Bronchiectasis with bronchial, poorly controlled bronchial asthma, and there's thick brownish mucus plugs. What could be the diagnosis?
Reading File
Searching the Web
ABPA allergic bronchopulmonary aspergillosis diagnosis criteria 2024
Searching PubMed
allergic bronchopulmonary aspergillosis diagnosis criteria
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to give a thorough answer. Here is the full response:
Diagnosis: Allergic Bronchopulmonary Aspergillosis (ABPA)
The triad you describe - central bronchiectasis + poorly controlled asthma + thick brownish/dark mucus plugs - is the classic presentation of ABPA. This is an eosinophilic hypersensitivity disease caused by Aspergillus fumigatus colonizing the airways of genetically susceptible asthmatics.
Why This Triad Points to ABPA
| Feature | Explanation |
|---|---|
| Poorly controlled asthma | ABPA occurs in ~7-14% of patients with refractory asthma. Asthma that fails usual therapy should trigger ABPA workup |
| Central (proximal) bronchiectasis | A hallmark finding - affects lobar bronchi and first/second-order segmental bronchi; distal airways remain normal |
| Brownish mucus plugs | Hyphae of Aspergillus grow within mucus plugs in the proximal bronchi. The brown color comes from the fungal elements and necrotic eosinophils. Plugs have a characteristic tapering cylindrical shape with branching (matching parent bronchi) |
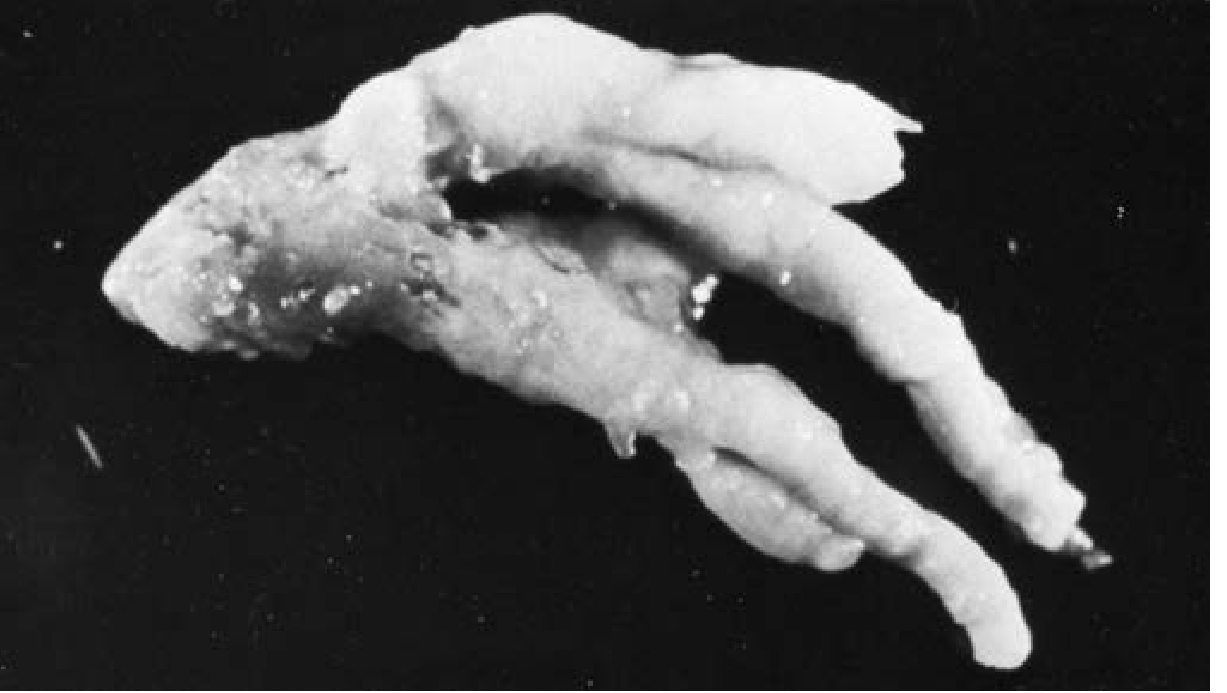
Mucus plug expectorated by a patient with ABPA - note the tapering, branching cylindrical shape characteristic of the bronchial tree. (Fishman's Pulmonary Diseases)
Pathogenesis
A. fumigatus conidia are inhaled and colonize the airways. In susceptible individuals (with HLA-DR2/DR5 alleles, CFTR mutations, or collectin polymorphisms), a dysregulated Th2 immune response occurs:
- Mast cell IgE cross-linking by Aspergillus antigens → degranulation → vasodilatation and vascular leakage
- Anti-Aspergillus IgG enters the bronchi → immune complexes form → complement activation → pulmonary inflammation and damage
- Aspergillus proteases further compromise mucociliary clearance and breach the epithelial barrier
The result is progressive airway damage with central bronchiectasis, mucoid impaction, and recurrent atelectasis.
Diagnostic Criteria (Revised ISHAM 2024)
Predisposing condition - asthma, cystic fibrosis, COPD, or bronchiectasis
Essential criteria (both required):
- Elevated Aspergillus-specific IgE (or positive Aspergillus skin test)
- Elevated total serum IgE (>1000 IU/mL; may be lower if all other criteria met)
Additional criteria (at least 2 of the following):
- Precipitating serum antibodies to A. fumigatus (elevated IgG)
- Radiographic opacities consistent with ABPA (central bronchiectasis, mucoid impaction, finger-in-glove opacities)
- Blood eosinophilia (>500 cells/µL) - in a glucocorticoid-naive patient
Radiological Features
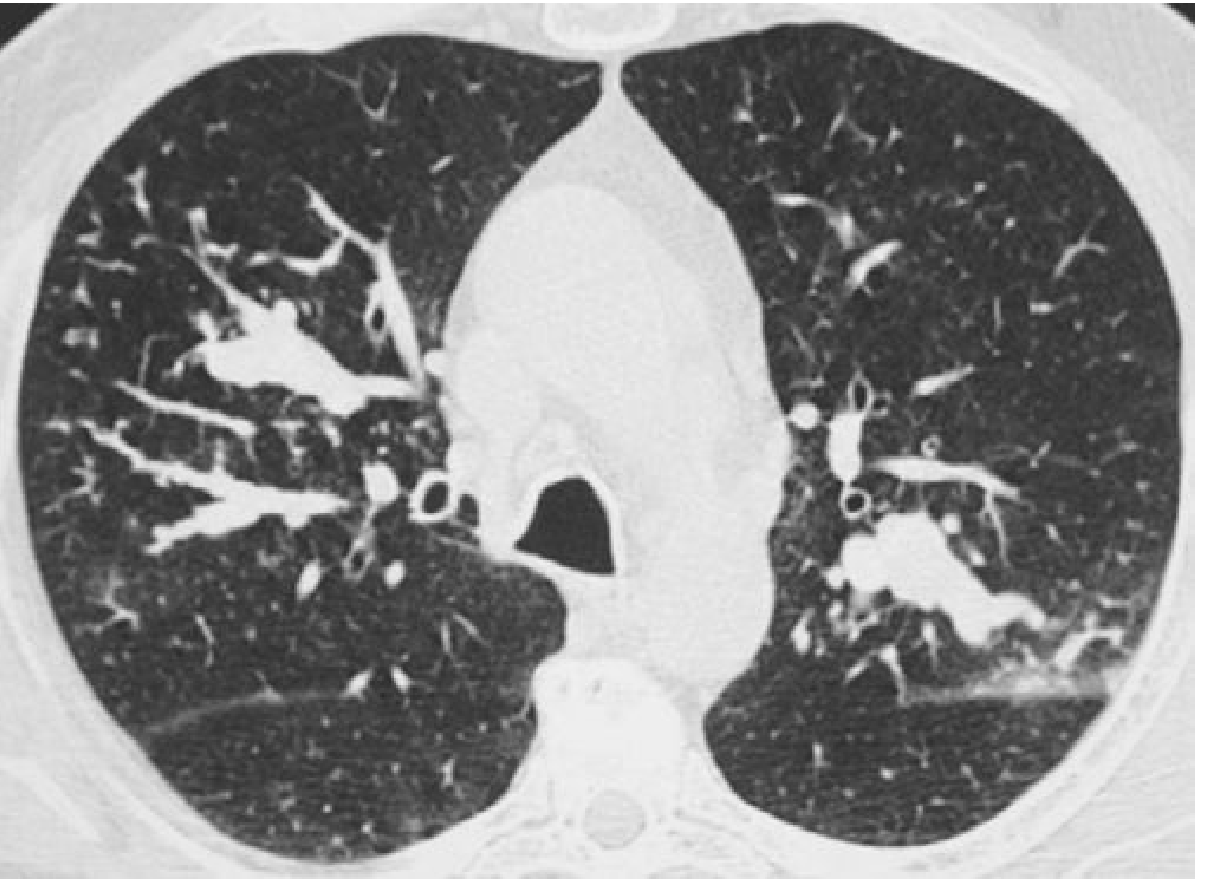
CT chest in ABPA: mucoid impactions within segmental and subsegmental dilated bronchi of the upper lobes, with centrilobular branching opacities (tree-in-bud). (Grainger & Allison's Diagnostic Radiology)
CT findings highly specific for ABPA:
- Varicose or cystic central bronchiectasis (90% in ABPA vs. 30% in asthma alone)
- Mucoid impaction of segmental/subsegmental airways (67% vs. 4%)
- Centrilobular nodules and tree-in-bud opacities (93% vs. 28%)
- High-attenuation mucus plugs (due to calcium salts/dystrophic calcification) - the most specific CT sign, especially in CF patients
- "Finger-in-glove" opacity, "tram lines," and fleeting pulmonary infiltrates
Additional Investigations to Order
- Total serum IgE level
- Aspergillus-specific IgE and IgG (RAST or ImmunoCAP)
- Aspergillus skin prick test
- CBC with differential (peripheral eosinophilia)
- Sputum culture for fungi
- HRCT chest
Management Summary
| Treatment | Indication |
|---|---|
| Oral prednisolone (0.5 mg/kg/day, taper over 3-6 months) | First-line for acute exacerbations |
| Itraconazole or voriconazole (4-month course) | Reduces antigenic stimulus; used with steroids for recurrent/steroid-dependent disease |
| Omalizumab (anti-IgE) | Severe ABPA, especially in CF; evidence also for mepolizumab/benralizumab (anti-IL-5) in eosinophilic ABPA |
| Inhaled therapies | For underlying asthma control |
Acute exacerbations cause progressive, irreversible lung damage with eventual cavitation, upper lobe contraction, and honeycomb fibrosis if not controlled - making early diagnosis and treatment important.
Sources: Fishman's Pulmonary Diseases and Disorders (pp. 2324-2325) | Harrison's Principles of Internal Medicine 22E (2025) | Grainger & Allison's Diagnostic Radiology | Revised ISHAM-ABPA Guidelines, Eur Respir J 2024
This is a shared conversation. Sign in to Orris to start your own chat.