROSEN's Emergency Medicine
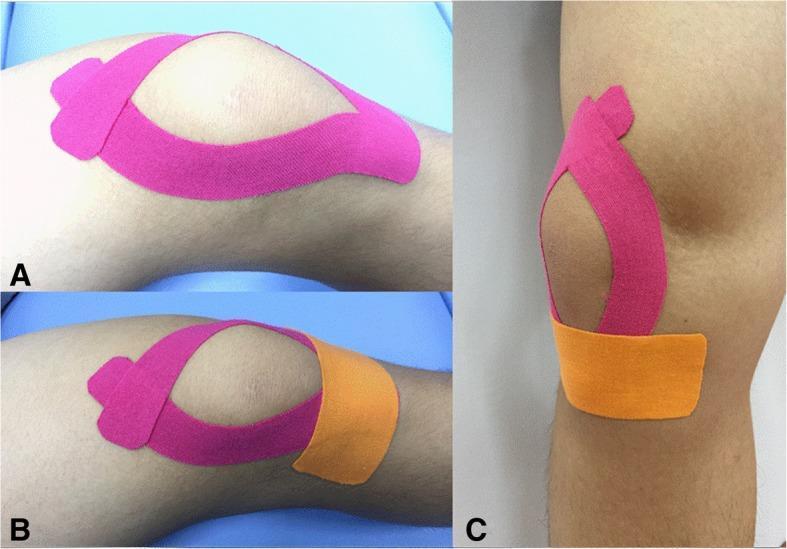
3. Patellar Taping (McConnell technique): Medial glide taping to correct lateral tracking; kinesio taping as adjunct for proprioception
4. Bracing: Patellar stabilizing brace or lateral buttress brace — evidence for efficacy is limited but may provide symptomatic relief
5. Activity Modification: Avoid prolonged knee flexion, deep squats, stair use until symptoms improve
6. Foot Orthotics: Indicated if excessive pronation contributes to dynamic valgus
For ITB Component
- Foam rolling/massage of ITB
- Ober stretch program
- Corticosteroid injection at lateral femoral condyle for refractory cases (avoid running ≥2 weeks post-injection)
Operative (Refractory Cases Only)
- Lateral retinacular release: Reserved for confirmed excessive lateral tilt unresponsive to ≥6 months conservative treatment, with evidence of neutral/negative tilt on arthroscopy and patella not articulating medially at 40° flexion — Miller's Review of Orthopaedics
- ITB surgical release: Rarely needed
Key Recent Evidence
- Neal et al. 2024 (BJSM) — Best practice guide synthesizing systematic review + patient voice: multimodal exercise (hip + knee) is the foundation; patient education and load management are critical
- Halabi et al. 2025 (Musculoskeletal Care) — Meta-analysis confirms that combined hip + knee strengthening is superior to knee-only strengthening for PFPS
Summary
This 48-year-old woman most likely has PFPS with lateral patellar facet compression and a coexisting ITB component explaining the lateral lower limb radiation. The combination of pain at the patella during flexion, stair difficulty, and lateral radiation is highly characteristic. Management is primarily non-surgical: aggressive hip/quad rehabilitation, NSAIDs for short-term pain control, patellar taping, and orthopedic follow-up. Imaging (X-ray + MRI) should be obtained to exclude cartilage damage, meniscal tears, or significant patellofemoral arthritis.
Sources: ROSEN's Emergency Medicine, Miller's Review of Orthopaedics 9th Ed., Harrison's Principles of Internal Medicine 22E, Gray's Anatomy for Students; BJSM 2024 [PMID 39401870]; Musculoskeletal Care 2025 [PMID 39934098]
This is a shared conversation. Sign in to Orris to start your own chat.