Human Heart
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
I have comprehensive content from authoritative anatomy textbooks with multiple anatomical diagrams. I now have everything needed to write a thorough, well-illustrated answer.
The Human Heart
The human heart is a fibromuscular, hollow organ with a roughly pyramidal shape. It sits obliquely in the thorax, with one-third of its mass to the right and two-thirds to the left of the midline. Below is a complete overview covering gross anatomy, chambers, valves, vasculature, and conduction.
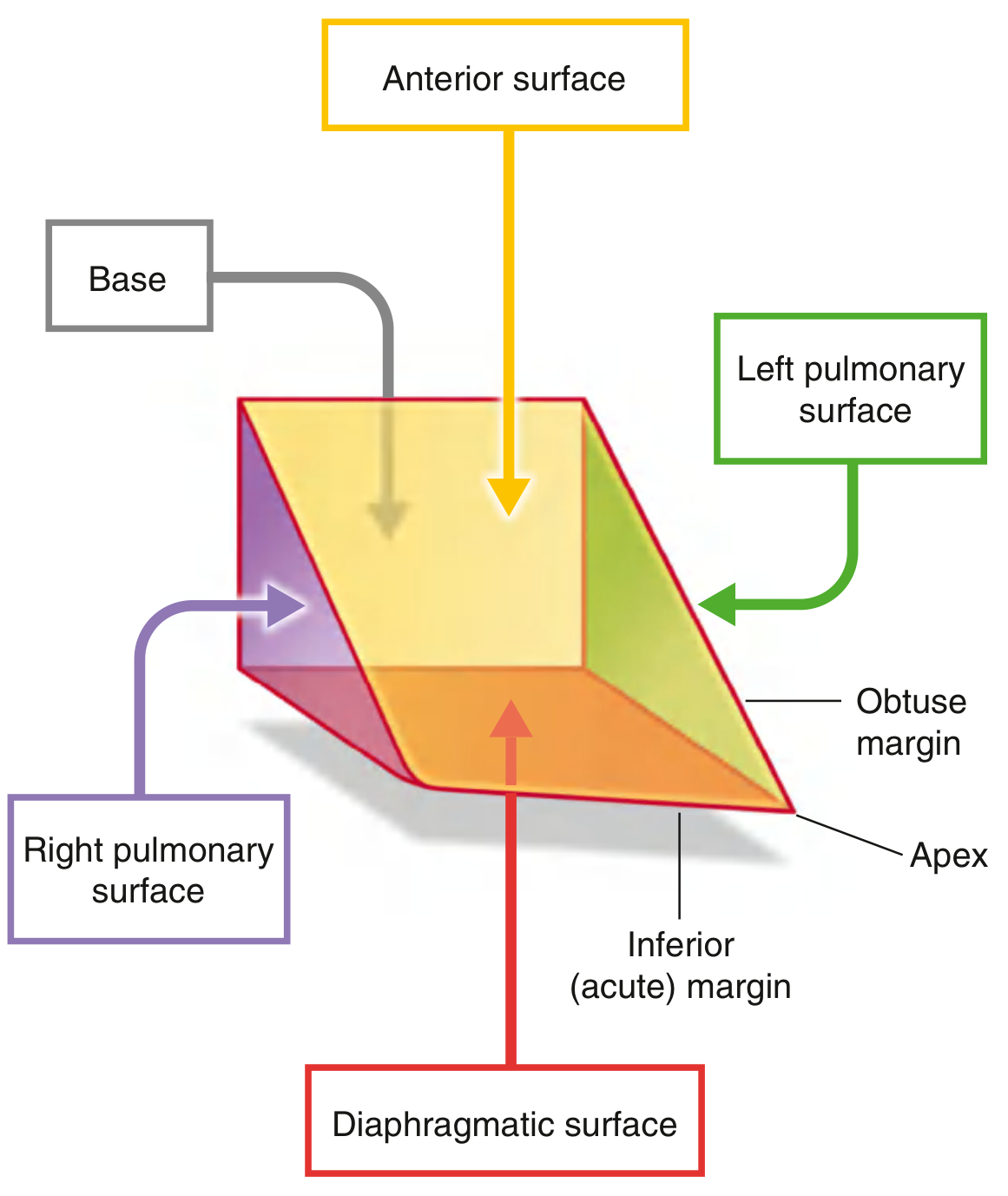
Shape, Position, and Surfaces
The heart resembles a pyramid that has "fallen over" and rests on one of its sides. Four surfaces are described:
| Surface | Formed by |
|---|---|
| Anterior (sternocostal) | Mostly right ventricle, some right atrium and left ventricle |
| Diaphragmatic (inferior) | Left ventricle (mostly) + small portion of right ventricle |
| Left pulmonary | Left ventricle + portion of left atrium |
| Right pulmonary | Right atrium |
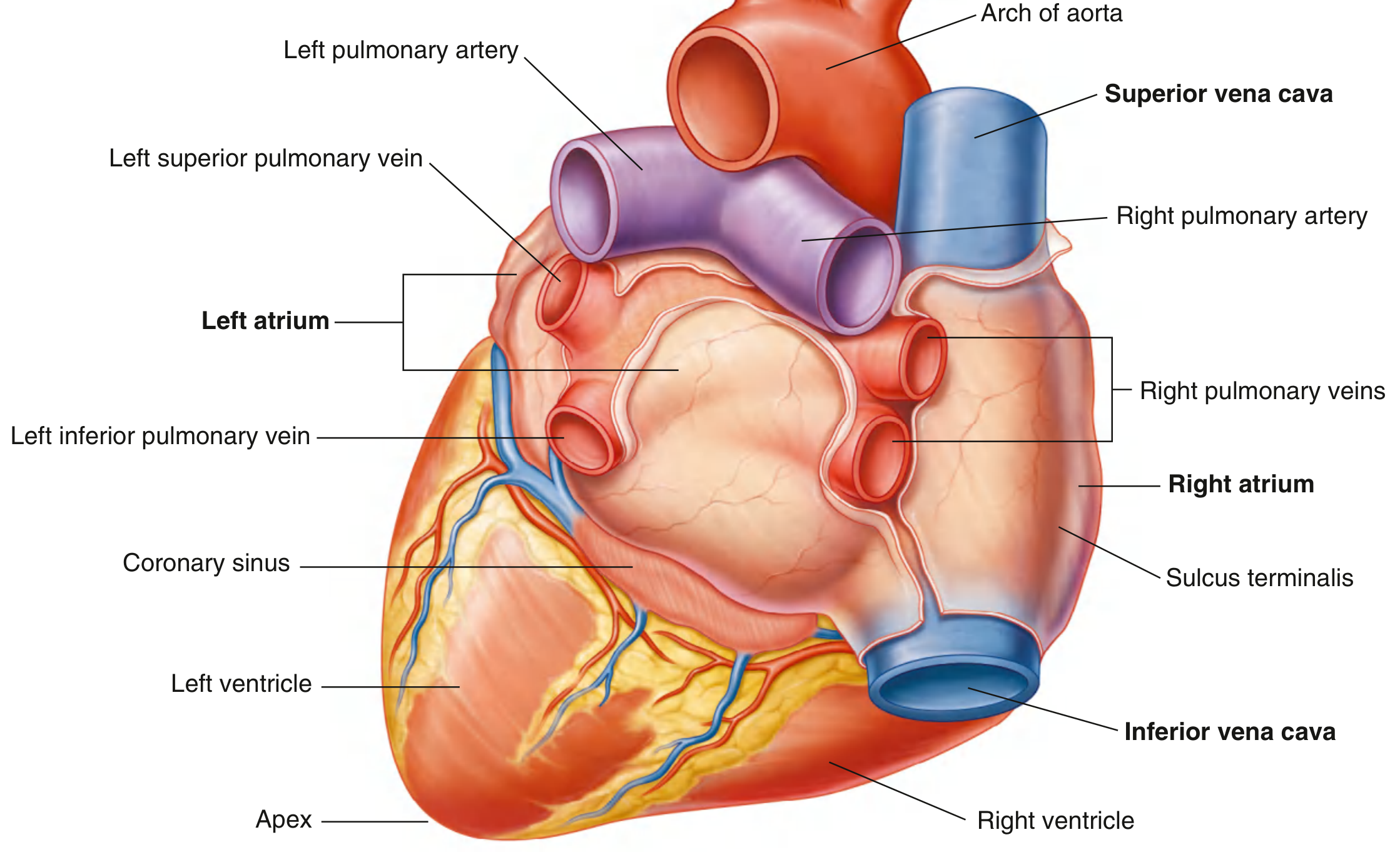
The apex points forward, downward, and to the left, resting deep to the left 5th intercostal space, 8-9 cm from the midsternal line. The base faces posteriorly and is formed by the left atrium, a small part of the right atrium, and the proximal great veins (superior/inferior venae cavae and pulmonary veins).
Gross External View (Posterior/Base)
The Four Chambers
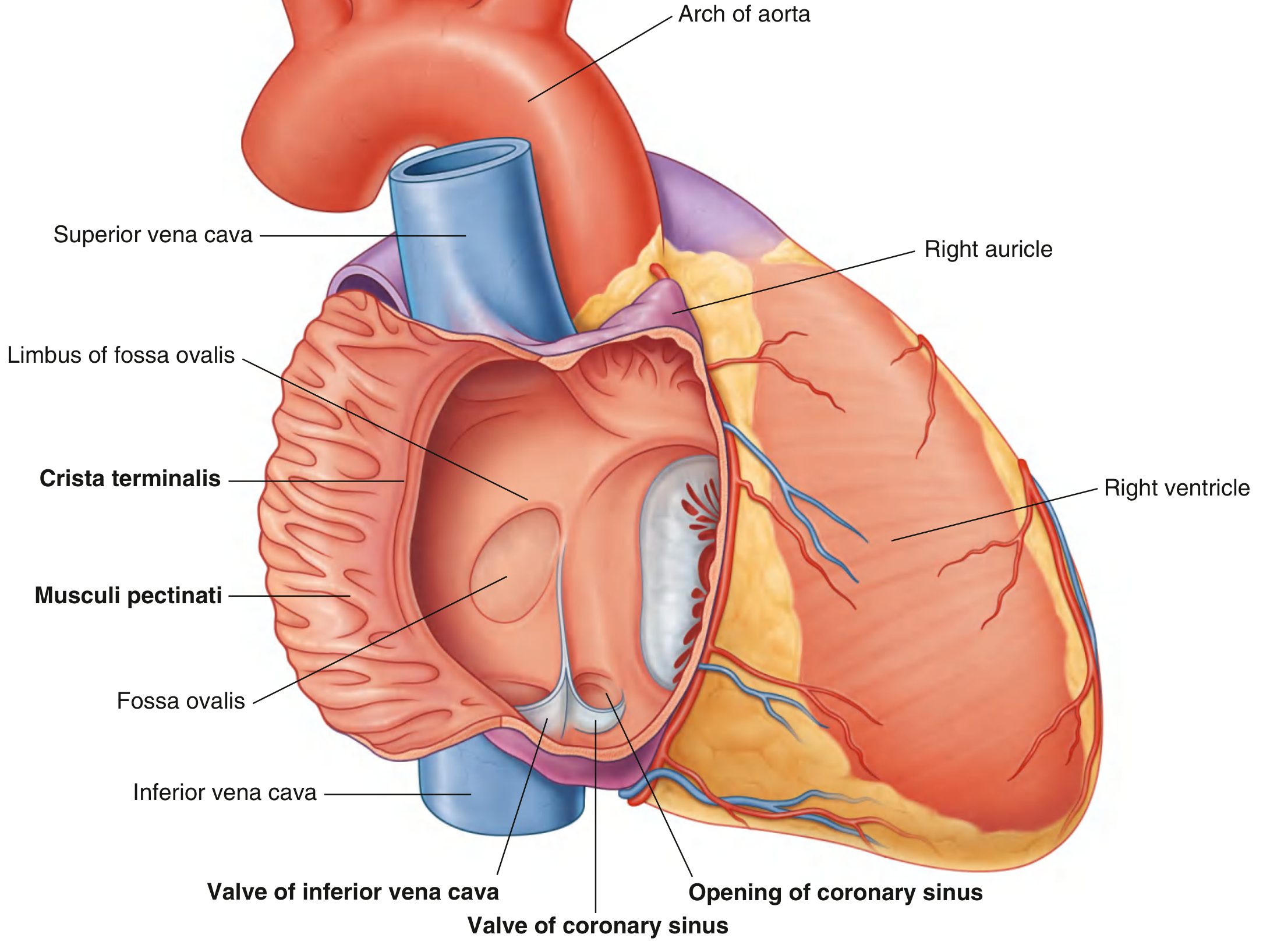
Right Atrium
Receives deoxygenated blood from the body via the superior vena cava (from the head/upper limbs) and inferior vena cava (from the lower body), and venous drainage from the myocardium via the coronary sinus. The interior is divided by the crista terminalis into:
- A smooth posterior region (sinus of venae cavae) derived from the embryonic sinus venosus
- An anterior region covered by musculi pectinati (comb-like ridges), including the right auricle
The fossa ovalis on the interatrial septum is the remnant of the fetal foramen ovale, which allowed oxygenated blood to bypass the lungs before birth.
Right Ventricle
Forms most of the anterior surface. Blood exits through the pulmonary valve into the pulmonary trunk toward the lungs. The interior has prominent trabeculae carneae (irregular muscle ridges), papillary muscles, and chordae tendineae that anchor the tricuspid valve (right atrioventricular valve, with three cusps: anterior, posterior, and septal).
Left Atrium
Receives oxygenated blood from the lungs via four pulmonary veins (two from each side). Its posterior half has smooth walls; its anterior half contains musculi pectinati and the left auricle. It forms most of the base of the heart.
Left Ventricle
The "workhorse" of the heart. It is conical, longer than the right ventricle, and has the thickest myocardial wall (to generate systemic arterial pressure). Blood exits through the aortic valve into the ascending aorta. The outflow tract is called the aortic vestibule. Two papillary muscles (anterior and posterior) with chordae tendineae control the mitral (bicuspid) valve.
The interventricular septum has a thick muscular part and a thin membranous part superiorly.
The Four Valves
| Valve | Type | Location | Function |
|---|---|---|---|
| Tricuspid | Atrioventricular (3 cusps) | Right AV orifice | Prevents backflow from RV to RA during systole |
| Pulmonary | Semilunar (3 cusps) | RV outflow | Prevents backflow from pulmonary trunk to RV |
| Mitral (Bicuspid) | Atrioventricular (2 cusps) | Left AV orifice | Prevents backflow from LV to LA during systole |
| Aortic | Semilunar (3 cusps) | LV outflow | Prevents backflow from aorta to LV; sinuses of Valsalva feed coronary arteries |
The aortic and pulmonary valves are semilunar - each has three pocket-like cusps that fill with blood during diastole, snapping the valve shut. The right and left aortic sinuses are the origin sites of the coronary arteries - as blood recoils after ventricular contraction, it is automatically forced into these vessels.
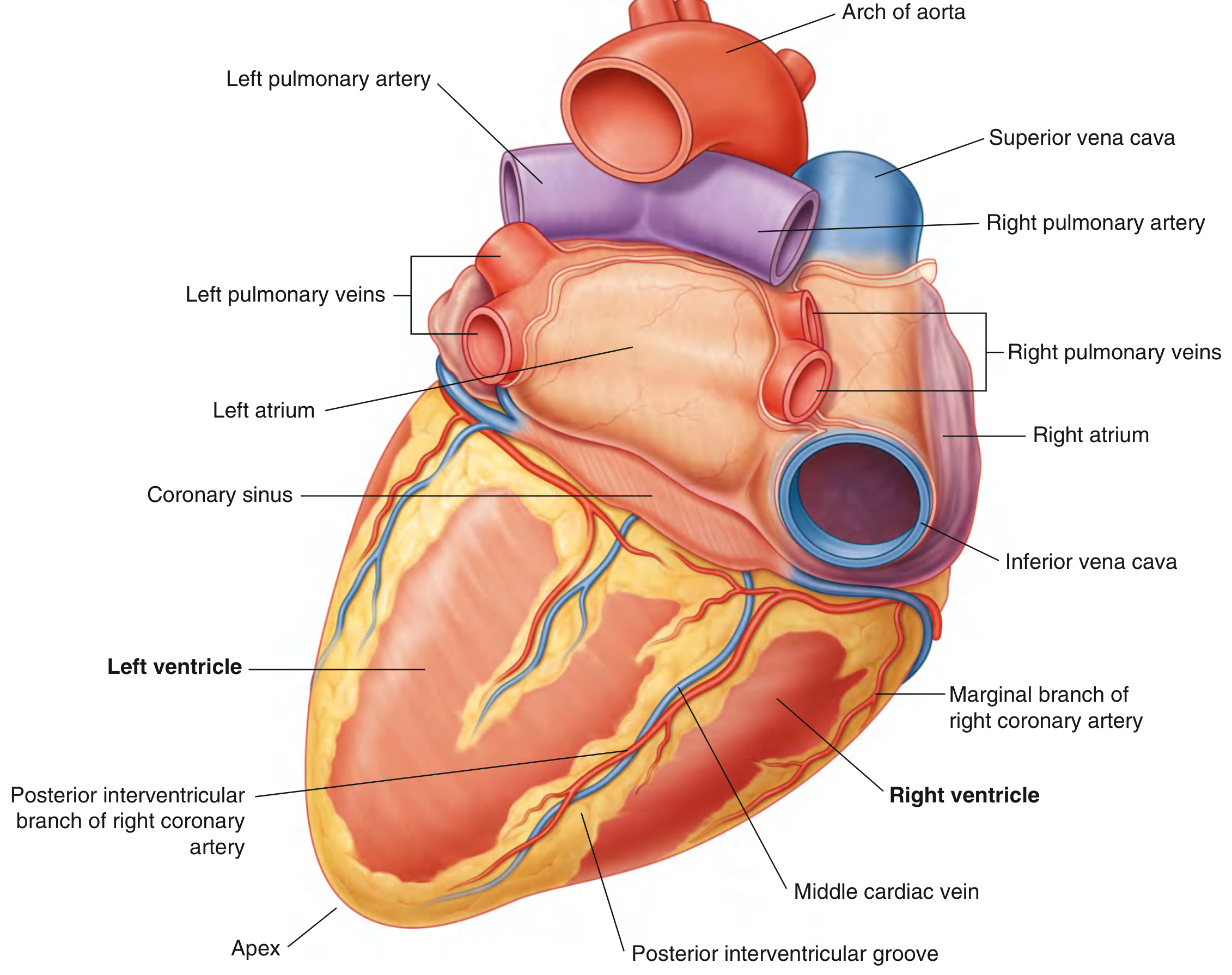
Coronary Circulation
The heart's own blood supply comes from two coronary arteries arising from the aortic sinuses:
- Right coronary artery (RCA) - travels in the coronary sulcus; gives off the posterior interventricular artery (supplies posterior interventricular groove in ~80% of people, termed "right dominant" circulation); also supplies the SA and AV nodes in most people
- Left coronary artery (LCA) - divides into:
- Anterior interventricular (left anterior descending, LAD) artery - runs in the anterior interventricular sulcus; supplies the anterior wall of both ventricles and the anterior 2/3 of the interventricular septum
- Circumflex artery - runs in the coronary sulcus on the left side; supplies the left atrium and posterior left ventricle
Venous drainage flows mainly into the coronary sinus (visible on the diaphragmatic surface) and then into the right atrium.
Wall Layers
The heart wall has three layers:
- Epicardium (visceral pericardium) - outermost serous layer; contains the coronary vessels and fat
- Myocardium - thick muscular middle layer; responsible for contraction
- Endocardium - smooth inner lining; continuous with the endothelium of blood vessels
The heart is enclosed in the fibrous pericardium with an inner serous pericardium creating a pericardial cavity with a thin film of fluid to reduce friction.
Conduction System
The cardiac conduction system generates and propagates electrical impulses for coordinated contraction:
- SA node (sinoatrial node) - the natural pacemaker, located near the superior vena cava opening in the right atrium; fires at ~60-100 bpm
- AV node (atrioventricular node) - at the base of the interatrial septum; delays the impulse by ~120 ms to allow atrial contraction to fill the ventricles
- Bundle of His - passes through the membranous septum
- Right and left bundle branches - travel down each side of the interventricular septum
- Purkinje fibers - fan out through ventricular myocardium, causing near-simultaneous contraction
Innervation
The heart receives dual autonomic innervation:
- Sympathetic (thoracic cardiac nerves, T1-T5): increases heart rate and force of contraction
- Parasympathetic (vagus nerve, CN X): slows heart rate; dominant at rest
Visceral afferent fibers (pain from ischemia) travel with sympathetic fibers and refer pain to the left arm, jaw, and chest (referred cardiac pain).
Key Clinical Points
- The left ventricle wall is ~3x thicker than the right ventricle due to the higher resistance of the systemic circulation
- Mitral stenosis is most commonly caused by rheumatic fever; stenosis develops decades after initial infection
- Aortic stenosis is the most common cardiac valve disease in adults and is usually caused by atherosclerotic calcification
- Coronary artery disease most frequently affects the LAD (the "widow maker"), causing anterior MI
- The fossa ovalis may remain probe-patent in up to 25% of adults (patent foramen ovale), usually clinically silent but a risk for paradoxical embolism
Sources: Gray's Anatomy for Students (9780323934237), Color Atlas of Human Anatomy Vol. 2 Internal Organs (9783132424487)
This is a shared conversation. Sign in to Orris to start your own chat.