Pelvic injuries. Orthopaedics notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent — I have all the material needed. Here are comprehensive orthopaedic notes on pelvic injuries:
Pelvic Injuries — Orthopaedic Notes
Sources: Miller's Review of Orthopaedics (9th ed.), Rockwood & Green's Fractures in Adults (10th ed., 2025)
1. Anatomy and Conceptual Framework
The pelvis must be viewed as a ring structure. A single break in the ring generally does not produce instability. Unstable injuries always involve injury to at least two areas of the pelvis. The pelvis is divided into:
- Anterior ring — pubic symphysis and pubic rami
- Posterior ring — sacroiliac (SI) joints, sacrum, ilium
The posterior ring is the primary load-bearing structure. Ligamentous stability is critical: the interosseous sacroiliac ligament is the strongest ligament of the pelvic ring. The sacrotuberous, sacrospinous, and iliolumbar ligaments provide supplementary stability.
2. Imaging
| View | What It Shows |
|---|---|
| AP pelvis | Initial trauma evaluation; identifies increased pelvic volume |
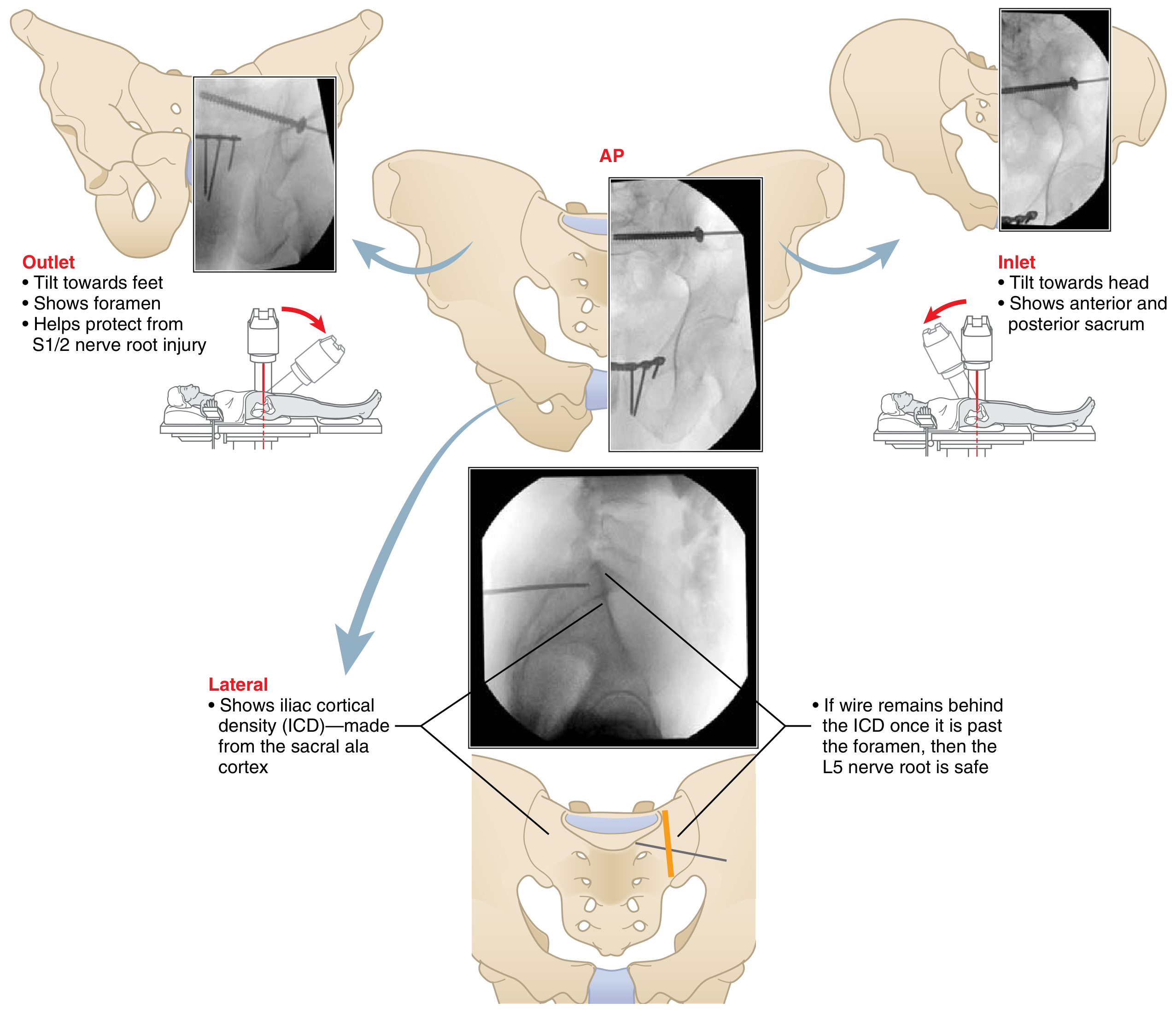
| Inlet (beam tilted toward head) | AP displacement of SI joint; internal/external rotation; anterior/posterior sacral breach during screw placement |
| Outlet (beam tilted toward feet) | Vertical displacement; S1/S2 neural foramina; protects from nerve root injury during screw placement |
| Lateral sacral | Iliac cortical density (ICD); L5 nerve root protection |
| Flamingo/single-leg-stance views | Dynamic instability at pubic symphysis — useful in subacute setting |
| CT scan | Posterior injury patterns; sacral dysmorphism; 3D reconstruction for acetabulum |
Key principle: CT in a binder/sheet may underestimate injury severity.
3. Pelvic Ring Injuries — Classification
Young-Burgess Classification (mechanism-based)
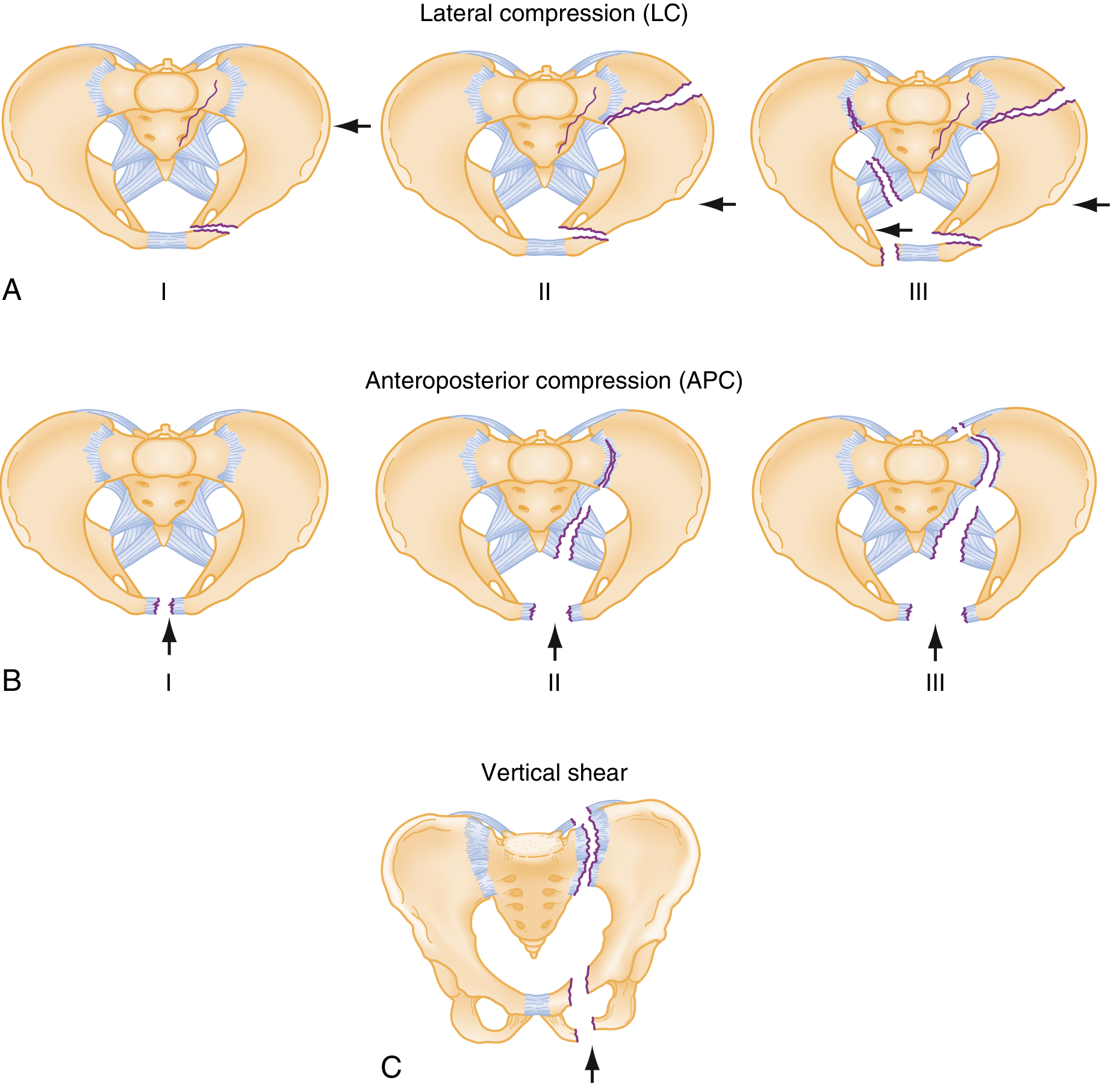
Lateral Compression (LC) — all have anterior transverse pubic ramus fracture
| Type | Posterior Lesion | Key Features |
|---|---|---|
| LC I | Sacral compression fracture | Stable |
| LC II | Posterior iliac wing "crescent" fracture | — |
| LC III | Contralateral APC injury ("windswept pelvis") | Rollover mechanism; crush injury pattern; other organs typically spared |
Cause of death in LC pattern = primarily brain injury.
Anteroposterior Compression (APC) — all have symphyseal diastasis
| Type | Diastasis | Ligament Disruption | Key Features |
|---|---|---|---|
| APC I | < 2.5 cm | Anterior SI ligaments stretched | Stable |
| APC II | > 2.5 cm | Sacrotuberous + sacrospinous + anterior SI ruptured | Anterior SI joint opens; ORIF + posterior fixation lowers failure rate |
| APC III | > 2.5 cm | All SI ligaments (anterior + posterior) ruptured | Complete hemipelvis separation; highest transfusion requirements |
Cause of death in APC pattern = shock, sepsis, ARDS.
Associated injuries: urethral + bladder injuries; rising incidence of vascular/visceral injury APC I → III.
Vertical Shear (VS)
- Fall mechanism; vertical fractures through rami + complete posterior disruption
- Vertical displacement of hemipelvis; equivalent to APC III in instability
- Mortality and transfusion requirements similar to APC II/III
Combined Mechanism (CM)
- Organ injury pattern similar to lower-grade APC and LC patterns
Stable types: LC I and APC I
High hemorrhage risk: APC II, APC III, LC III, VS
Tile Classification (stability-based)
| Type | Stability | Examples |
|---|---|---|
| A | Stable (posterior arch intact) | Avulsion, iliac wing, transverse sacral fractures |
| B | Rotationally unstable, vertically stable | External rotation: anterior pelvic disruption ± anterior SI lig; LC: ipsilateral / contralateral (bucket-handle) / bilateral |
| C | Completely unstable (posterior arch disrupted) | Unilateral, bilateral-mixed (one B, one C), bilateral C |
4. Emergency Management
Life-threatening hemorrhage — 85% from venous injury (internal iliac plexus); only 15% arterial.
Priority sequence:
- Apply pelvic binder or sheet immediately if increased pelvic volume is identified — reduces pelvic volume and tamponades venous bleeding
- Skeletal traction for vertical instability
- Resuscitation — volume + early transfusions
- CT scan to evaluate for arterial injury
- Angiographic embolization if arterial source confirmed
- Pelvic packing (retroperitoneal) — excellent for venous tamponade; popularized in Europe
⚠️ Always establish and follow a treatment protocol to reduce variation in decision-making.
5. Treatment of Pelvic Ring Injuries
Nonoperative
- Indications: stable fracture patterns (LC I, APC I)
- Weight bearing as tolerated for isolated anterior injuries
- Protected weight bearing for combined anterior + posterior ring injuries
Operative Indications
- Symphysis diastasis > 2.5 cm
- Anterior + posterior SI ligament disruption
- Vertical instability of posterior hemipelvis
- Sacral fracture displacement > 1 cm
Anterior Injuries
| Option | Notes |
|---|---|
| ORIF with plate fixation | Avoids pin tract complications; biomechanically superior for symphysis |
| External fixation (AIIS or iliac wing pins) | AIIS biomechanically stronger; iliac wing better tolerated clinically; risk to lateral femoral cutaneous nerve |
| Anterior subcutaneous internal fixator (INFIX) | Reduced dissection; risk of femoral nerve injury (impairs quad function); lateral femoral cutaneous nerve injury in ~1/3; HO most common complication (usually asymptomatic) |
Posterior Injuries
| Option | Notes |
|---|---|
| Percutaneous iliosacral or trans-sacral screws | Trans-sacral > iliosacral in stability; mandatory fluoroscopic landmark identification before surgery (AP, inlet, outlet, lateral views — see diagram below) |
| Anterior plate fixation across SI joint | — |
| Posterior transiliac sacral bars or sacral plating | — |
| Spinal-pelvic fixation | Bilateral sacral fractures; triangular osteosynthesis has high implant prominence/pain rate |
| Most stable construct for vertically unstable anterior + posterior dislocations | Anterior ring internal fixation + percutaneous SI screw |
6. Sacral Fractures
Denis Classification (zone relative to foramen)
| Zone | Location | Neurologic Risk |
|---|---|---|
| Zone I | Lateral to foramina (sacral ala) | Low |
| Zone II | Through foramina | L5 nerve root most common; highest incidence of urologic injury |
| Zone III | Central (sacral canal) | Cauda equina syndrome |
H-fracture / U-fracture — bilateral Zone II/III injuries; assess sagittal CT reformats for kyphosis.
Sacral Dysmorphism (20–44% of population)
Sacralization of L5 or lumbarization of S1. Creates anterosuperior sacral concavity — high risk of anterior screw penetration causing neurologic injury.
Outlet view signs: prominent mammillary processes, laterally downsloping sacral ala, vestigial disc space between S1–S2, iliac crest at level of L5–S1, non-circular S1 tunnel.
Treatment
- Nonoperative: stable/minimally displaced; weight bearing as tolerated for incomplete fractures where ilium is contiguous with intact sacrum (e.g., LC impaction fractures); touch-toe WB for complete fractures
- Operative (displaced > 1 cm): percutaneous IS/trans-sacral screws; posterior plating; transiliac sacral bars; open foraminal decompression for neurologic injury in Zone II
Complications
- Urologic injury (highest with displaced Zone II)
- L5 nerve root injury (Zone II)
- Cauda equina syndrome (Zone III)
- Chronic low back pain, malunion
7. Acetabular Fractures
Mechanism
- Flexed hip with axial load ("dashboard mechanism") — most common
- Pattern determined by position of hip and direction of impact
Radiographic Evaluation
AP pelvis — 6 cardinal lines:
- Posterior wall
- Anterior wall
- Roof
- Teardrop
- Ilioischial line
- Iliopectineal line
| View | Profiles |
|---|---|
| Obturator oblique (affected hip up 45°) | Anterior column + posterior wall |
| Iliac oblique (affected hip down 45°) | Posterior column + anterior wall |
CT (thin-cut 1–2 mm): posterior injuries, articular fragments, marginal impaction, hip congruency, 3D reconstruction with femur subtracted.
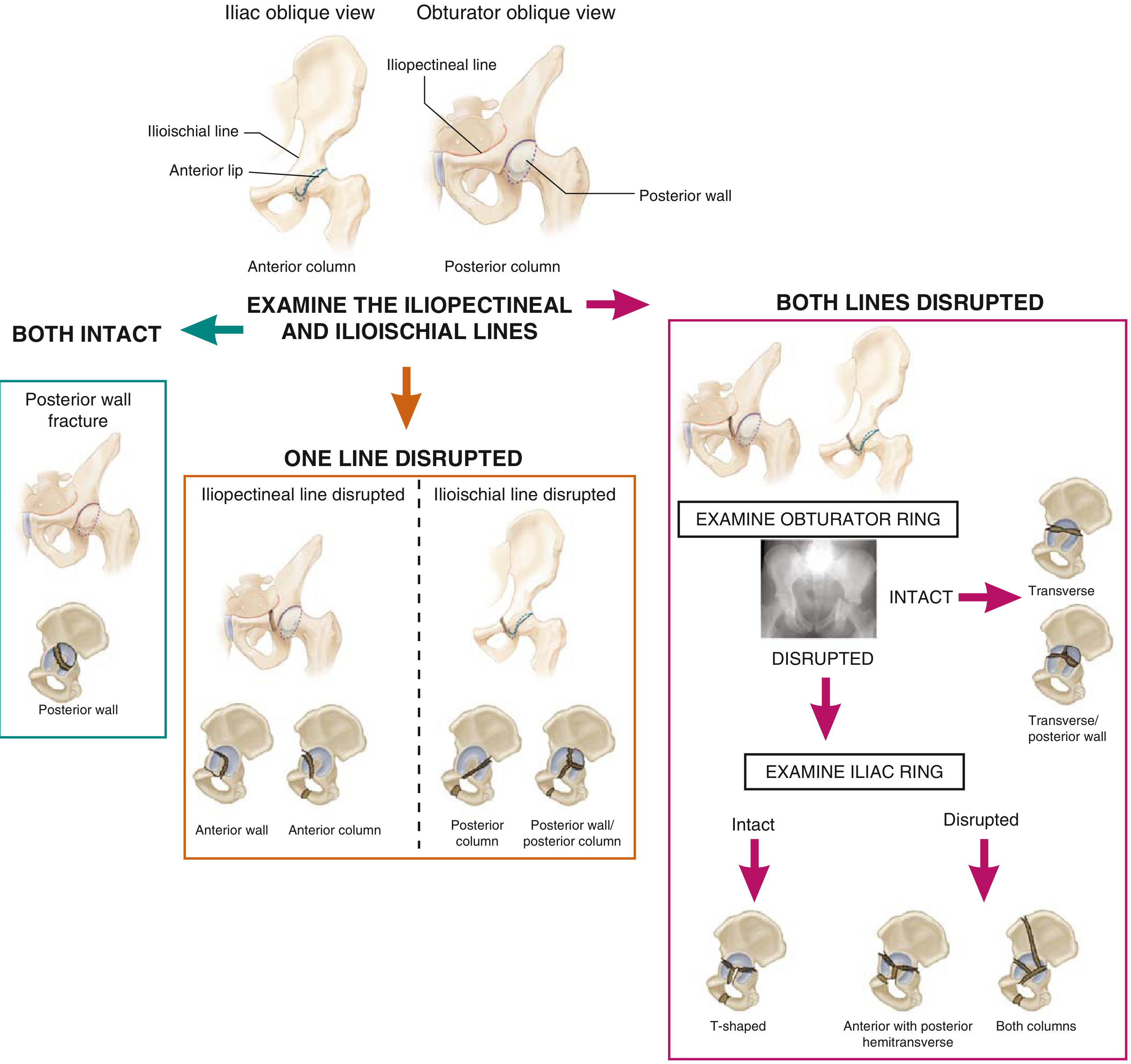
Letournel Classification
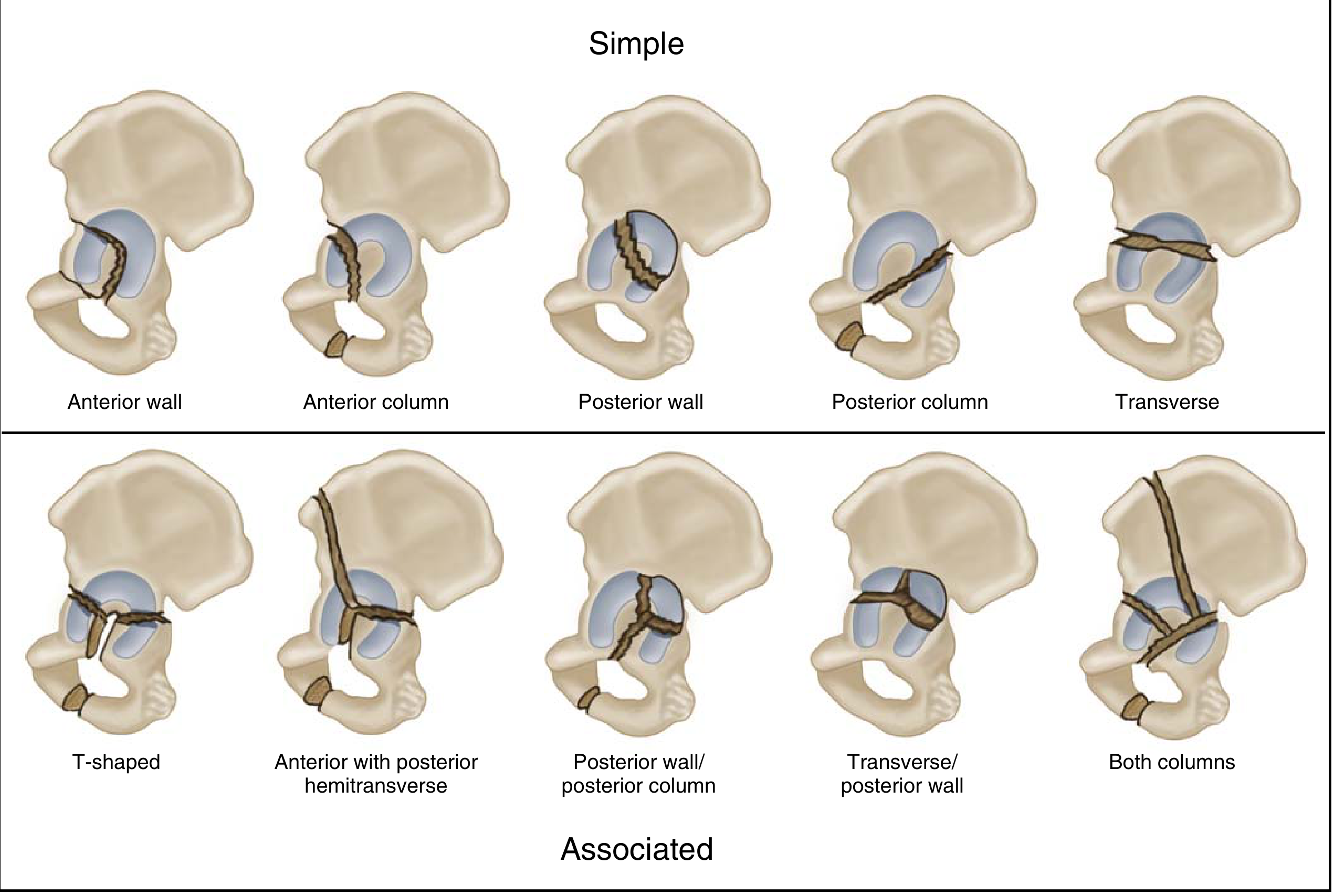
Simple (5 types):
- Posterior wall (PW) — most common simple type
- Posterior column (PC)
- Anterior wall (AW)
- Anterior column (AC)
- Transverse (involves both columns)
Associated (5 types):
- Posterior column + posterior wall
- Transverse + posterior wall
- T-type
- Anterior column + posterior hemitransverse (AC/PHT)
- Both-column (ABC fracture) — spur sign on obturator oblique = intact iliac wing remaining in anatomic position; no intact articular support from acetabulum to axial skeleton on sequential axial CT
Treatment Principles
- Restore articular congruity and hip stability
- Avoid injury to blood supply of femoral head
- DVT screening and prophylaxis
- During surgery: hip extended, knee flexed to reduce sciatic nerve tension
Surgical Approaches
| Approach | Used For | Notes |
|---|---|---|
| Kocher-Langenbeck (posterior) | PW, PC, PC/PW, transverse/PW | Prone or lateral decubitus |
| Ilioinguinal (anterior) | AC, AW, AC/PHT, both-column (without posterior impaction) | Three windows |
| Stoppa/modified Stoppa | Low AC, quadrilateral plate, both-column | Intrapelvic access |
| Extensile approaches (combined, extended iliofemoral, triradiate) | > 3 weeks old; complex associated fractures; PC reduction needed | Higher HO risk |
| ORIF + acute THA | Age > 60 with gull sign (superomedial dome impaction); associated femoral neck fracture; significant pre-existing arthrosis | — |
Percutaneous Fixation
- PC screw: retrograde (ischium, hip flexed) or antegrade (mini lateral window approach); use Judet images for trajectory
- AC screw: through superior ramus OR supra-acetabular corridor; use obturator oblique outlet (shows corridor + avoids joint), iliac oblique (avoids inferior breach), obturator inlet (avoids medial/lateral breach)
Complications
| Complication | Key Points |
|---|---|
| DVT/PE | Preoperative screening; IVC filter if DVT present preoperatively |
| Heterotopic ossification (HO) | Extended iliofemoral > Kocher-Langenbeck > anterior approach (50% → 25% → 10%); prophylaxis: indomethacin or 600 cGy radiation within 48h |
| Sciatic nerve injury | Associated with posterior dislocations; < 50% full recovery; peroneal division most vulnerable; transverse + PW = highest nerve injury rate |
| Osteonecrosis (AVN) | Highest with posterior fracture-dislocations; iatrogenic damage to medial femoral circumflex artery |
| Morel-Lavallée lesion | Soft tissue degloving; associated with higher infection rates |
| Posttraumatic arthritis | Leading long-term complication |
8. Risk Factors for Death
Identified during initial treatment:
- Blood transfusion requirement in first 24 hours
- Unstable fracture type: APC II, APC III, LC II, LC III, VS, combined mechanism
- Open fracture
Key Mnemonics & High-Yield Points
- "Open book" = APC injury → apply binder to close the book
- Stable = LC I and APC I; everything else warrants close attention
- 85% of pelvic hemorrhage is venous — binder + packing first; angio only if arterial source confirmed
- Posterior wall = most common simple acetabular fracture
- Both-column fracture = spur sign on obturator oblique; only fracture with secondary congruence (femoral head stays congruent with displaced fragments)
- Zone II sacral fracture = L5 nerve root most at risk; highest urologic injury
- Zone III sacral fracture = cauda equina
- Sacral dysmorphism in 20–44% — increases risk of screw penetration; recognize on outlet view
- ICD (iliac cortical density) = landmark for safe IS screw placement; screw must remain posterior to ICD
Miller's Review of Orthopaedics, 9th ed., pp. 907–915 | Rockwood & Green's Fractures in Adults, 10th ed., 2025, pp. 2313ff.
Congenital dislocation of hip. Torticollis (Stiffneck).Congenital clubfoot.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the material needed. Here are the complete orthopaedic notes.
Paediatric Orthopaedics — Congenital Conditions
Sources: Miller's Review of Orthopaedics (9th ed.); Schwartz's Principles of Surgery (11th ed.); The Developing Human — Clinically Oriented Embryology (Moore & Persaud)
PART 1: Developmental Dysplasia of the Hip (DDH) / Congenital Dislocation of the Hip (CDH)
1. Definition
Abnormal development or dislocation of the hip secondary to capsular laxity and mechanical factors (e.g., intrauterine positioning). The term DDH is now preferred over CDH as it reflects the full spectrum of the condition.
2. Spectrum of Disease
| Type | Description |
|---|---|
| Dysplasia | Shallow acetabulum, femoral head in joint |
| Subluxation | Partial loss of contact between femoral head and acetabulum |
| Dislocation | Complete loss of contact |
| Teratologic | Dislocated in utero, irreducible at birth; associated with neuromuscular conditions (arthrogryposis, Larsen syndrome); pseudoacetabulum present at or near birth |
| Late dysplasia | Adolescent/adult presentation |
3. Risk Factors
(In descending order of importance)
- Breech positioning — highest risk (30–50%)
- Positive family history (ligamentous laxity) — ≥20%
- Female sex — 85% of cases
- Firstborn child (less intrauterine space)
Additional associations:
- Left hip most commonly affected (67% of cases)
- Increased maternal oestrogens
- Postnatal: swaddling with hips in extension
- Associated conditions: torticollis (20%), metatarsus adductus (10%); no association with clubfoot
4. Pathoanatomy — Obstacles to Concentric Reduction
If left untreated, muscles contract and the acetabulum becomes more dysplastic and fills with fibrofatty tissue (pulvinar).
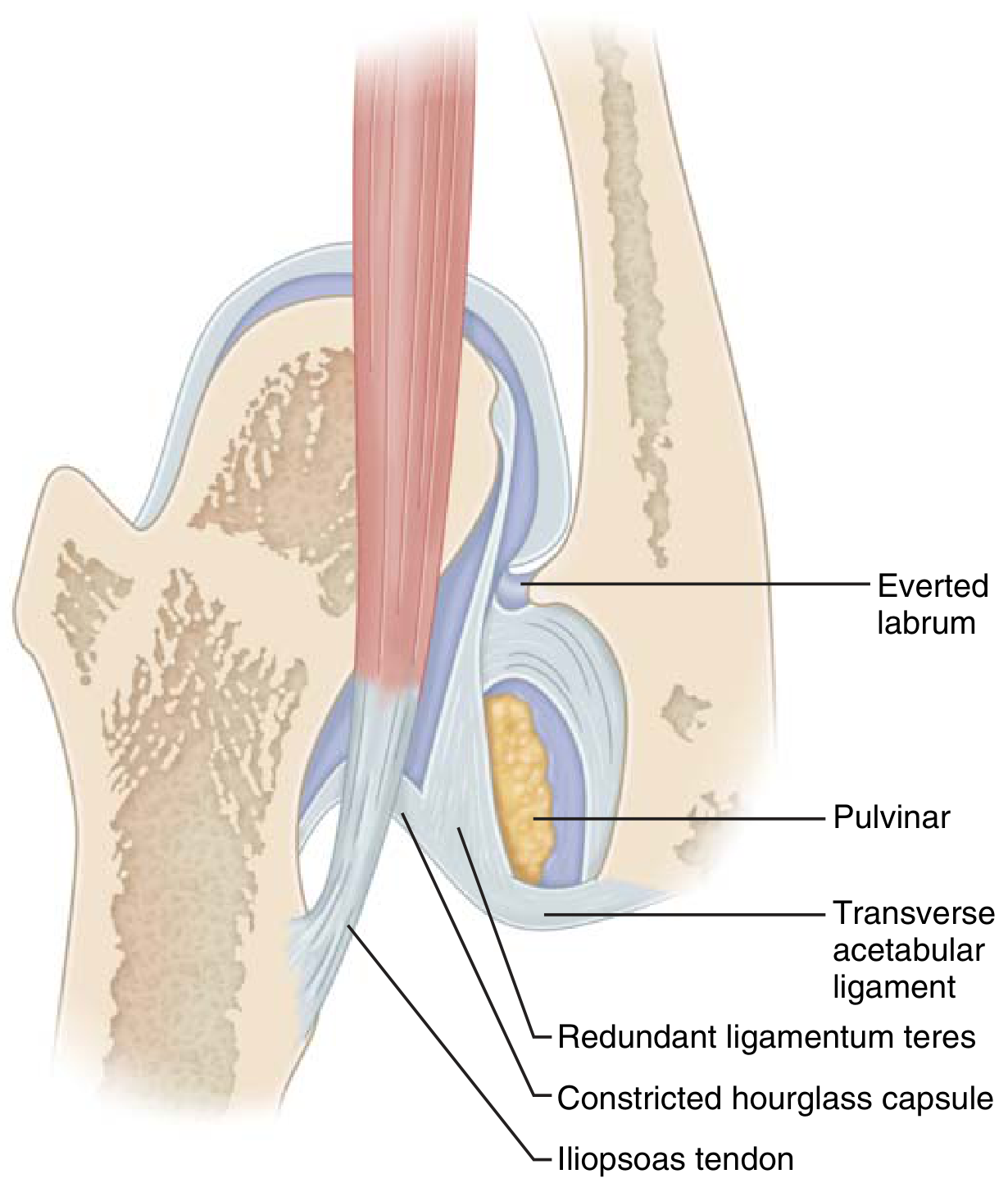
Obstacles to reduction:
- Iliopsoas tendon
- Pulvinar (fibrofatty tissue)
- Hypertrophied ligamentum teres
- Contracted inferomedial hip capsule
- Transverse acetabular ligament
- Inverted (infolded) labrum
5. Diagnosis
Clinical Examination
| Test | Mechanism | Positive Finding |
|---|---|---|
| Ortolani test | Elevation + abduction of flexed hip | Clunk = dislocated hip reduces (positive early; negative late when irreducible) |
| Barlow test | Adduction + depression of hip | Clunk = reduced hip dislocates |
| Galeazzi sign | Feet together, knees flexed | Foreshortened femur on affected side |
| Limited hip abduction | Passive ROM | Asymmetric restriction as laxity resolves |
| Asymmetric gluteal folds | Inspection | Less reliable |
| Trendelenburg gait | Walking child | Older children with untreated DDH |
⚠️ In bilateral dislocation, abduction may appear symmetrically decreased — easily missed.
Ultrasound (< 4–6 months of age)
- Dynamic ultrasound — investigation of choice before femoral head ossification
- Normal α angle > 60° on coronal view; femoral head bisected by iliac line
- Useful to assess reduction in Pavlik harness and diagnose capsular laxity
Radiographs (> 4 months)
- Acetabular index — normal < 25°
- Perkin line — ossific nucleus should be medial to this line
- Shenton line — disrupted in dislocation
- Delayed ossification of femoral head on affected side
Advanced Imaging
- Arthrography — assesses adequacy of closed reduction; look for "thorn sign" (normal labral position)
- CT or MRI post-reduction — confirms concentric reduction
6. Treatment (age-dependent)
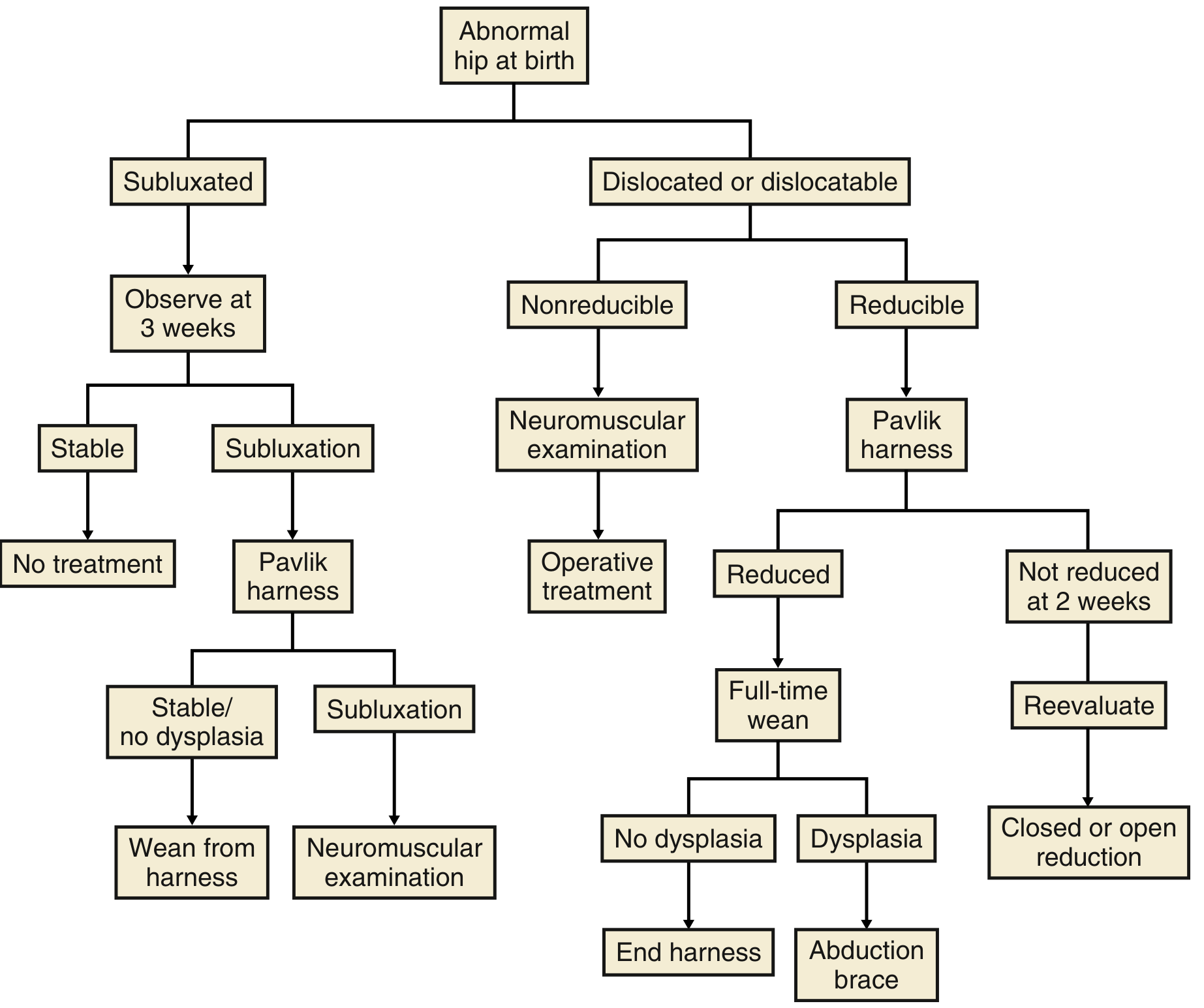
| Age | Treatment |
|---|---|
| Birth – 6 months | Pavlik harness for Ortolani-positive hips; closely watch Barlow-positive; repeat ultrasound at 6 weeks |
| 6 – 18 months | Arthrography, percutaneous adductor tenotomy, closed reduction + hip spica cast; if fails → open reduction |
| 18 months – 3 years | Open reduction + femoral shortening osteotomy ± acetabular osteotomy |
| 3 – 8 years | Acetabular osteotomy (Salter, Dega, Pemberton, Staheli) |
| > 8 years | Triple (Steele), double pelvic (Sutherland), Staheli [open physis]; Ganz or Chiari [closed physis] |
| Adult | Total hip arthroplasty |
Note: Diagnosis after age 8 years (age 6 in bilateral DDH) may contraindicate reduction as the acetabulum has little remodelling capacity.
Pavlik Harness — Key Points
- Designed for infants < 6 months
- Maintains ~100° flexion + mild abduction ("human position" / Salter position)
- Must be within the safe zone of Ramsey (between maximum adduction before redislocation and excessive abduction causing AVN)
- Worn 23h/day for ≥ 6 weeks after reduction, then part-time 6–8 weeks
- Contraindicated in teratologic dislocations
- Excessive flexion → transient femoral nerve palsy
- If not reduced within 3 weeks → discontinue ("Pavlik disease") to prevent acetabular erosion
Pavlik harness failure risk factors:
- Age > 7 weeks at initiation
- Bilateral dislocations
- Absence of Ortolani sign
Pelvic Osteotomies (summary table)
| Osteotomy | Type | Key Feature |
|---|---|---|
| Salter | Redirectional (open-wedge) | May lengthen limb up to 1 cm; requires open triradiate cartilage |
| Pemberton | Volume-reducing | Bends on triradiate cartilage; good for residual dysplasia |
| Dega | Volume-reducing | Preferred for paralytic dislocations; posterior deficiency |
| Ganz (PAO) | Redirectional | Triradiate must be closed; superior 3D correction; single incision; preserves abductors |
| Steel / Sutherland | Triple/double innominate | Open triradiate; uses Salter cut + additional cuts |
| Chiari | Salvage/medialisation | Closed triradiate |
7. Complications
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) | Most feared; caused by vascular injury or excessive abduction in harness; medial open reduction has higher AVN rate |
| Redislocation | — |
| Residual dysplasia | May require further osteotomy |
| Stiffness | Especially after prolonged spica casting |
| Leg length discrepancy | — |
| Degenerative joint disease | Long-term outcome if poorly treated |
PART 2: Congenital Muscular Torticollis (CMT) / "Wry Neck" / "Stiff Neck"

1. Definition
Lateral bending of the head towards the affected side with slight rotation of the chin away from the affected side, caused by fibrosis and shortening of the sternocleidomastoid (SCM) muscle.
2. Pathogenesis
- Tearing of SCM fibres during childbirth → haematoma → necrosis + fibrosis of muscle fibres
- Histology: deposition of collagen and fibroblasts around atrophied muscle cells
- Also occurs in caesarean births → additional causes include intrauterine crowding and primary SCM myopathy
- A palpable SCM mass is present in approximately two-thirds of cases (also diagnosable by USS)
3. Clinical Features
- Head tilts to the side of the lesion
- Chin rotates away from the lesion
- Palpable firm mass in the SCM in ~2/3 of cases
- If untreated → plagiocephaly (facial asymmetry) and facial hemihypoplasia on the affected side
- Associated with DDH in 20% of cases; associated with other intrauterine positioning abnormalities
4. Differential Diagnosis
| Condition | Key Differentiator |
|---|---|
| Atlantoaxial rotatory subluxation (Grisel syndrome) | Associated with pharyngeal infections; rotation with lateral tilt; no SCM mass |
| Klippel-Feil syndrome | Cervical vertebral fusion; short neck |
| Ocular torticollis | Head tilt compensates for extraocular muscle imbalance |
| Sprengel deformity | Elevated scapula; may restrict head movement |
Torticollis is secondary to fibrosis of the sternal head of SCM — a palpable mass within SCM is a key distinguishing feature from atlantoaxial subluxation.
5. Treatment
- Physiotherapy (passive stretching of the affected SCM) — effective in the vast majority of cases; recommended from as early as possible
- Stretching: tilt head to opposite side and rotate chin towards affected side
- Surgical transection of the SCM — reserved for refractory/resistant cases that do not respond to conservative management (rare); performed when:
- Persistent after 1 year of conservative treatment
- Significant facial asymmetry
- Restricted ROM after age 1 year
- Surgery involves bipolar SCM release; complications include haematoma and scar
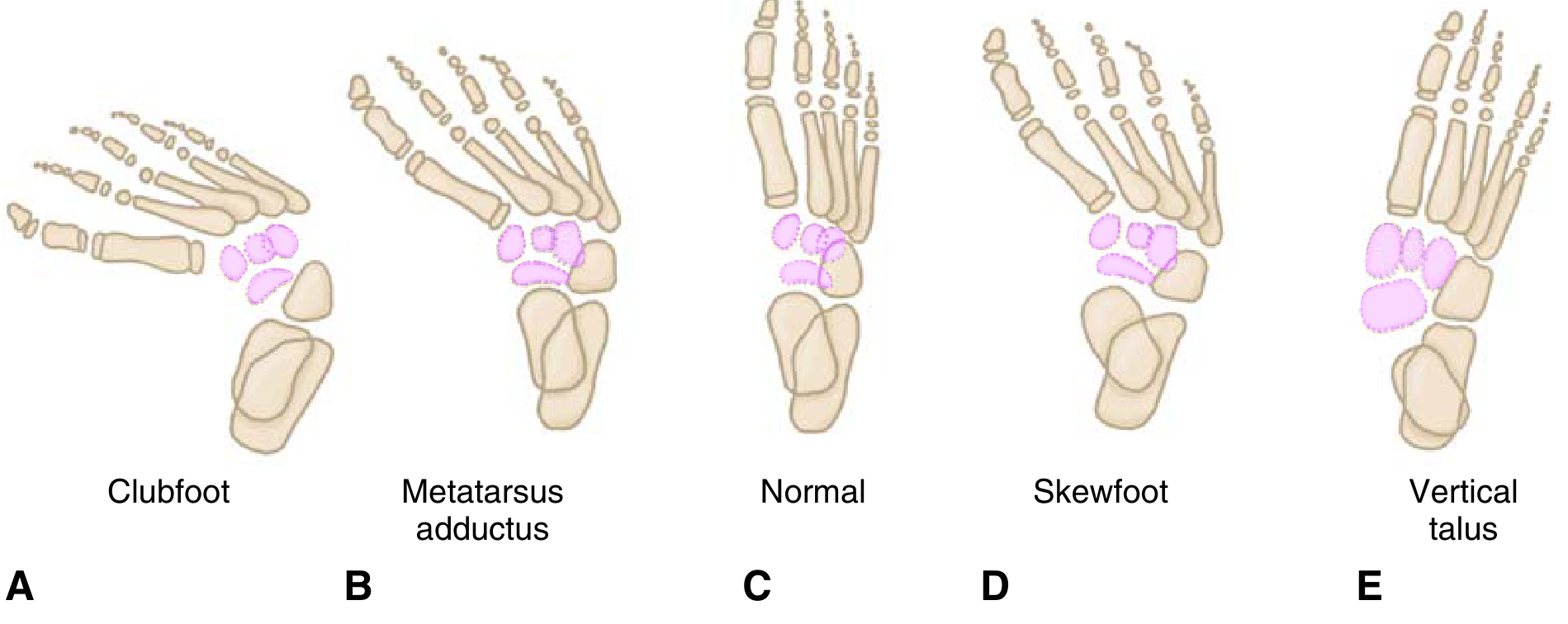
PART 3: Congenital Clubfoot (Congenital Talipes Equinovarus — CTEV)
1. Deformity Components — Mnemonic: CAVE
| Letter | Deformity | Explanation |
|---|---|---|
| C | Cavus | High arch — forefoot plantarflexed relative to hindfoot |
| A | Adductus | Forefoot adducted |
| V | Varus | Hindfoot varus |
| E | Equinus | Plantarflexion of the whole foot |
Underlying deformity: Talar neck — medial and plantar deviation, with medial rotation of calcaneus and medial displacement of navicular and cuboid.
Shortened/contracted structures: intrinsic muscles, Achilles tendon, tibialis posterior, flexor hallucis longus, flexor digitorum longus, joint capsules, ligaments, and fascia.
Associated: absence or diminutive anterior tibial artery.
2. Epidemiology
- Boys affected twice as often as girls
- 50% bilateral
- Incidence: ~1–2 per 1,000 live births
3. Aetiology
- Majority idiopathic, but strong genetic component (PITX1-TBX4 transcriptional pathway)
- Associated conditions:
- Arthrogryposis
- Myelomeningocele
- Streeter dysplasia (hand anomalies)
- Diastrophic dwarfism
- Prune-belly syndrome
- Tibial hemimelia
4. Imaging
Radiographs rarely used in infants (minimal ossification). When used:
| View | Measurement | Normal | Clubfoot |
|---|---|---|---|
| AP (Kite angle) | Talocalcaneal angle | 20–40° | Decreased (parallelism of calcaneus and talus) |
| Dorsiflexion lateral (Turco) | Talocalcaneal angle | ~35° | < 35° (decreased) |
| AP | Talus–1st metatarsal angle | 0–20° | Negative |
5. Treatment
Ponseti Method (first-line; 95% success for idiopathic cases)
Serial weekly manipulation and long-leg plaster casts — corrects deformities in reverse order of CAVE:
| Step | What is Corrected | How |
|---|---|---|
| 1st cast | Cavus | Supinate forefoot + dorsiflex 1st ray |
| Subsequent casts | Adductus + Varus | Lateral pressure on distal talar head as fulcrum |
| Last cast | Equinus | 70° of abduction |
- 90% of patients require percutaneous Achilles tendon lengthening at end of casting to address hindfoot equinus
- Last cast placed in 70° abduction
- Foot abduction brace (FAB) mandatory after casting — non-compliance is the main cause of recurrence
Surgical Treatment
- Reserved for refractory/resistant cases (~5% of idiopathic presentations)
- Posterior tibial artery must be protected (dorsalis pedis often insufficient)
- Procedures:
- Tendon lengthening
- Subtalar, tibiotalar, and talonavicular release + realignment
- Older children (3–10 years): medial opening-wedge or lateral column-shortening osteotomy or cuboid decancellation for adductus
- Late presentation: triple arthrodesis (contraindicated in insensate feet — causes rigidity → ulceration)
6. Complications of Treatment
| Complication | Key Details |
|---|---|
| Dynamic supination | Most common post-treatment deformity (15–20%); overpull of tibialis anterior with weak peroneus longus; treat with tibialis anterior transfer laterally |
| Dorsal bunion | After clubfoot surgery; strong tibialis anterior + flexor hallucis brevis/abductor hallucis; may be iatrogenic (peroneus longus division); treated with capsulotomy, FHL lengthening, FHB transfer to MTP |
| Recurrence | Especially with non-compliance with brace |
| Avascular necrosis of talus | Post-surgical over-release |
| Stiffness / restricted ROM | |
| Flat-top talus | Overly aggressive casting/surgery |
Summary Comparison Table
| Feature | DDH | Torticollis | Clubfoot |
|---|---|---|---|
| Sex predilection | Female (85%) | None significant | Male (2:1) |
| Laterality | Left hip (67%) | Contralateral to mass | 50% bilateral |
| Key test | Ortolani / Barlow | Passive cervical ROM; SCM mass | CAVE on inspection |
| Primary Rx | Pavlik harness (< 6 mo) | Passive stretching physiotherapy | Ponseti casting |
| Surgery threshold | Failed conservative / older child | Resistant after 1 year | Refractory (~5%) |
| Genetic pathway | Multifactorial, laxity genes | — | PITX1-TBX4 |
| Associated condition | Metatarsus adductus, torticollis | DDH (20%) | Arthrogryposis, myelomeningocele |
Miller's Review of Orthopaedics, 9th ed., pp. 264–268, 282–283 | Schwartz's Principles of Surgery, 11th ed. | The Developing Human, Moore & Persaud, p. 965
Residual consequence of flaccid poliomyelitis. Cerebral palsy.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.