Ace inhibitors
Reading File
Finding Sources
Searching PubMed
"ACE inhibitors" AND "cardiovascular outcomes"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of ACE inhibitors drawn from multiple authoritative textbooks.
ACE Inhibitors (Angiotensin-Converting Enzyme Inhibitors)
Mechanism of Action
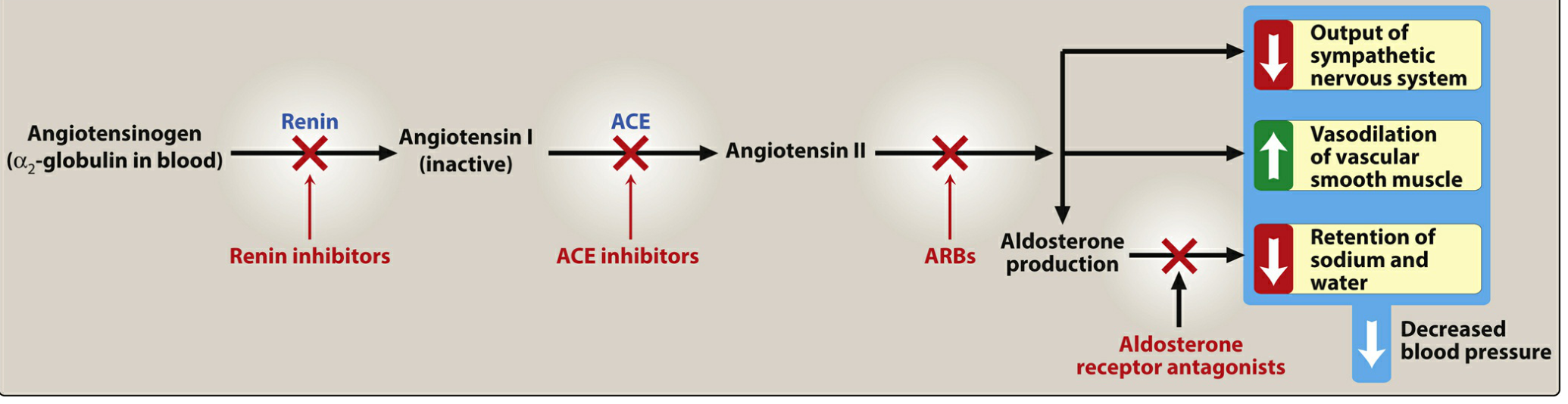
ACE inhibitors block the enzyme responsible for two key reactions:
- Conversion of angiotensin I → angiotensin II (a potent vasoconstrictor)
- Breakdown of bradykinin (a vasodilator that stimulates nitric oxide and prostacyclin release)
The net result is:
- Reduced angiotensin II → less vasoconstriction, less aldosterone secretion → less sodium/water retention
- More bradykinin → enhanced vasodilation
- Dilation of both arterioles and veins → reduced cardiac preload and afterload
- Efferent arteriolar dilation in the kidney → reduced intraglomerular pressure (protective in nephropathy)
Drugs in This Class
| Drug | Brand Name | Notes |
|---|---|---|
| Captopril | (generic) | Short-acting; 3x/day dosing |
| Enalapril | Vasotec | Prodrug; IV form (enalaprilat) available |
| Lisinopril | Prinivil, Zestril | Not a prodrug; once daily |
| Ramipril | Altace | Once or twice daily |
| Fosinopril | (generic) | Only ACE inhibitor NOT renally eliminated - no dose adjustment needed in renal impairment |
| Benazepril | Lotensin | Prodrug |
| Quinapril | Accupril | Prodrug |
| Perindopril | (generic) | Prodrug |
| Trandolapril | (generic) | Prodrug; once daily |
| Moexipril | (generic) | Prodrug |
Pharmacokinetics note: All are orally bioavailable. Most (except captopril and lisinopril) are prodrugs requiring hepatic conversion to active forms - captopril and lisinopril are preferred in severe hepatic impairment. Enalaprilat is the only IV formulation in the class.
Therapeutic Uses
1. Hypertension
First-line agents, especially with compelling indications. All ACE inhibitors are equally effective at equivalent doses. They achieve sustained BP reduction and cause regression of left ventricular hypertrophy.
2. Heart Failure (HFrEF)
Multiple large trials clearly demonstrate improved symptoms and survival in LV systolic dysfunction. ACE inhibitors are first-line alongside beta-blockers, MRAs, and SGLT2 inhibitors for NYHA class II-IV. They also benefit asymptomatic LV dysfunction (NYHA class I). Note: ARNIs (sacubitril/valsartan) are now often preferred over ACE inhibitors in HFrEF.
3. Post-Myocardial Infarction
Standard of care post-MI - improve ventricular remodeling and reduce subsequent events.
4. Diabetic Nephropathy
- In type 1 diabetes: the Collaborative Study Group captopril trial showed a ~50% reduction in risk of serum creatinine doubling and the composite of death/dialysis/transplantation, independent of blood pressure. ACE inhibitors should be started as soon as persistent moderately elevated albuminuria is documented, even if BP is normal.
- In type 2 diabetes: consistently reduce risk of developing albuminuria and slow GFR decline. Ramipril in the HOPE trial significantly reduced cardiovascular events. No evidence of differential efficacy versus ARBs in type 2 DKD.
5. Chronic Kidney Disease (non-diabetic)
Reduce proteinuria and slow CKD progression via intraglomerular pressure reduction.
6. Coronary Artery Disease / High Cardiovascular Risk
First-line in patients with CAD, prior stroke, or high CV risk.
Dosing (Heart Failure - Target Doses)
| Drug | Starting Dose | Target Dose |
|---|---|---|
| Captopril | 6.25 mg TID | 50 mg TID |
| Enalapril | 2.5 mg BID | 10-20 mg BID |
| Lisinopril | 2.5-5 mg OD | 20-35 mg OD |
| Ramipril | 2.5 mg OD | 5 mg BID or 10 mg OD |
| Trandolapril | 0.5 mg OD | 4 mg OD |
(Start low, double dose every 2 weeks as tolerated)
Adverse Effects
| Effect | Mechanism | Notes |
|---|---|---|
| Dry cough | Bradykinin/substance P accumulation in pulmonary tree | Up to 10% of patients; more common in women; resolves within days of stopping |
| Angioedema | Excess bradykinin causing swelling of lips, oral mucosa, throat | Rare but life-threatening; absolute contraindication to restarting ACE inhibitors |
| Hyperkalemia | Reduced aldosterone → reduced K+ excretion | Monitor K+; caution with K+ supplements, K+-sparing diuretics, MRAs, NSAIDs |
| Hypotension | Especially with first dose, in volume-depleted patients | Start low, especially if on diuretics |
| Acute kidney injury / creatinine rise | Reduced efferent arteriolar tone → reduced GFR | A rise in creatinine up to 30% above baseline is acceptable; avoid in bilateral renal artery stenosis |
| Rash / dysgeusia | Mostly with captopril (sulfhydryl group) | |
| Leukopenia | Rare | |
| Teratogenicity | Fetal RAAS inhibition | Contraindicated in pregnancy - causes fetal renal dysgenesis, oligohydramnios |
Contraindications
- History of ACE inhibitor-associated angioedema (absolute)
- Bilateral renal artery stenosis (or unilateral stenosis with solitary kidney)
- Pregnancy (all trimesters - teratogenic)
- Significant hyperkalemia (K+ > 5.0 mmol/L) - relative contraindication
- Severe hypotension (SBP < 90 mmHg) - relative
- Combination with ARNI (sacubitril/valsartan) - risk of angioedema; must wash out ACE inhibitor for 36 hours before starting ARNI
Key Drug Interactions
- K+-sparing diuretics (amiloride, triamterene): hyperkalemia risk
- MRAs (spironolactone, eplerenone): hyperkalemia risk
- ARBs: dual RAAS blockade - increased risk of renal dysfunction, hyperkalemia; generally avoided
- NSAIDs: blunt antihypertensive effect; increase risk of AKI and hyperkalemia
- Lithium: ACE inhibitors reduce lithium excretion - toxicity risk
- Low-salt substitutes (high K+ content): hyperkalemia risk
ACE Inhibitors vs. ARBs
| Feature | ACE Inhibitors | ARBs |
|---|---|---|
| Bradykinin levels | Increased | Modest increase (via AT2 signaling) |
| Cough | Up to 10% | Rare |
| Angioedema | Rare but higher than ARBs | Very rare |
| Renal/CV protection | Equivalent in type 2 DKD | Equivalent |
| Pregnancy | Contraindicated | Contraindicated |
| Cost | Generally cheaper (generic) | Higher cost |
ARBs should be used when ACE inhibitors are not tolerated (primarily due to cough or angioedema). Do not combine ACE inhibitors + ARBs + MRAs (triple RAAS blockade) due to severe hyperkalemia/AKI risk.
Sources: Lippincott Illustrated Reviews: Pharmacology | Goodman & Gilman's The Pharmacological Basis of Therapeutics | Goldman-Cecil Medicine | The Washington Manual of Medical Therapeutics | NKF Primer on Kidney Diseases, 8e
This is a shared conversation. Sign in to Orris to start your own chat.