explain part 4 in more detail with picture example.
cd /home/daytona/workspace/attachments/d99a624b-a1cb-45ec-8773-85d2a3cdc704/ && …
cd /home/daytona/workspace/attachments/d99a624b-a1cb-45ec-8773-85d2a3cdc704/ && …
cd /home/daytona/workspace/attachments/d99a624b-a1cb-45ec-8773-85d2a3cdc704/ && …
cd /home/daytona/workspace/attachments/d99a624b-a1cb-45ec-8773-85d2a3cdc704/ && …
Humphrey Field Analyser HFA printout explained annotated image grey scale deviation plot
HFA 24-2 printout annotated SITA standard grey scale total deviation pattern deviation glaucoma example
https://eyeguru.org/essentials/visual-fields
Part 4: The Humphrey Field Analyser (HFA) - In Full Detail
4.1 Testing Strategies (Algorithms)
Full Threshold
SITA (Swedish Interactive Thresholding Algorithm)
- SITA Standard - the most commonly used. Same accuracy as Full Threshold but takes ~6-7 minutes. The benchmark for glaucoma monitoring.
- SITA Fast - halves the test time again (~3-4 min) with a small accuracy tradeoff. Useful for patients with poor concentration.
- SITA Faster - newest generation, fastest of all. Comparable to SITA Standard in accuracy with very short test duration.
Suprathreshold Screening
4.2 Testing Patterns (Which Locations Are Tested?)
| Pattern | Coverage | Primary Use |
|---|---|---|
| 24-2 | Central 24°, 54 points on a 6° grid | Standard for glaucoma - captures arcuate defects |
| 30-2 | Central 30°, 76 points | Neurological field loss, wider coverage |
| 10-2 | Central 10°, 68 points, 2° grid | Advanced glaucoma, macular disease |
| Macula | Central 4.24°, 16 points | Subtle central defects |
4.3 Step-by-Step: How to Read an HFA Printout

STEP 1: Patient Details + Reliability Indices
| Index | What it measures | Acceptable | What goes wrong when it fails |
|---|---|---|---|
| Fixation Losses (FL) | Blindspot re-presentations: did the patient move their eye? | < 20% | High FL = wandering fixation; the field map is spatially unreliable |
| False Positives (FP) | Patient pressing the button when NO stimulus was shown ("trigger happy") | < 15% | Grey scale looks artificially pale/white (sensitivities seem too good); most important index |
| False Negatives (FN) | Patient NOT pressing when a bright suprathreshold stimulus is shown at a location they previously saw | < 15% | Cloverleaf pattern - central points done at the start are answered correctly, peripheral points done later are missed due to fatigue |
Kanski's rule: If reliability indices are significantly abnormal, do NOT interpret the field. Repeat the test. The entire subsequent analysis is invalidated.
STEP 2: Grey Scale
- White/light grey = high sensitivity (the patient easily sees dim stimuli here)
- Dark grey to black = low sensitivity (the patient cannot detect stimuli here, or needs them very bright)
STEP 3: Numerical Sensitivity Map (Raw dB Values)
- A value of
<0= the patient could not see even the brightest stimulus - that location is essentially blind. - Compare these numbers to the deviation plots below, which tell you how abnormal each value actually is for this patient's age.
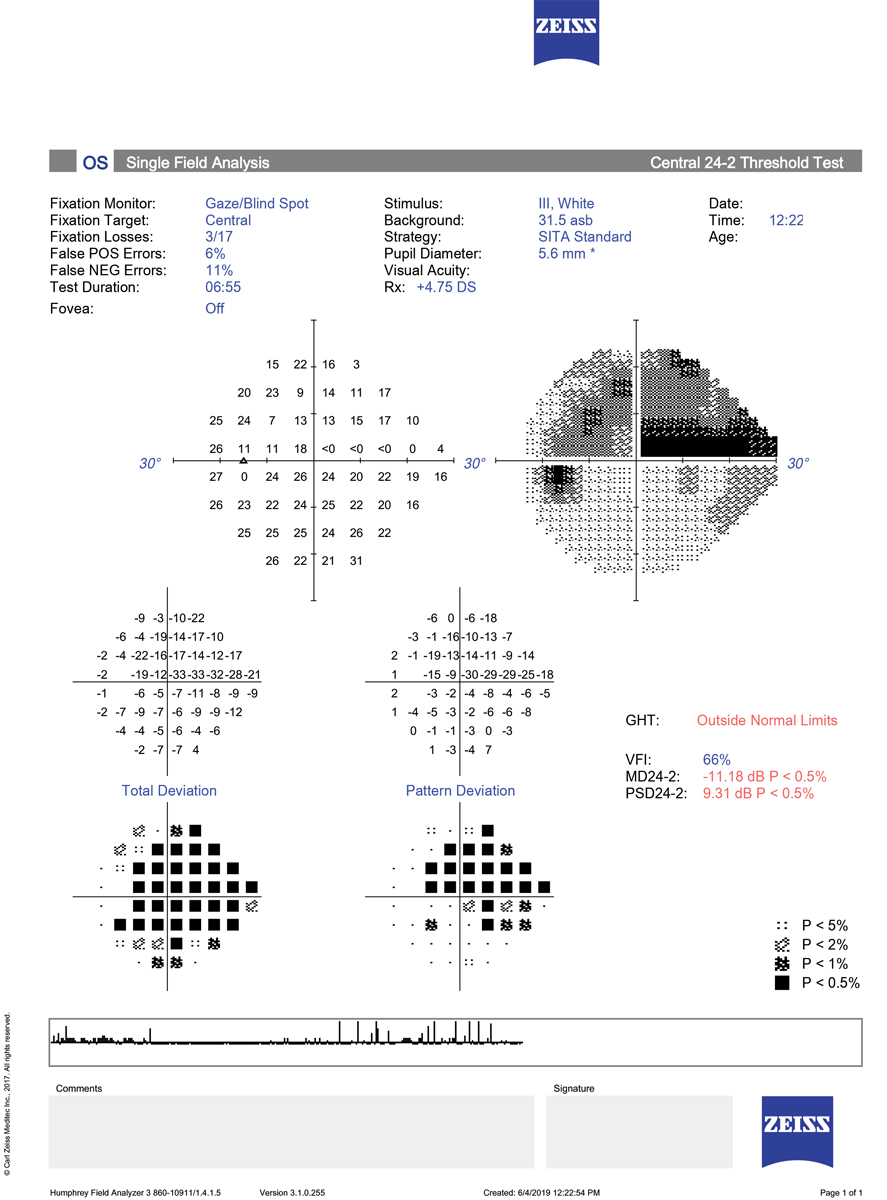
STEP 4: Total Deviation (TD) Plot
- A negative number (e.g., -8 dB) means that point is 8 dB worse than expected for this patient's age.
- A positive number means slightly better than normal (uncommon).
| Symbol | Meaning |
|---|---|
| · | p < 5% (mildly below normal) |
| :: | p < 2% |
| ▩ | p < 1% |
| ■ | p < 0.5% (most significant - this point is very unlikely to be normal) |
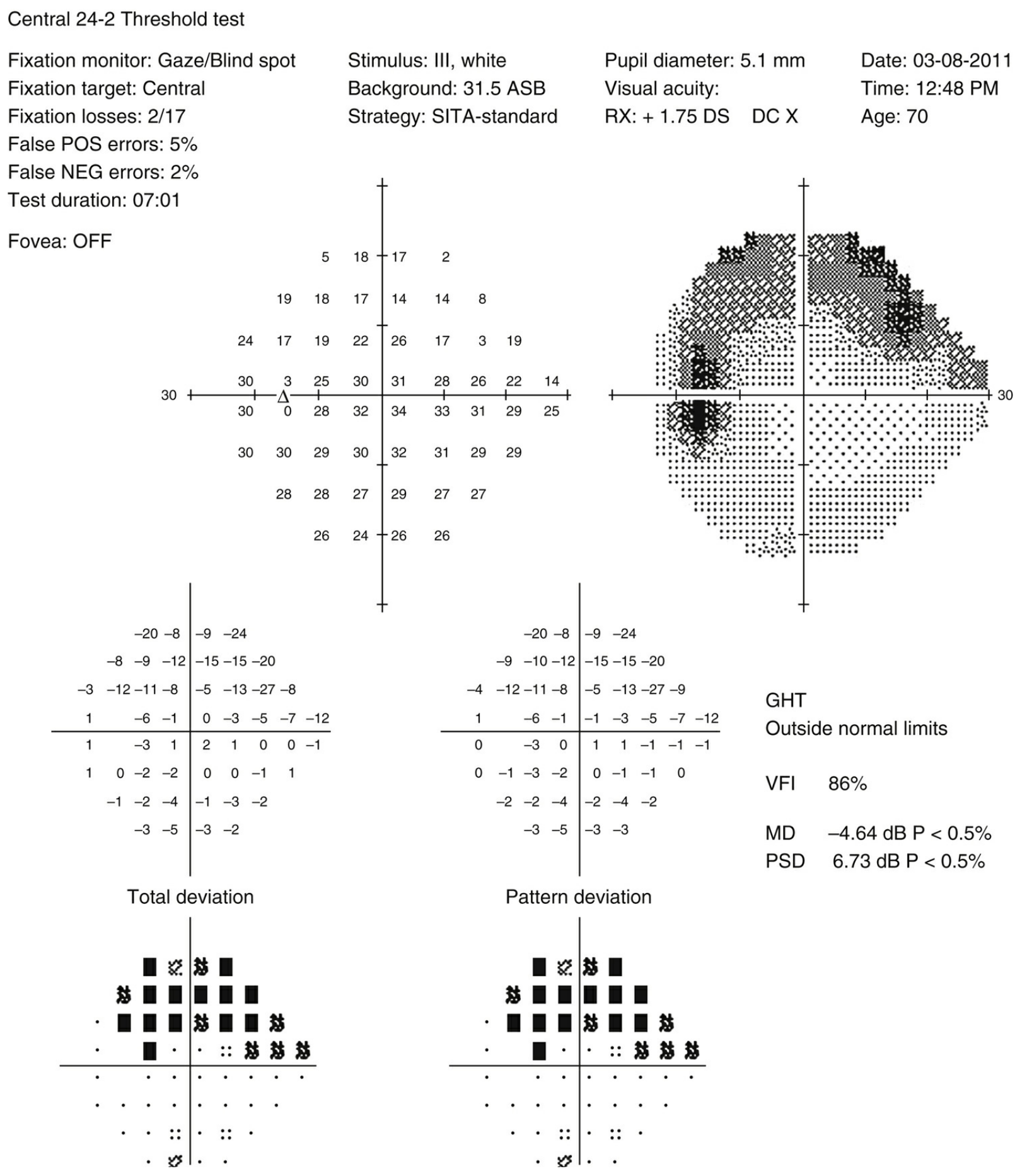
STEP 5: Pattern Deviation (PD) Plot
| Scenario | TD | PD | Interpretation |
|---|---|---|---|
| Cataract/miosis/poor dilation | Diffusely abnormal | Normal | Diffuse depression - media opacity, not nerve damage |
| Glaucomatous arcuate defect | Focally abnormal | Also abnormal | True focal nerve damage |
| Mixed (cataract + glaucoma) | Globally abnormal | Focal defect visible | PD unmasks the true glaucoma pattern beneath the cataract effect |
Remember: TD abnormal + PD normal = think cataract/miosis/media opacity. TD abnormal + PD abnormal = true focal field defect.
STEP 6: Global Indices
- Normal: 0 to -2 dB
- Mild loss: -2 to -6 dB
- Moderate loss: -6 to -12 dB
- Severe loss: worse than -12 dB
- Normal fields have a smooth hill of vision, so PSD is low.
- High PSD = focal irregular loss = more specific for glaucoma (arcuate scotoma creates a patchy pattern)
- A diffuse cataract depresses all points equally - PSD stays low even though MD is very negative.
- PSD rises early in glaucoma, making it a sensitive marker of focal nerve damage.
- 100% = completely normal field
- 0% = completely blind
- Used for tracking the progression rate (e.g., -1% per year = slow progression, -5% per year = fast and worrying)
- "Within Normal Limits" - the two hemifields are symmetrically normal
- "Borderline" - a small but suspicious asymmetry
- "Outside Normal Limits" - asymmetry exceeds the 99.5th percentile; strongly suggests glaucoma
- "General Reduction of Sensitivity" - both hemifields equally depressed (think cataract, not glaucoma)
- "Abnormally High Sensitivity" - false positives are inflating sensitivities
STEP 7: Guided Progression Analysis (GPA)
- "Possible progression" - a change exceeding the test-retest variability threshold at several locations on one field
- "Likely progression" - the same significant change confirmed on a second consecutive field
Key Clinical Rules for the HFA
- Never interpret an unreliable field. Check FL, FP, FN first - every time.
- Grey scale is a first impression only. Always verify with the deviation plots.
- Pattern Deviation is your main diagnostic tool - it strips away media opacity and reveals true focal defects.
- TD abnormal + PD normal = cataract/miosis. TD abnormal + PD abnormal = true glaucoma/neuro defect.
- GHT "Outside Normal Limits" is one of the earliest and most reliable glaucoma indicators.
- For progression monitoring, look at VFI trend, MD trend, and GPA together - no single number tells the whole story.
what are the viva questions that can be asked in POAG from basic to advanced level?
cd /home/daytona/workspace/attachments/d99a624b-a1cb-45ec-8773-85d2a3cdc704/ && …
cd /home/daytona/workspace/attachments/d99a624b-a1cb-45ec-8773-85d2a3cdc704/ && …
POAG Viva Question Bank - Basic to Advanced
BASIC LEVEL
- Retinal nerve fibre layer (RNFL) thinning
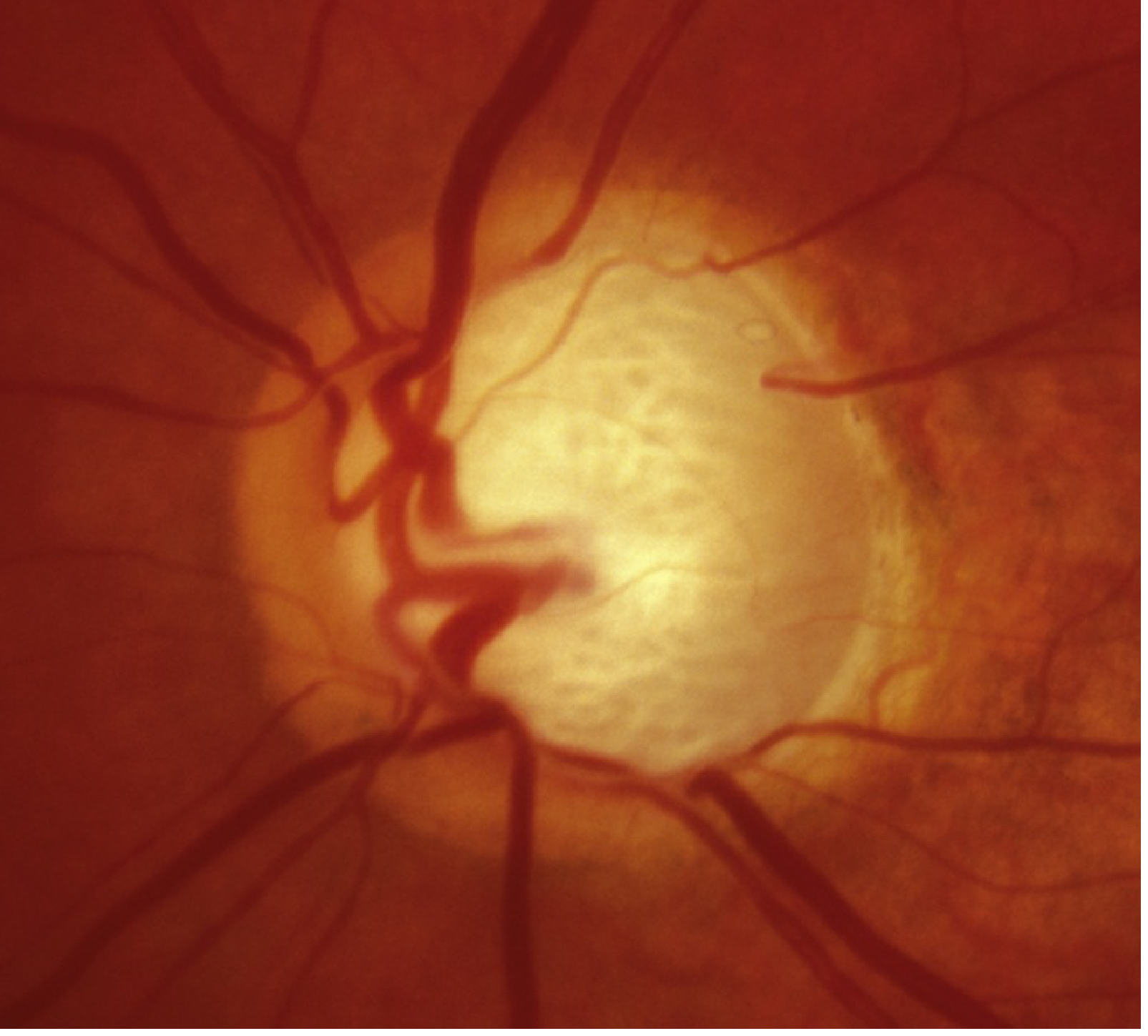
- Glaucomatous optic nerve damage (cupping)
- Characteristic visual field loss as damage progresses
- An open anterior chamber angle on gonioscopy
- Absence of signs of secondary glaucoma or a non-glaucomatous cause for the optic neuropathy
- IOP is a key modifiable risk factor (but is not mandatory for diagnosis)
| Risk Factor | Detail |
|---|---|
| IOP | Higher IOP = greater risk. Asymmetry of ≥4 mmHg is significant |
| Age | More common in older individuals |
| Race | ~4x more common in Black populations; earlier onset, harder to control |
| Family history | Siblings: 4x risk; offspring: 2x risk |
| Myopia | Associated with increased incidence; myopic eyes more susceptible |
| Large optic disc | More vulnerable to glaucomatous damage |
| Low ocular perfusion pressure | Increases risk |
| Translaminar pressure gradient | Difference between IOP and orbital CSF pressure may deform the lamina cribrosa |
| Systemic Ca-channel blockers | Higher prevalence in meta-analyses |
| Anti-VEGF injections | Risk of sustained IOP elevation, especially with repeated bevacizumab |
- Tonometry - measure IOP (Goldmann applanation is gold standard)
- Gonioscopy - confirm the angle is open (no peripheral anterior synechiae, no neovascularisation, normal-appearing angle)
- Optic disc assessment + visual field testing - look for glaucomatous cupping and characteristic field loss
- A vertical C/D ratio >0.6 is suspicious
- Asymmetry of C/D ratio >0.2 between the two eyes is significant and more important than the absolute value
- The neuroretinal rim (NRR) follows the ISNT rule normally: Inferior > Superior > Nasal > Temporal. Any reversal of this rule suggests glaucomatous rim loss.
INTERMEDIATE LEVEL
- Direct mechanical damage - RGC axons are physically compressed/kinked as they pass through the lamina cribrosa, especially with elevated IOP deforming this structure
- Ischaemic damage - compression of blood vessels supplying the optic nerve head reduces blood flow, especially when ocular perfusion pressure is low
- Increased vertical C/D ratio (>0.6)
- C/D asymmetry between eyes >0.2
- Neuroretinal rim thinning or notching - especially inferior and superior poles
- ISNT rule violation
- Disc haemorrhage (Drance haemorrhage) - a small splinter haemorrhage at the disc margin, strongly associated with progression
- Bayonetting sign - vessels appear to disappear over the disc edge then reappear at the base of the cup, indicating a steep cup wall
- Overpass cupping - vessels pass over the cup wall
- RNFL defect - visible as a wedge-shaped dark shadow on red-free photography, precedes visual field changes
- Peripapillary atrophy (PPA) - beta zone (bare sclera) enlargement
- Nasal shifting of vessels
- Nasal step (earliest sign) - an asymmetry of sensitivity across the horizontal meridian nasally, due to nasal fibres being more vulnerable
- Paracentral scotoma - small islands of loss within 10° of fixation, corresponding to arcuate bundle damage
- Arcuate (Bjerrum) scotoma - coalescence of paracentral scotomas curving from the blind spot above or below fixation, following the arcuate nerve fibre bundles
- Ring scotoma - when superior and inferior arcuate defects join
- Altitudinal defect - loss of either upper or lower hemifield
- Temporal island - a small island of temporal vision persists while the rest is gone (temporal fibres most resilient)
- Central island - only a small central island of fixation remains
- Total blindness - end stage
- GHT Outside Normal Limits
- A cluster of three or more non-edge points in a typical glaucomatous location, all depressed at p<5% on Pattern Deviation, with at least one at p<1%
- Corrected PSD occurring in <5% of normals
| Stage | MD Value |
|---|---|
| Early | MD < -6 dB |
| Moderate | MD -6 to -12 dB |
| Severe | MD worse than -12 dB |
- Thin cornea (<500 µm): GAT underestimates true IOP - patient may appear to have normal IOP but actually have higher true IOP. Independently associated with greater risk of glaucoma development (OHTS study).
- Thick cornea (>600 µm): GAT overestimates true IOP - patient may be labelled as having elevated IOP when it is actually normal.
| Drug Class | Example | Mechanism | IOP Reduction | Key Side Effects |
|---|---|---|---|---|
| Prostaglandin analogues | Latanoprost, bimatoprost (once daily, PM) | Increase uveoscleral outflow | 25-35% | Iris/lash pigmentation, periorbital fat loss, CME in aphakia |
| Beta-blockers | Timolol 0.5% | Reduce aqueous production (ciliary body) | 20-27% | Bradycardia, bronchospasm - contraindicated in asthma/COPD |
| Alpha-2 agonists | Brimonidine 0.2% | Reduce aqueous production + increase uveoscleral outflow | 18-27% | Allergy/follicular conjunctivitis (up to 25%), fatigue, CNS depression in children |
| Topical CAIs | Dorzolamide, brinzolamide | Inhibit carbonic anhydrase II in ciliary body → reduce aqueous production | 15-20% | Stinging, metallic taste |
| Systemic CAIs | Acetazolamide, methazolamide | Same mechanism, more potent | 30-40% | Paraesthesias, fatigue, nausea, renal stones, aplastic anaemia (rare) |
| Miotics (parasympathomimetics) | Pilocarpine | Increase trabecular outflow (ciliary muscle contraction) | 20-30% | Miosis, brow ache, myopia in young, risk of RD |
- Severity of existing damage (C/D ratio, visual field MD)
- Pre-treatment IOP level
- CCT
- Rate of progression if known
- Age and life expectancy
ADVANCED LEVEL
- MYOC gene (myocilin protein, found in trabecular meshwork) - multiple mutations described; accounts for ~3-4% of POAG cases, often with earlier onset and higher IOP
- OPTN gene (optineurin) - associated with Normal Tension Glaucoma
| Feature | POAG (high IOP) | NTG |
|---|---|---|
| Average disc size | Normal | Larger on average |
| Disc haemorrhages | Less frequent | More frequent - associated with progression |
| Field defects | Arcuate, peripheral | Tend to be closer to fixation, deeper, steeper |
| Peripapillary atrophy | Present | More prevalent |
| Vascular associations | Less prominent | More prominent (migraine, vasospasm, hypotension) |
- VA loss out of proportion to cupping
- Loss of colour vision on Ishihara testing
- VF loss not matching RNFL loss pattern
- Pallor of neuroretinal rim (suggests non-glaucomatous optic neuropathy)
- Rapid progression despite normal pressure
- RNFL thickness - the classic "TSNIT" profile (Temporal-Superior-Nasal-Inferior-Temporal). Inferotemporal thinning is the earliest and most common OCT sign. RNFL thinning precedes visual field defects by months to years.
- Ganglion Cell Layer (GCL) thickness - macular GCL analysis is sensitive for early damage, especially inferior to the fovea.
- Optic disc parameters - rim area, disc area, cup/disc ratio, vertical C/D.
- "Possible progression" - significant worsening at specific test locations on one field
- "Likely progression" - the same significant change confirmed on two consecutive fields
| Stage | Narrowest Rim Width |
|---|---|
| 1 | ≥0.4 (at risk) |
| 2-4 | 0.1-0.39 (at risk) |
| 5 | <0.1 (threshold for glaucoma damage) |
| 6 | Rim = 0 (absent) over <45° |
| 7-9 | Rim absent over 46-270° |
| 10 | Rim absent over >270° (severe disability) |
| Procedure | Mechanism | Key Facts |
|---|---|---|
| Trabeculectomy | Creates a fistula from the anterior chamber to the subconjunctival bleb, bypassing the trabecular meshwork | Gold standard; use of antimetabolites (MMC, 5-FU) improves success but increases risk of bleb leak and hypotony |
| Tube-shunt surgery (AGV, Baerveldt) | Silicone tube drains aqueous to an equatorial plate under the conjunctiva | Used when trabeculectomy is likely to fail (e.g. previous failed bleb, uveitis, neovascular glaucoma) |
| Selective Laser Trabeculoplasty (SLT) | 532 nm Nd:YAG laser selectively targets melanin in trabecular meshwork cells, stimulating macrophage clearance and remodelling | Equivalent IOP reduction to ALT; lower energy, repeatable; can be used as first-line |
| Argon Laser Trabeculoplasty (ALT) | Burns trabecular meshwork to improve outflow | Initial success 70-80%, drops to 50% by 2-5 years; not repeatable |
| MIGS (Minimally Invasive Glaucoma Surgery) | Various devices (iStent, Hydrus, Kahook blade, goniotomy) that improve trabecular/Schlemm's canal outflow | Lower IOP reduction than trabeculectomy but much safer; often combined with cataract surgery |
| Trial | Finding |
|---|---|
| OHTS (Ocular Hypertension Treatment Study) | Treating ocular hypertension with drops reduces the risk of conversion to POAG. CCT is an independent risk factor - thin corneas at greatest risk |
| AGIS (Advanced Glaucoma Intervention Study) | Keeping IOP below 18 mmHg at all visits is associated with virtually no visual field progression |
| EMGT (Early Manifest Glaucoma Trial) | Progression risk is influenced by: (a) magnitude of initial IOP reduction, (b) height of baseline IOP, (c) pseudoexfoliation, (d) bilateral disease, (e) worse MD, (f) older age |
| CIGTS (Collaborative Initial Glaucoma Treatment Study) | Surgery and medication equally effective for initial IOP control; similar quality of life outcomes |
| LiGHT Trial (UK, 2019) | SLT as first-line treatment is at least as effective as drops and may be more cost-effective; 74% of SLT patients required no drops at 3 years |
- IOP consistently above target despite maximum tolerated medical therapy
- Progression despite target IOP being achieved
- Inability to tolerate or comply with medical therapy
- End-stage disease where even small further IOP reduction has significant benefit
- Patient preference (avoidance of lifelong drops)
| Feature | POAG | PACG |
|---|---|---|
| Angle | Open (normal gonioscopy) | Closed/narrow (peripheral anterior synechiae, appositional closure) |
| IOP mechanism | Increased resistance at trabecular meshwork | Mechanical obstruction of trabecular meshwork by iris |
| Onset | Insidious, chronic | Can be acute (angle-closure crisis) or chronic |
| Symptoms | Asymptomatic | Acute: severe pain, redness, haloes, vomiting |
| Prevalence | European/African populations | Asian populations (shorter axial length, thicker lens, shallower AC) |
| Treatment | Medical/laser/surgery | Laser peripheral iridotomy (LPI) is definitive for angle closure |
- Confirm reliability of the visual field (repeat if necessary)
- Check CCT - a thin cornea means Goldmann tonometry is underestimating true IOP
- Perform 24-hour IOP phasing to exclude IOP spikes (especially nocturnal)
- Gonioscopy to confirm open angle
- Check colour vision (Ishihara) - impaired colour vision points to optic neuritis or compression
- MRI brain/orbits if: VA loss disproportionate to cupping, colour vision loss, VF pattern atypical, pallor of rim, rapid progression
- Blood tests: B12, FBC, ESR, CRP, ACE, autoantibodies, lipids, glucose, syphilis serology
- 24-hour ambulatory BP monitoring - nocturnal dip is a risk factor for NTG progression
- Once secondary causes excluded and diagnosis confirmed: treat to a lower target IOP (typically 30% reduction from baseline or IOP <12 mmHg in NTG)
as a final year postgraduate resident hoping to achieve gold medal, what are the things that should be known beyond this?
primary open angle glaucoma neuroprotection treatment
MIGS minimally invasive glaucoma surgery outcomes
OCT angiography glaucoma optic disc perfusion
glaucoma gene therapy neuroprotection clinical trial
POAG gold medal postgraduate advanced topics 2024 2025 lamina cribrosa OCT angiography sustained drug delivery MIGS neuroprotection
AAO preferred practice pattern POAG 2026 updates corneal hysteresis sustained release SLT first line
selective laser trabeculoplasty first line glaucoma LiGHT trial
https://www.reviewofoptometry.com/news/article/aaos-updated-…
corneal hysteresis glaucoma progression risk factor
glaucoma sustained drug delivery bimatoprost implant travoprost punctal plug
POAG advanced viva topics postgraduate 2025 Rho kinase inhibitor netarsudil aqueous veins Schlemm canal microstructure OCT-A
Beyond the Textbook: POAG at Gold Medal Level
1. AQUEOUS DYNAMICS - THE PHYSIOLOGY THEY WILL PROBE
Production
- Active secretion (dominant, ~90%) - Na-K-ATPase and carbonic anhydrase II drive bicarbonate and sodium into the posterior chamber, water follows osmotically. This is the target of CAIs and beta-blockers.
- Ultrafiltration - hydrostatic pressure-driven, IOP-dependent
- Simple diffusion - minor
Two Outflow Pathways
| Pathway | Percentage | Route | Target of Drugs |
|---|---|---|---|
| Conventional (trabecular) | 60-80% | TM → Schlemm's canal → collector channels → episcleral veins | Pilocarpine, ROCK inhibitors, SLT |
| Uveoscleral (unconventional) | 20-40% | Through ciliary muscle interstices → suprachoroidal space → sclera | Prostaglandin analogues |
Gold medal point: Episcleral venous pressure (EVP) is the downstream backpressure in the conventional pathway. Normal EVP is ~8-12 mmHg. It is the reason IOP cannot be reduced below a certain level by conventional outflow drugs alone. EVP is elevated in Sturge-Weber syndrome, superior vena cava obstruction, and orbital varix. ROCK inhibitors (netarsudil) reduce episcleral venous pressure directly - a unique mechanism no other drug class has.
The Goldman Equation
2. THE LAMINA CRIBROSA - THE FORGOTTEN VILLAIN
What is the lamina cribrosa?
Biomechanical theory of POAG
- Mechanically kinks and compresses RGC axons as they pass through the fenestrae
- Disrupts axoplasmic flow - BDNF (brain-derived neurotrophic factor) made in the lateral geniculate nucleus cannot travel retrogradely to sustain RGC survival
- Causes glial cell activation, extracellular matrix remodelling and collagen deposition - making the lamina progressively stiffer over time
Lamina Cribrosa Depth (LCD) and Lamina Cribrosa Curvature Index (LCCI)
- Greater posterior bowing (higher LCCI) at baseline predicts faster visual field progression rate independent of IOP
- Younger patients (<69 years) with greater LCCI show more rapid VF loss - suggesting the lamina is more deformable in younger eyes
- This is why some POAG eyes progress despite "controlled" IOP - the lamina has already been structurally remodelled
Gold medal point: The translaminar pressure gradient = IOP minus intracranial pressure (ICP). Normal ICP is ~10 mmHg, so normal gradient is ~6-8 mmHg. In NTG: normal IOP but low ICP (often seen in patients who are positional sleepers, low body weight) widens this gradient and damages the lamina exactly like elevated IOP does. This explains why some NTG patients have "normal" IOP but still progress rapidly.
3. CORNEAL HYSTERESIS - THE 2026 AAO PPP'S STAR
What is corneal hysteresis (CH)?
Why it matters in POAG
- Low CH is independently associated with faster rates of visual field progression (after adjusting for IOP and CCT)
- It reflects scleral stiffness, not just corneal stiffness - and stiffer sclera transmits more pressure to the lamina cribrosa
- The 2026 AAO PPP elevated CH to its own dedicated section, calling it an adjunct risk factor for progression alongside CCT and IOP
- The key takeaway: two patients with identical IOP, CCT, and MD - the one with lower CH is at higher risk of faster progression and should have a lower target IOP
Key difference from CCT: CCT primarily affects Goldmann tonometry accuracy. CH affects biological susceptibility to glaucomatous damage.
4. RHO KINASE (ROCK) INHIBITORS - THE NEW DRUG CLASS
Mechanism
- Relaxing the actomyosin cytoskeleton of trabecular meshwork cells → cells become less stiff → better drainage through TM
- Opening inter-endothelial spaces in Schlemm's canal
- Reducing episcleral venous pressure (unique among all glaucoma drugs)
- Minor reduction in aqueous production
Approved drugs
- Netarsudil 0.02% (Rhopressa) - once daily, FDA approved 2017. Also inhibits norepinephrine transporter (NET), reducing aqueous production.
- Ripasudil 0.4% (Glanatec) - approved in Japan
- Netarsudil/latanoprost combination (Rocklatan) - single daily drop combining two different mechanisms (conventional + uveoscleral outflow), achieving ~30% IOP reduction
Side effects
Gold medal insight
5. SUSTAINED DRUG DELIVERY SYSTEMS
Current and emerging systems
| Device | Drug | Route | Duration | Status |
|---|---|---|---|---|
| Bimatoprost SR (Durysta) | Bimatoprost | Intracameral biodegradable implant | ~3-6 months | FDA approved (2020) |
| iDose TR (Glaukos) | Travoprost | Intracameral sustained-release titanium implant | ~3 years | FDA approved (2024) |
| Travoprost punctal plug | Travoprost | Punctal plug (sits in the lacrimal punctum) | Ongoing | Clinical trials |
| OTX-TIC | Travoprost | Intracameral | 12+ months | Phase 3 trials |
| Subconjunctival implants | Various | Subconjunctival | Several months | Investigational |
Key data: Sustained-release systems achieve 93% adherence by eliminating the need for patient compliance with daily drops. IOP reductions of 5.4-9.5 mmHg have been reported consistently across trials. The 2026 AAO PPP cited this as a major advance in glaucoma management.
6. MINIMALLY INVASIVE GLAUCOMA SURGERY (MIGS) - THE FULL PICTURE
MIGS Classification (2026 AAO PPP)
- MIGS (non-bleb based): trabecular/Schlemm's canal procedures
- MIBS (minimally invasive bleb surgery): newer bleb-forming procedures
Non-bleb MIGS - Trabecular/Canal Procedures
| Device/Procedure | Mechanism | Notes |
|---|---|---|
| iStent inject W | Titanium micro-bypass stent into Schlemm's canal (bypasses TM) | Most studied; typically 2 stents |
| Hydrus Microstent | Larger stent spanning 3 clock-hours of Schlemm's canal | HORIZON RCT: reduced IOP and medication burden when combined with cataract surgery |
| Kahook Dual Blade (KDB) goniotomy | Excises a strip of TM (not bypass - removes the resistance) | Can be standalone; repeatable; evidentiary data now strong |
| GATT (Gonioscopy-Assisted Transluminal Trabeculotomy) | 360° trabeculotomy using a suture or illuminated catheter | Best for younger patients, high-IOP POAG; good data in Black patients |
| Ab interno canaloplasty (ABiC/OMNI) | Dilates Schlemm's canal + viscodilates collector channels | Addresses collector channel resistance beyond TM |
Minimally Invasive Bleb Surgery (MIBS)
| Procedure | Notes |
|---|---|
| XEN gel stent | Ab interno conjunctival bleb via 45µm gel stent; comparable to trabeculectomy in moderate POAG with lower complication rate |
| PRESERFLO (InnFocus) | 8.5 mm long microshunt; creates external bleb; results comparable to trabeculectomy at 2 years |
Gold medal point on MIGS limitations: MIGS requires a functioning Schlemm's canal and collector channels. In advanced POAG with severe trabecular/canal damage, or in eyes with high baseline IOP needing large reductions, traditional trabeculectomy/tube remains superior. Meta-analyses show ROCK inhibitors may lose efficacy in advanced POAG for the same reason - irreversible TM damage.
7. LiGHT TRIAL - 6 YEAR DATA (2026, PMID: 41043781)
- At target IOP: SLT-first 94.2% vs. drops-first 94.7% (equivalent)
- Drop-free control without surgery: SLT-first 69.8% vs. drops-first 18% (dramatic difference)
- Need for trabeculectomy: SLT-first 2.4% vs. drops-first 5.8% (SLT significantly reduces need for incisional surgery)
- IOP: SLT 16.3 vs. drops 15.4 mmHg (clinically equivalent)
- VF progression to OAG/deterioration: SLT-first 19.6% vs. drops-first 26.8% (SLT may actually protect better)
Gold medal question: "Why might SLT show fewer progressors than drops?" Answer: drops require daily adherence; SLT provides consistent, continuous IOP control. The benefit is in real-world consistency, not in the mechanism itself.
8. OCT-ANGIOGRAPHY (OCT-A) IN GLAUCOMA
What does OCT-A measure?
Why it matters in POAG
- Vascular theory of glaucoma: Reduced optic nerve head perfusion (ischaemia) is a parallel pathway of RGC death alongside the mechanical compression theory
- OCT-A shows reduced optic disc flow index and vessel density in POAG eyes vs. normal
- Optic disc haemorrhages (Drance haemorrhages) are associated with focal ischaemia and OCT-A demonstrates localised reduction in perfusion at the bleeding site
- Studies show reduced vessel density precedes RNFL thinning at some locations - earlier than even OCT-A structural measures
Current limitations
9. NEUROPROTECTION - THE HOLY GRAIL
Why we need neuroprotection
Current state of evidence
| Agent | Mechanism | Status |
|---|---|---|
| Citicoline (CDP-choline) | Precursor of phosphatidylcholine (neuronal membrane); promotes RGC survival; improves VEP amplitudes | Systematic review (2023, PMID: 37768938): evidence suggests benefit in slowing VF deterioration; not yet standard of care |
| Nicotinamide (Vit B3) | Restores mitochondrial function in RGCs; increases NAD+ levels | Phase 2 RCTs ongoing; real-world case series show tolerability and trend to slower progression |
| Coenzyme Q10 + Vitamin E | Antioxidant; counters mitochondrial oxidative stress in RGCs | Studies show preserved GCL thickness and better VEP in combination with standard therapy (Dogan et al., 2025) |
| Brimonidine | Alpha-2 agonist; beyond IOP lowering, upregulates BDNF and inhibits glutamate excitotoxicity | LOW-PRESSURE GLAUCOMA TREATMENT STUDY (LoGTS): brimonidine reduced progression more than timolol in NTG, despite similar IOP - possible neuroprotective effect |
| Memantine | NMDA receptor antagonist; blocks excitotoxic glutamate cascade | Phase 3 RCT (Weinreb et al.) showed no benefit over placebo in slowing VF loss - the biggest failed neuroprotection trial |
Gold medal point: No drug is currently approved specifically for neuroprotection in glaucoma. IOP remains the only proven modifiable target. However, the LoGTS study with brimonidine is the strongest signal yet that neuroprotection independent of IOP may be achievable. The field is watching NAD+ precursor (nicotinamide) trials closely.
10. GENETICS BEYOND MYOC AND OPTN
The Polygenic Architecture
Polygenic Risk Score (PRS)
- High PRS individuals screened earlier and treated at lower IOP thresholds
- Low PRS individuals monitored less intensively
- This enables personalised glaucoma medicine - the same approach used in familial hypercholesterolaemia and BRCA testing for breast cancer
Pharmacogenomics (PMID: 37833756)
11. PATTERN ERG (pERG) - OBJECTIVE GLAUCOMA ASSESSMENT
What is pERG?
Why it matters
- pERG detects RGC dysfunction before RNFL thinning and before VF defects - the earliest objective marker available
- Particularly valuable in patients with unreliable visual fields (low cognition, tremor, malingerers)
- A reduced P50 amplitude (the positive deflection at 50ms) is the key abnormality in glaucoma
- Progressive reduction in P50 amplitude correlates with RGC loss on OCT
Current role
12. THE TUBE VS. TRABECULECTOMY STUDY - 5 YEAR DATA
- Compared tube-shunt (Baerveldt 350) to trabeculectomy + MMC in previously unoperated eyes with medically uncontrolled glaucoma
- At 5 years: no significant difference in IOP, visual acuity, or VF
- Failure rate: trabeculectomy 29% vs. tube 21% (tube had slightly better survival)
- Complications: trabeculectomy had more serious complications (especially hypotony maculopathy, bleb leaks), but tubes had more exposure/erosion
Gold medal point: Traditionally, trabeculectomy was reserved for first surgery and tubes for failed trabeculectomies. PTVT shows tubes are a reasonable first surgical choice, particularly in eyes at high risk of bleb failure (previous conjunctival surgery, uveitis, young patients).
13. CLINICAL SCENARIOS THAT ONLY GOLD-MEDAL CANDIDATES ANSWER CORRECTLY
- Personalised medicine via PRS - treating based on genetic risk, not just measured IOP
- Sustained drug delivery (iDose TR, Durysta) - eliminating adherence as the biggest cause of treatment failure
- Neuroprotection (nicotinamide, citicoline, ROCK inhibitors) - protecting RGCs independent of IOP
- MIGS expansion - minimising the step from drops to surgery; earlier surgical intervention with better safety profiles
- Artificial intelligence in progression detection - AI algorithms now outperform clinicians in detecting early OCT and VF changes and predicting progression rate from a single visit
Summary: What Separates Gold Medal from Average
| Average resident knows | Gold medal candidate adds |
|---|---|
| Goldman equation conceptually | Uses it to justify rational drug combinations |
| Prostaglandins increase uveoscleral outflow | Uveoscleral accounts for 20-40% of outflow; PGAs increase this to 50-60% |
| SLT is repeatable | LiGHT 6-year data: SLT-first patients 69.8% drop-free vs. 18% |
| CCT affects tonometry | CH predicts progression rate via scleral biomechanics |
| Lamina cribrosa exists | LCCI predicts VF progression independently of IOP |
| MIGS is less invasive than trabeculectomy | Classification into MIGS/MIBS; trabecular vs. canal vs. suprachoroidal; limitations in advanced disease |
| No neuroprotection available | LoGTS (brimonidine); nicotinamide trials; the failed memantine RCT |
| MYOC and OPTN genes | Polygenic risk scores; pharmacogenomics; NTG/POAG genetic overlap |
| pERG is an ERG variant | P50 amplitude detects RGC dysfunction before structural or functional changes |