Name the urinary buffers. Explain their role in excreting excess acid from the body. Mention the other renal mechanisms of pH homeostasis (1+2+2)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a thorough, well-cited answer. Here is the complete response:
Urinary Buffers and Renal Mechanisms of pH Homeostasis
1. The Urinary Buffers (×1)
The two principal urinary buffers are:
- Phosphate buffer (HPO₄²⁻ / H₂PO₄⁻) - pK 6.8
- Ammonia/Ammonium buffer (NH₃ / NH₄⁺) - pK 9.1
A minor contribution is also made by creatinine, urate, and other organic anions filtered at the glomerulus.
2. Role of Urinary Buffers in Excreting Excess Acid (×2)
Why buffers are necessary
A common misconception is that the kidney excretes acid simply by acidifying the urine to a low pH. In fact, a urine volume of 1 L at pH 5.0 contains only 0.01 mmol of free H⁺ - a trivial amount compared with the ~50-100 mmol of fixed acid produced daily (~1 mmol/kg/day). The kidney cannot lower urine pH below 4.5-5.0. To excrete meaningful quantities of acid, H⁺ must be captured by urinary buffers, converting them to their conjugate acid forms and trapping them in the tubular lumen. Each H⁺ captured by a buffer also alkalinizes the tubular cell, allowing a "new" HCO₃⁻ to form within the cell and enter the blood - this is net acid excretion. - Goldman-Cecil Medicine, p. 1221-1222
A. Phosphate Buffer - Titratable Acidity
Reaction:
HPO₄²⁻ + H⁺ ⇌ H₂PO₄⁻ (pK = 6.8)
Phosphate is freely filtered at the glomerulus. In the tubular lumen, as H⁺ is secreted by the alpha-intercalated cells of the collecting duct (via H⁺-ATPase), the pH falls from 7.4 towards 5.0. At this range, the pK of 6.8 makes phosphate an extremely effective buffer - it accepts secreted H⁺ and converts dibasic phosphate (HPO₄²⁻) to monobasic phosphate (H₂PO₄²⁻), which is then excreted in urine. This is measured as titratable acidity (TA) - the amount of NaOH required to titrate urine back to pH 7.4.
Phosphate (plus creatinine) accounts for approximately 40-50% of the daily fixed acid load excreted as titratable acid. However, because the amount of phosphate filtered at the glomerulus is fixed and cannot be increased in response to acid loading, the phosphate buffer system has a limited capacity. - National Kidney Foundation Primer on Kidney Diseases, p. 1310; Ganong's Review, p. 2797
B. Ammonia Buffer - Ammonium Excretion
Reactions:
Glutamine → (glutaminase) → Glutamate + NH₄⁺ Glutamate → (glutamate dehydrogenase) → α-ketoglutarate + NH₄⁺
NH₃ + H⁺ ⇌ NH₄⁺ (pK = 9.1)
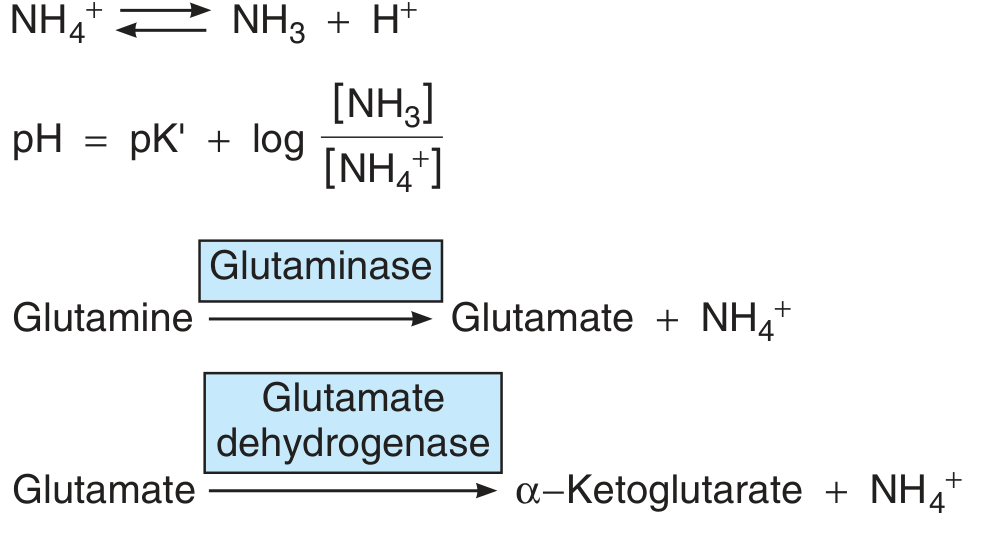
Ammonium is produced predominantly in the proximal tubule by mitochondrial glutaminase acting on glutamine. The process works as follows:
- NH₄⁺ is produced in proximal tubular cells and is in equilibrium with lipid-soluble NH₃ + H⁺ (pK 9.1, so at pH 7.0, the ratio of NH₃:NH₄⁺ is only 1:100).
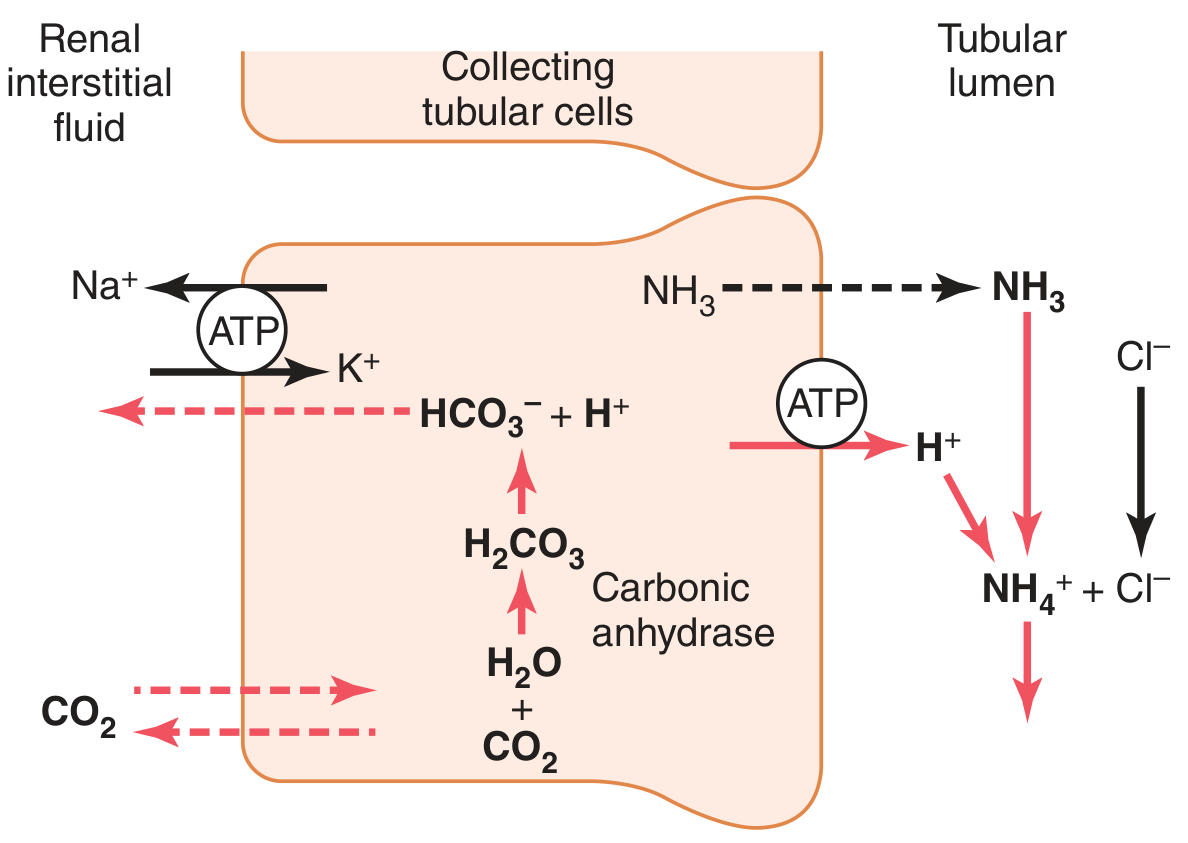
- NH₃ freely diffuses across the cell membrane into the tubular lumen and interstitium.
- In the lumen, NH₃ combines with secreted H⁺ to form NH₄⁺, which is ionically trapped and cannot cross the lipid membrane - it is excreted in urine.
- For each NH₄⁺ excreted, one new HCO₃⁻ is generated intracellularly (from the metabolism of α-ketoglutarate, which consumes 2H⁺ to free 2HCO₃⁻) and returned to the blood.
The ammonia buffer system accounts for 30-50% of normal net acid excretion. Critically, unlike phosphate, ammonia production can be upregulated massively in response to chronic acidosis - NH₄⁺ excretion can increase from ~40 mEq/day normally to up to 500 mEq/day, making it the dominant mechanism for net acid excretion during chronic metabolic acidosis. - Guyton and Hall, p. 417; Goldman-Cecil Medicine, p. 1222
Regulation of ammoniagenesis:
- Increased by metabolic acidosis, respiratory acidosis, and hypokalemia
- Metabolic acidosis triggers cortisol-mediated proteolysis in muscle, releasing glutamine into circulation
- Liver acidosis reduces urea cycle activity, diverting NH₃ to hepatic glutamine synthesis, which is then delivered to the proximal tubule as substrate
- In the kidney, NH₄⁺ preserves K⁺ by serving as an alternate cation for anion (e.g., Cl⁻) excretion - Goldman-Cecil Medicine, p. 1222
3. Other Renal Mechanisms of pH Homeostasis (×2)
A. Bicarbonate Reabsorption
The kidney filters approximately 4,500 mEq of HCO₃⁻ per day. This filtered HCO₃⁻ must be completely reclaimed before net acid excretion can occur; losing even one HCO₃⁻ ion in urine is equivalent to adding one H⁺ to the blood.
| Nephron Segment | % HCO₃⁻ Reabsorbed | Mechanism |
|---|---|---|
| Proximal tubule | ~80% | Na⁺/H⁺ exchanger (NHE3); luminal carbonic anhydrase IV converts luminal H₂CO₃ → CO₂ + H₂O; CO₂ re-enters cell, cytoplasmic CA II re-forms HCO₃⁻, which exits basolaterally via NBC1 |
| Thick ascending limb of Henle | 10-15% | Similar NHE3-mediated mechanism |
| Cortical collecting duct | < 10% | alpha-intercalated cells secrete H⁺ via H⁺-ATPase and H⁺/K⁺-ATPase; luminal HCO₃⁻ is consumed; HCO₃⁻ exits basolaterally via AE1 (Cl⁻/HCO₃⁻ exchanger) |
| Medullary collecting duct | Minimal | H⁺-ATPase continues; urine pH can fall to 4.5-5.0 |
beta-Intercalated cells in the cortical collecting duct have reverse polarity - they secrete HCO₃⁻ via apical pendrin (Cl⁻/HCO₃⁻ exchanger) when plasma HCO₃⁻ is elevated (metabolic alkalosis). This provides a mechanism for HCO₃⁻ elimination when there is excess alkali. - Goldman-Cecil Medicine, p. 881-889
B. Regulation of Acid Secretion (Adaptability)
The transport processes described above (H⁺-ATPase, Na⁺/H⁺ exchange, Cl⁻/HCO₃⁻ exchange) are not fixed - they adapt to the acid-base challenge:
- Metabolic and respiratory acidosis: increase HCO₃⁻ reabsorptive capacity, increase expression of luminal H⁺-ATPase, stimulate glutamine uptake into proximal cells to increase ammoniagenesis, and enhance distal H⁺ secretion.
- Metabolic and respiratory alkalosis: have the opposite effects - reduce H⁺ secretion, downregulate ammoniagenesis, and increase HCO₃⁻ secretion by beta-intercalated cells.
Net Acid Excretion (NAE) formula:
NAE = NH₄⁺ excretion + Titratable Acid excretion − urinary HCO₃⁻ excretion
In chronic kidney disease, the inability to produce sufficient ammonium leads to poor buffering, retention of fixed acids, and a progressively worsening metabolic acidosis - even though urine pH may already be maximally acidic. - Goldman-Cecil Medicine, p. 1222
Summary Table
| Component | Mechanism | Relative Contribution |
|---|---|---|
| Phosphate (titratable acid) | Filtered HPO₄²⁻ accepts secreted H⁺ → H₂PO₄⁻ | 40-50% of fixed acid; limited, cannot be upregulated |
| Ammonia/Ammonium | NH₃ from glutamine metabolism traps H⁺ as NH₄⁺ | 30-50% normal; up to 500 mEq/day in acidosis |
| HCO₃⁻ reabsorption | 80% proximal, 15% loop, <10% collecting duct | Reclaims all filtered HCO₃⁻; prerequisite for net acid excretion |
| Adaptive regulation | H⁺-ATPase upregulation, beta-intercalated cell HCO₃⁻ secretion | Fine-tunes response to acid/alkali loads |
Sources: Goldman-Cecil Medicine International Edition 2-Volume Set, pp. 881-889, 1221-1222 | Guyton and Hall Textbook of Medical Physiology, pp. 414-418 | Ganong's Review of Medical Physiology 26e, pp. 2772-2797 | National Kidney Foundation Primer on Kidney Diseases 8e, p. 1310
This is a shared conversation. Sign in to Orris to start your own chat.