CBD
Asking for Preferences
Reading File
Searching the Web
CBD cannabidiol medical uses evidence 2025 2026
Searching PubMed
cannabidiol CBD therapeutic effects
Finding Sources
Reading Article
PMID: 38924898
Reading File
Reading File
Here is a thorough overview of CBD (cannabidiol) drawing from pharmacology references and recent evidence:
Cannabidiol (CBD)
What It Is
CBD is a nonintoxicating phytocannabinoid derived from Cannabis sativa. Unlike THC, it produces no psychoactive "high." It is available as a pharmaceutical-grade oral solution (Epidiolex) and in a wide range of over-the-counter products (oils, gummies, topicals).
Mechanism of Action
CBD works through multiple targets rather than a single receptor pathway (Goodman & Gilman's, p. 417):
- CB1/CB2 receptors - CBD has low direct binding affinity for these endocannabinoid receptors. It acts as a negative allosteric modulator at CB1 and as an inverse agonist at CB2, and it inhibits the reuptake/hydrolysis of anandamide.
- TRPV1 (vanilloid receptor) - activation, relevant for pain and inflammation.
- GPR55 - antagonism, reduces presynaptic calcium and neuronal excitability.
- 5-HT1A receptors - activation, relevant to anxiolytic and antidepressant effects.
- Adenosine (ENT-1 inhibition) - increases adenosine tone, which suppresses seizure activity.
FDA-Approved Uses (Epidiolex)
CBD is FDA-approved (since 2018) for seizures associated with:
- Dravet syndrome
- Lennox-Gastaut syndrome
- Tuberous sclerosis complex
Approved for patients aged 1 year and older. The EU's EMA has granted orphan drug status for the same indications (Goodman & Gilman's, p. 418).
Evidence for Other Conditions
| Condition | Evidence Level |
|---|---|
| Epilepsy (above) | Strong - FDA-approved RCTs |
| Anxiety (GAD, SAD, PTSD) | Moderate - 2024 meta-analysis (n=316) showed significant effect size (Hedges' g = -0.92), but small sample sizes limit conclusions [PMID: 38924898] |
| Chronic pain / inflammation | Preclinical evidence strong; clinical evidence limited and mixed |
| Parkinson's disease symptoms | Emerging - systematic reviews ongoing [PMID: 37253174] |
| Psychosis | Interest exists but efficacy not yet established |
| Sleep | Anecdotal/low-quality evidence; no approved indication |
Pharmacokinetics
- Route: Oral only (prescription form)
- Bioavailability: ~6% fasting; increases 4-fold with a high-fat meal
- Half-life: 18-32 hours (longer with repeated dosing, up to 60+ h at steady state)
- Metabolism: Primarily CYP2C19 (hydroxylation to 7-OH-CBD) and CYP3A4 (further oxidation). Active metabolite 7-OH-CBD retains antiepileptic activity.
- Excretion: Mostly fecal, small amounts urinary
Safety and Side Effects
Common adverse effects at antiepileptic doses:
- Somnolence, fatigue
- Decreased appetite
- Diarrhea
- Elevated liver transaminases - ALT >3x ULN in >10% of patients at 10-25 mg/kg/day. Risk nearly doubles with valproate co-administration. Monitoring required.
Drug Interactions (Important)
CBD inhibits CYP3A4 and CYP2C19, creating significant interaction potential:
- Clobazam - CBD dramatically raises clobazam and nor-clobazam plasma levels. Monitoring essential.
- Valproate - does not raise valproate levels, but doubles the risk of liver enzyme elevation.
- Many other CYP-metabolized drugs can be affected (see nephrology drug interaction tables).
Legal and Regulatory Status (2026)
- Prescription CBD (Epidiolex) is FDA-approved and Schedule V.
- Over-the-counter CBD products exist in a legal gray area; the FDA has not approved them as dietary supplements.
- In December 2025, President Trump signed Executive Order 14370 directing NIH, FDA, and CMS to expand real-world evidence research on CBD and medical cannabis, acknowledging the gap between widespread use and established evidence.
Bottom Line
CBD has one well-established medical use (treatment-resistant epilepsy in children and adults) backed by strong RCT data. For anxiety, pain, and other conditions, early evidence is promising but not yet sufficient for routine clinical recommendation. It has a real drug interaction profile and can cause liver injury at higher doses, so it is not risk-free despite being "natural."
Choledocholithiasis
Reading File
Finding Sources
Searching PubMed
choledocholithiasis management ERCP
Searching the Web
choledocholithiasis diagnosis management guidelines 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Excellent - I have comprehensive content. Here is the full clinical overview:
Choledocholithiasis (Common Bile Duct Stones)
Definition and Prevalence
Choledocholithiasis is the presence of gallstones within the common bile duct (CBD). It occurs in up to 20% of patients with cholelithiasis. Up to a third of patients with CBD stones may pass them spontaneously, but the majority require intervention.
Stone Types
| Type | Origin | Composition | Notes |
|---|---|---|---|
| Secondary (most common in US) | Migrated from gallbladder | Cholesterol or black pigment | Most common type overall |
| Primary | Formed de novo in CBD | Brown pigment (bile pigment + cholesterol) | Associated with bacterial infection, more common in Asian populations |
| Retained | Missed at cholecystectomy | Any | Identified within 2 years post-op; occurs in 1-2% of cases |
Primary brown stones form because bacteria release hydrolyzing enzymes that free bilirubin, which precipitates and crystallizes in the duct.
Clinical Presentation
Presentation ranges from entirely asymptomatic (incidental finding) to life-threatening:
- Biliary colic - RUQ or epigastric pain, often colicky, may radiate to the back or right shoulder
- Obstructive jaundice - painful onset (distinguishes from malignancy, where obstruction is gradual/painless), dark urine, scleral icterus, acholic (pale) stools, pruritus
- Cholangitis (Charcot's triad: fever + jaundice + RUQ pain) - present in <50% of cases; progression to Reynolds pentad (+ hypotension + altered mental status) signals septic shock with ~100% mortality without urgent decompression
- Gallstone pancreatitis - elevated lipase (>3x ULN), epigastric pain
Diagnosis
Labs
| Finding | Significance |
|---|---|
| Elevated total bilirubin | Low sensitivity, high specificity for choledocholithiasis |
| Elevated ALP | Often the most prominent LFT abnormality |
| Elevated AST/ALT | Present with hepatocellular injury from obstruction |
| Leukocytosis | Raises concern for cholangitis |
| Lipase >3x ULN | Suggests concurrent pancreatitis |
Elevated bilirubin + abnormal ultrasound together push the probability of choledocholithiasis toward ~90%. Normal US + normal LFTs: probability falls to <5%.
Imaging
Transabdominal ultrasound (US)
- First-line, widely available
- Specificity ~90%, sensitivity ~80% for CBD stones
- Can directly visualize stones or show CBD dilation (>6 mm in average adult; >8 mm in patients >65 years or post-cholecystectomy)
- Stone visualization itself is less common than detecting ductal dilation
MRCP (MR Cholangiopancreatography)
- Non-invasive, excellent sensitivity/specificity
- Preferred confirmatory test in intermediate-risk patients before committing to ERCP
ERCP (Endoscopic Retrograde Cholangiopancreatography)
- Both diagnostic and therapeutic; preferred when intervention is already planned
- Below is an intraoperative cholangiogram showing a CBD stone (arrow):
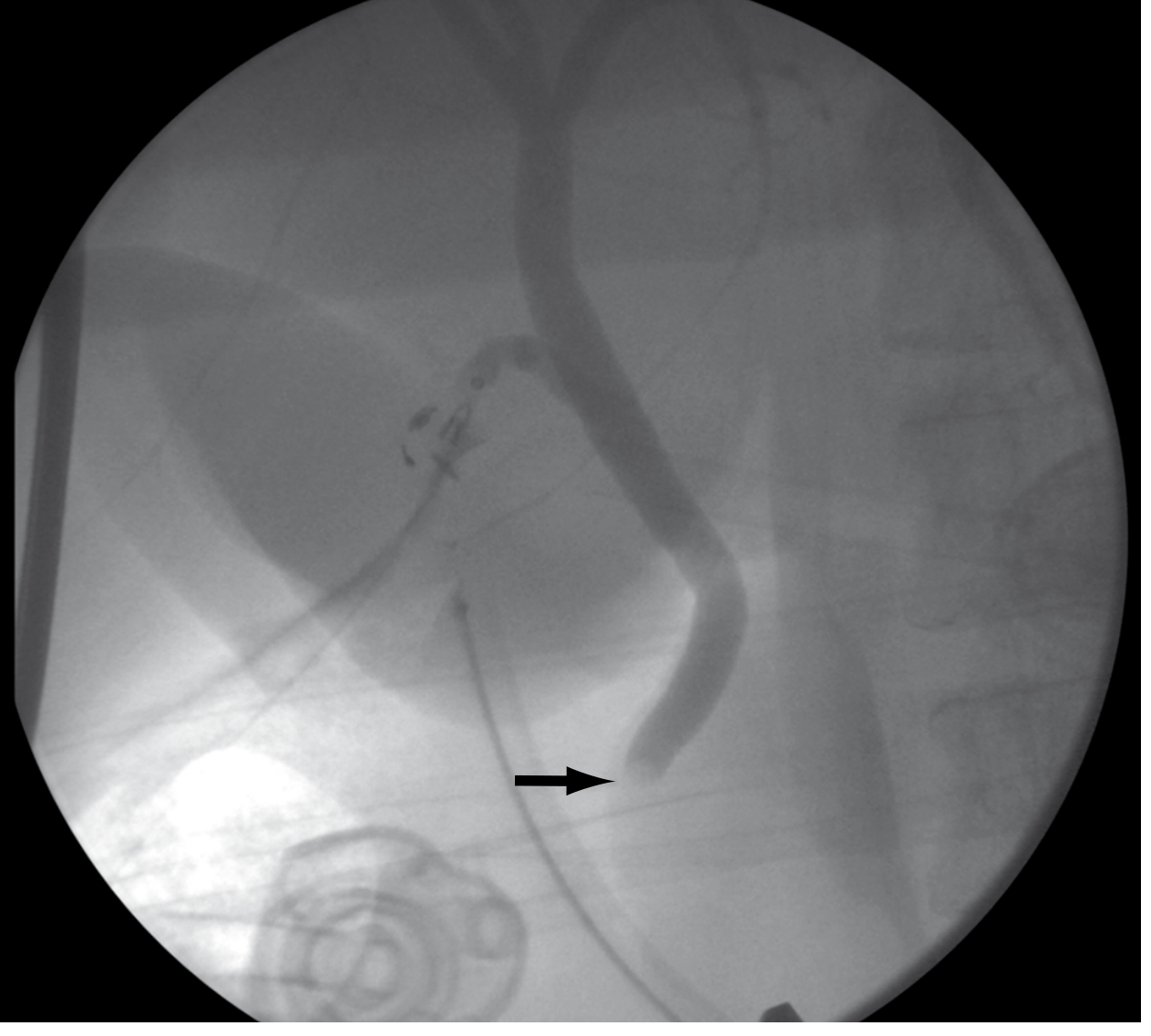
Intraoperative cholangiogram showing choledocholithiasis: filling defect (arrow) with no contrast filling the duodenum - Sabiston Textbook of Surgery
Risk Stratification (ASGE Guidelines)
ASGE and SAGES guidelines classify patients into low, intermediate, and high risk to guide next steps:
| Risk Category | Features | Action |
|---|---|---|
| High (>50% probability) | Bilirubin >4 mg/dL + CBD stone on US, OR cholangitis, OR bilirubin 1.8-4 + dilated CBD | Proceed directly to ERCP |
| Intermediate | Some but not all high-risk features | MRCP or EUS first |
| Low (<10% probability) | Normal LFTs, normal US | Proceed to cholecystectomy without further workup |
A 2025 systematic review [PMID 40569779] found that both ASGE 2019 and ESGE guidelines perform comparably - their strength is ruling out CBD stones in low-risk patients, but both have limited specificity for identifying high-risk patients who need upfront ERCP.
Management
1. ERCP (Primary Treatment)
90% of CBD stones can be removed with standard ERCP. Steps:
- Biliary cannulation - wire-guided approach preferred to reduce post-ERCP pancreatitis risk
- Endoscopic sphincterotomy - required for stone removal; creates access through the papilla
- Stone extraction - balloon or basket retrieval
- Large stones (>1.5 cm) - partial sphincterotomy + balloon sphincteroplasty, or lithotripsy (mechanical, electrohydraulic [EHL], laser, or extracorporeal shock wave)
For unstable/sick patients, a biliary stent or nasobiliary tube (NBT) can temporarily drain the duct, followed by definitive stone clearance later.
If difficult cannulation (>5 attempts, >5 minutes, or >1 unintended pancreatic duct cannulation): double wire technique or precut fistulotomy can be used.
ERCP failure (5-10% of cases even with expert endoscopists) is more likely with: stones >2.5 cm, altered anatomy (Roux-en-Y), impacted stones, intrahepatic stones, or multiple stones.
2. Surgical Common Bile Duct Exploration (CBDE)
Can be performed laparoscopically, robotically, or open. Two approaches:
- Transcystic (preferred) - via incision in cystic duct
- Transcholedochal - direct CBD incision; for stones too large or proximal for transcystic access
Stone clearance rates average 95% with laparoscopic CBDE. RCTs show laparoscopic cholecystectomy + CBDE results in lower morbidity/mortality and shorter hospital stay vs. two-stage ERCP then laparoscopic cholecystectomy, when performed by experienced surgeons.
3. Percutaneous Transhepatic Cholangioscopy (PTCS)
Reserved for patients where ERCP fails (altered post-surgical anatomy, high intrahepatic stones). Complete stone removal in ~90% of cases. Requires ~2 weeks of external biliary drainage first to prevent cholangitis. Lithotripsy (laser preferred over electrohydraulic for precision) used for large stones. Recurrence is reported in up to one-third of patients with intrahepatic stones, especially in the setting of intrahepatic strictures.
4. Cholecystectomy
Because >50% of patients managed by ERCP alone (without cholecystectomy) will develop recurrent biliary tract symptoms, same-admission laparoscopic cholecystectomy is strongly advised after successful ERCP.
Complications
| Complication | Key Point |
|---|---|
| Ascending cholangitis | Occurs in ~5% of admitted patients with choledocholithiasis; bactibilia in ~90% with obstruction. Common pathogens: Klebsiella, E. coli, Enterobacter, Pseudomonas, Citrobacter. Requires urgent antibiotics + biliary decompression. |
| Gallstone pancreatitis | CBD stone impaction at ampulla of Vater triggers pancreatic duct obstruction |
| Post-ERCP pancreatitis | Most common serious ERCP complication; risk reduced by wire-guided cannulation |
| Biliary cirrhosis | Long-term consequence of untreated chronic obstruction |
Sources: Sabiston Textbook of Surgery, p. 1832-1834 | Sleisenger & Fordtran's GI and Liver Disease, p. 1267-1270 | Clinical Gastrointestinal Endoscopy, p. 843-844 | Current Surgical Therapy, 14e, p. 571-572
This is a shared conversation. Sign in to Orris to start your own chat.