Explain pharmacotherapy of arrythmias
Reading File
Finding Sources
Finding Sources
Searching PubMed
"antiarrhythmic drugs" AND "arrhythmia"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have more than enough information from multiple authoritative sources (Goodman & Gilman, Harrison's, Katzung) to write a thorough, well-organized answer. Let me compile it.
Pharmacotherapy of Arrhythmias
Physiological Basis
Normal cardiac rhythm depends on precisely timed ion currents - Na⁺ (depolarization), K⁺ (repolarization), and Ca²⁺ (plateau/nodal tissues). Arrhythmias arise from three major mechanisms:
- Abnormal automaticity - ectopic pacemaker discharge (enhanced or abnormal phase 4 depolarization)
- Triggered activity - afterdepolarizations (early [EADs] or delayed [DADs]) from abnormal Ca²⁺ handling or prolonged action potentials
- Reentry - unidirectional block with slow conduction in a circuit, allowing a wavefront to re-excite tissue it has already passed
Antiarrhythmic drugs (AADs) work by suppressing initiating mechanisms or interrupting reentrant circuits. Crucially, they can also cause arrhythmias (proarrhythmia) - a key clinical concern.
The Vaughan-Williams Classification
The traditional framework classifies AADs into four classes based on their primary ion channel targets. Most clinically used drugs have effects across multiple classes.
| Class | Primary Target | Mechanism | Key Drugs |
|---|---|---|---|
| IA | Na⁺ channel (intermediate kinetics) | Moderate Na⁺ block + K⁺ block → slows conduction + prolongs refractoriness | Quinidine, Procainamide, Disopyramide |
| IB | Na⁺ channel (fast kinetics) | Rapid Na⁺ block, preferentially in ischemic tissue; shortens AP duration | Lidocaine, Mexiletine |
| IC | Na⁺ channel (slow kinetics) | Marked Na⁺ block; minimal effect on repolarization | Flecainide, Propafenone |
| II | β-adrenergic receptors | Reduce phase 4 slope, slow AV conduction | Metoprolol, Esmolol, Atenolol |
| III | K⁺ channels | Prolong action potential duration and refractoriness | Amiodarone, Sotalol, Dofetilide, Ibutilide, Dronedarone |
| IV | L-type Ca²⁺ channels | Slow AV node conduction and automaticity | Verapamil, Diltiazem |
Note: Amiodarone has Class I, II, III, and IV properties simultaneously.
Class I: Sodium Channel Blockers
Na⁺ channel blockers bind to channels in the open or inactivated state (use-dependent/frequency-dependent block). Recovery from block during diastole determines the extent of steady-state block - drugs with slow recovery (Class IC) cause more block at faster rates.
Class IA
Quinidine
- Broadest Class IA agent; also blocks K⁺ channels (prolongs QT), α-adrenergic receptors, and has anticholinergic properties
- Uses: AF maintenance, ventricular arrhythmias
- Toxicity: Cinchonism (tinnitus, headache), GI upset (diarrhea), torsades de pointes (due to QT prolongation), vagolytic effects can increase ventricular rate in AF if used without an AV nodal agent
Procainamide
- Similar to quinidine; active metabolite N-acetylprocainamide (NAPA) has additional Class III effects
- Uses: Acute VT, WPW with AF (preferred IV agent in some guidelines)
- Toxicity: Drug-induced lupus erythematosus (slow acetylators at risk), agranulocytosis; chronic use avoided
Disopyramide
- Strongly anticholinergic (urinary retention, dry mouth, glaucoma risk)
- Strong negative inotrope - contraindicated in heart failure
- Uses: Vagally-mediated AF, hypertrophic obstructive cardiomyopathy
Class IB
Lidocaine
- IV only (extensive first-pass metabolism)
- Binds preferentially to depolarized (ischemic) tissue - excellent for ventricular arrhythmias post-MI/reperfusion
- Minimal effect on normal tissue; does not affect atrial arrhythmias significantly
- Toxicity: CNS (perioral numbness, tremor, seizures at toxic levels)
Mexiletine
- Oral analogue of lidocaine
- Uses: Chronic ventricular arrhythmia suppression, often combined with amiodarone
- Notable use: Long QT syndrome type 3 (blocks the pathological late Na⁺ current)
- Toxicity: Tremor, nausea
Class IC
Flecainide
- Potent Na⁺ channel blocker with slow recovery - markedly slows conduction
- Uses: AF/flutter in structurally normal hearts; "pill-in-the-pocket" for paroxysmal AF
- CAST Trial Warning: Significantly increased mortality in patients with structural heart disease (post-MI) - contraindicated in ischemic heart disease or LV dysfunction
- Toxicity: Pro-arrhythmia (can convert AF to atrial flutter with 1:1 AV conduction if given without AV nodal blockade)
Propafenone
- IC agent with mild β-blocking properties
- Similar indications and contraindications to flecainide
- Metabolized by CYP2D6 (variable effects in poor metabolizers)
Class II: Beta-Blockers
Mechanism: Block β₁-adrenergic receptors → reduce sinus automaticity (decrease phase 4 slope) and slow AV node conduction.
Key agents in arrhythmia:
- Metoprolol, Atenolol - oral, cardioselective; rate control in AF/flutter, prevention of SVT
- Esmolol - ultra-short-acting IV (t½ ~9 min); ideal for acute rate control intraoperatively or in emergency settings
- Propranolol - non-selective; also used in long QT syndrome, thyrotoxic arrhythmias, CPVT
Beta-blockers are the cornerstone of rate control in AF and are antiarrhythmic in the post-MI setting, reducing sudden cardiac death risk.
Class III: Potassium Channel Blockers
These drugs prolong the action potential duration (APD) and refractoriness by blocking outward K⁺ currents. Prolonged APD = prolonged QT = risk of torsades de pointes.
Amiodarone - the most widely used antiarrhythmic
- Properties across all 4 classes (I, II, III, IV)
- Extremely long half-life (40-55 days); large volume of distribution
- Most effective AAD for maintaining sinus rhythm in AF; effective for VT/VF
- Multiorgan toxicity with long-term use:
- Pulmonary toxicity (fibrosis/pneumonitis) - most serious
- Thyroid dysfunction (hypo- or hyperthyroidism - contains 37% iodine)
- Hepatotoxicity
- Corneal microdeposits (nearly universal, usually asymptomatic)
- Photosensitivity (blue-grey skin discoloration)
- Peripheral neuropathy
- Drug interactions: Inhibits CYP3A4, CYP2C9, and P-glycoprotein → increases warfarin, digoxin, flecainide, procainamide levels significantly
Sotalol
- Class III + significant β-blocking (Class II) properties
- Uses: AF maintenance, ventricular arrhythmias
- Risk of torsades de pointes (especially with bradycardia, hypokalemia, renal failure)
- Must be initiated in-hospital with QT monitoring
Dofetilide
- "Pure" IKr blocker - selective Class III
- Uses: AF/flutter cardioversion and maintenance
- Significant torsades risk; requires 3-day in-hospital initiation with renal dose adjustment
- Eliminated renally - contraindicated in severe renal impairment
Ibutilide (IV only)
- Rapid-acting Class III agent for acute cardioversion of AF/flutter
- Effective in ~50-70% of flutter cases
- Requires cardiac monitoring for 4 hours post-dose (torsades risk)
Dronedarone
- Structural analogue of amiodarone without iodine moieties - less thyroid/pulmonary toxicity
- Effects across all 4 classes (milder than amiodarone)
- Uses: AF rate/rhythm control in patients with preserved EF
- Contraindicated in decompensated heart failure and permanent AF (increased mortality shown in ANDROMEDA and PALLAS trials)
Class IV: Calcium Channel Blockers
Only verapamil and diltiazem are clinically relevant for arrhythmias (dihydropyridines such as nifedipine act primarily on vascular smooth muscle).
- Block L-type Ca²⁺ channels in nodal tissue (SA, AV)
- Rate control in AF/flutter (acute and chronic)
- Terminate AVNRT and AVRT (reentry involving AV node)
- Contraindicated in WPW - blocking the AV node may force conduction through the accessory pathway at dangerous rates, potentially precipitating VF
- Verapamil is contraindicated in VT - can cause hemodynamic collapse (famous clinical pitfall of misidentifying VT as SVT)
Other Important Agents
Adenosine
- Endogenous nucleoside; activates K⁺ channels and inhibits adenylyl cyclase in AV node → transient complete AV block (seconds)
- Drug of choice for acute termination of AVNRT and AVRT (diagnostic and therapeutic)
- Half-life: ~10 seconds - administer as rapid IV bolus
- Contraindicated in cardiac transplant recipients (denervated heart is hypersensitive), severe asthma
- Common side effects: Flushing, dyspnea, chest discomfort (transient)
Digoxin
- Inhibits Na⁺/K⁺-ATPase → indirect vagomimetic effect → slows AV node conduction
- Uses: Rate control in AF with heart failure (where beta-blockers/CCBs may be poorly tolerated)
- Narrow therapeutic index; toxicity manifests as bradyarrhythmias, AV block, or paradoxically ventricular arrhythmias
- Contraindicated in WPW (same reason as CCBs)
Magnesium (IV)
- Treatment of torsades de pointes (even when Mg levels are normal)
- Adjunct in digoxin toxicity
Ranolazine
- Inhibits late Na⁺ current (Class IB-like) and IKr
- Primary indication: Chronic angina
- Notable antiarrhythmic use: AF in ischemic heart disease, adjunct in ventricular arrhythmias
Mechanistic Approach to Specific Arrhythmias
| Arrhythmia | Acute Therapy | Chronic Therapy |
|---|---|---|
| AF | Rate control (CCB, β-blocker, digoxin); DC cardioversion; IV ibutilide | Rate control (β-blocker, CCB); rhythm control (amiodarone, flecainide, propafenone, sotalol, dofetilide); anticoagulation |
| Atrial flutter | Same as AF; highly responsive to DC cardioversion | Catheter ablation preferred; same drugs as AF |
| AVNRT/AVRT (PSVT) | Vagal maneuvers → adenosine → IV verapamil/diltiazem | β-blockers, CCBs; catheter ablation (curative) |
| WPW with AF | IV procainamide or ibutilide | Ablation of accessory pathway |
| Stable VT | IV amiodarone, IV lidocaine, procainamide | Amiodarone, sotalol, mexiletine; ICD |
| VF/pulseless VT | DC defibrillation; IV amiodarone (300 mg); epinephrine | ICD; amiodarone |
| Torsades de pointes | IV magnesium; correct electrolytes; pacing; stop offending drug | Identify/treat cause; ICD if congenital LQTS |
| Digoxin toxicity arrhythmias | Digibind (Fab fragments); avoid cardioversion; correct K⁺ | Stop digoxin |
Drug Selection Algorithm for AF (Rhythm Control)
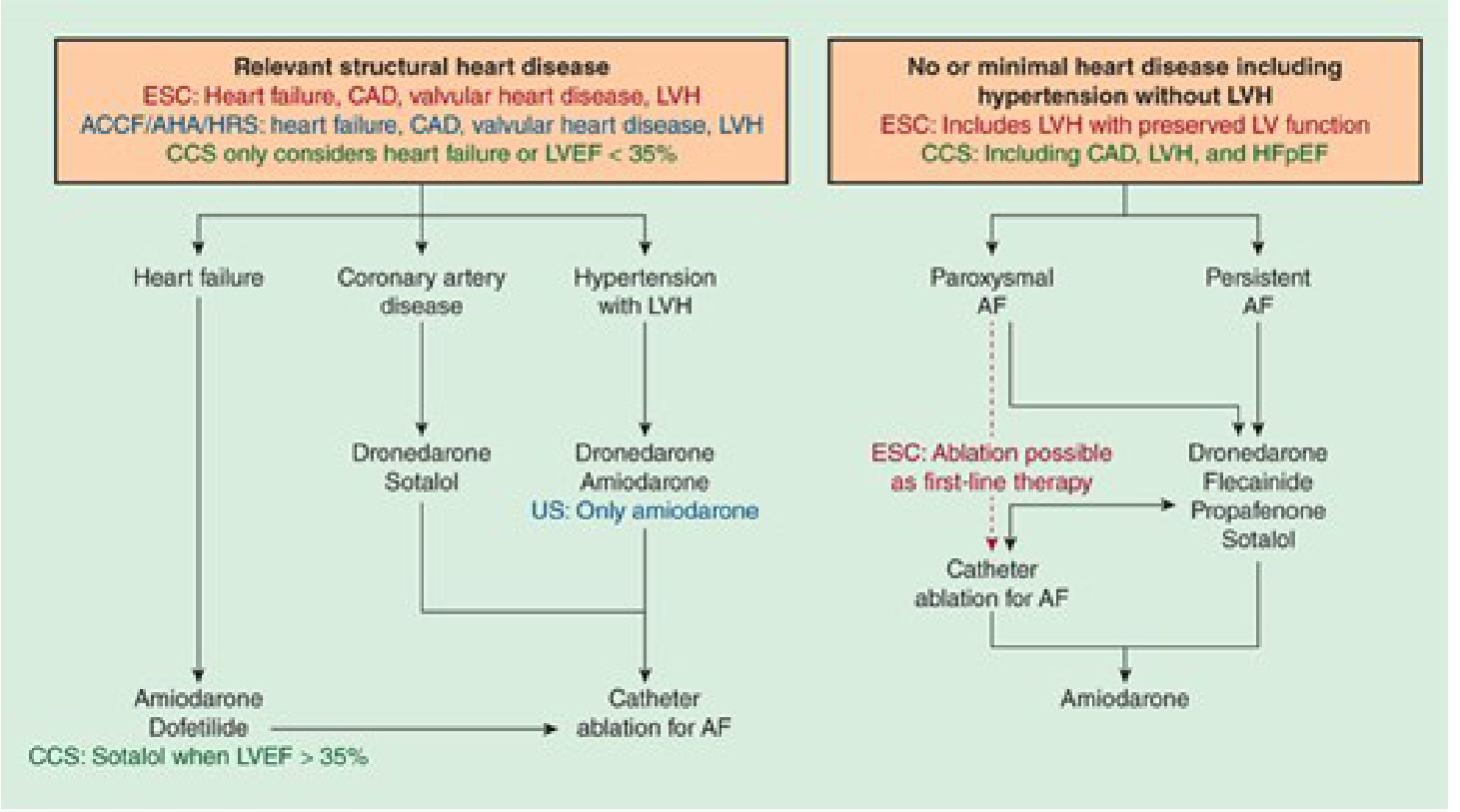
Drug selection for AF rhythm control depends primarily on the presence and type of structural heart disease - Katzung's Basic and Clinical Pharmacology, 16th Ed.
Key Contraindications Summary
| Condition | Drugs to Avoid |
|---|---|
| Heart failure (reduced EF) | Disopyramide, flecainide, dronedarone |
| Post-MI / ischemic heart disease | Flecainide, propafenone (Class IC) |
| WPW syndrome | Digoxin, verapamil, diltiazem |
| Prolonged QT | Quinidine, procainamide, sotalol, dofetilide, ibutilide, amiodarone |
| Severe renal failure | Dofetilide, sotalol (dose-adjust), procainamide |
| Asthma/COPD | β-blockers, propafenone |
| Lung disease | Amiodarone (relative) |
| Bradycardia/AV node disease | Digoxin, verapamil, diltiazem, β-blockers, amiodarone |
Proarrhythmia: A Critical Concept
All AADs can cause arrhythmias. The most clinically significant proarrhythmic mechanisms:
- QT prolongation → Torsades de pointes: Class IA (quinidine, procainamide), Class III agents - risk amplified by hypokalemia, hypomagnesemia, bradycardia, female sex, and drug interactions
- Flecainide/propafenone: Can convert AF to organized atrial flutter with 1:1 conduction (extreme tachycardia) - always co-prescribe an AV nodal agent
- Proarrhythmia in structural heart disease: The CAST trial established that flecainide/encainide increased sudden death in post-MI patients with asymptomatic PVCs
- Amiodarone: Despite QT prolongation, torsades is relatively uncommon - possibly due to its multiple channel-blocking effects providing balance
Clinical Principles of AAD Use
- Identify and remove precipitating factors - electrolyte abnormalities (K⁺, Mg²⁺), ischemia, thyroid disease, hypoxia
- Establish the arrhythmia diagnosis precisely before treating - misidentifying VT as SVT can be fatal
- Match drug to mechanism - e.g., AV nodal agents are not useful for AF termination, only rate control
- Use non-pharmacologic therapy when appropriate - catheter ablation is now first-line for many arrhythmias (AVNRT, atrial flutter, WPW, paroxysmal AF)
- Monitor for toxicity - plasma levels (digoxin, procainamide), QT intervals (all Class I/III agents), organ function (amiodarone monitoring: TFTs, LFTs, PFTs, ophthalmic exam)
- Consider the "moving target" - cardiac electrophysiology changes with ischemia, rate, and autonomic tone, altering drug effects unpredictably
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Ed. | Harrison's Principles of Internal Medicine, 22nd Ed. (2025) | Katzung's Basic and Clinical Pharmacology, 16th Ed.
Recent evidence note: A 2024 meta-analysis (PMID 38727662) comparing rhythm vs. rate control strategies for AF found no significant mortality difference between strategies, reinforcing that symptom burden and patient preference guide the choice. A 2026 analysis (PMID 40803485) comparing AADs vs. catheter ablation found ablation superior to drugs for maintaining sinus rhythm in AF, consistent with the growing shift toward earlier ablation.
What is meant by sprue with sartans
Reading File
Finding Sources
Searching PubMed
"olmesartan" AND "sprue" AND "enteropathy"
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"olmesartan enteropathy" AND "mechanism"
I now have comprehensive information from multiple authoritative GI textbooks to give a detailed, well-sourced answer.
Sprue with Sartans (Olmesartan-Associated Sprue-like Enteropathy)
What It Is
"Sprue with sartans" refers to a drug-induced sprue-like enteropathy caused by angiotensin II receptor blockers (ARBs, colloquially called "sartans"). It is most strongly associated with olmesartan medoxomil and was first described in 2012 by Rubio-Tapia et al. at the Mayo Clinic. The condition clinically and histologically mimics celiac disease (gluten-sensitive enteropathy) but is caused by the drug itself, not gluten.
The hallmark features are:
- Severe chronic diarrhea
- Weight loss and malabsorption
- Villous atrophy on small bowel biopsy
- Negative celiac serology (anti-tTG, anti-endomysial antibodies)
- Resolution with drug withdrawal
Epidemiology and Which Sartans Are Implicated
Olmesartan is by far the most commonly reported culprit, prompting an FDA drug safety communication in July 2013. However, case reports and pharmacovigilance data from Germany and Italy suggest other ARBs (valsartan, irbesartan, candesartan, telmisartan) can also cause the syndrome, though far less frequently. Large US and French cohort studies have not confirmed a significant signal with non-olmesartan ARBs, so olmesartan appears uniquely potent in this regard.
Clinical Features
Based on a systematic review of 54 patients (Brenner & Rector's The Kidney):
| Feature | Frequency |
|---|---|
| Diarrhea | 95% |
| Weight loss | 89% |
| Fatigue, nausea, vomiting, abdominal pain | Less common |
| Normochromic normocytic anemia | ~45% |
| Hypoalbuminemia | ~39% |
| HLA-DQ2 or HLA-DQ8 positivity | >70% |
A key distinguishing feature is the prolonged latency: diarrhea onset typically lags the start of olmesartan therapy by months to years (reported range: 6 months to 7 years). This makes the drug-symptom connection easy to miss clinically.
Pathological Findings
On small bowel (duodenal) biopsy:
- Villous atrophy (varying degrees - partial to total)
- Increased intraepithelial lymphocytes
- Crypt hyperplasia
Additional findings often present simultaneously:
- Microscopic colitis (lymphocytic or collagenous colitis)
- Lymphocytic gastritis
This multi-segment GI involvement is somewhat characteristic and can be a clue to the drug etiology. The histology is indistinguishable from celiac disease, which is why serology is critical in the workup.
Mechanism (Proposed)
The exact mechanism is not fully established. The leading hypothesis is immune-mediated:
- Olmesartan appears to interfere with TGF-β signaling in the gut. TGF-β normally maintains intestinal immune tolerance; its blockade may unleash T-cell-mediated mucosal attack.
- Angiotensin II itself has pro-inflammatory roles in the gut mucosa, but paradoxically, ARBs that block it may disrupt the regulatory balance.
- The high prevalence of HLA-DQ2/DQ8 in affected patients suggests a genetic predisposition similar to celiac disease - these individuals may have an underlying tendency toward T-cell-mediated gut inflammation that olmesartan triggers.
- Unlike celiac disease, there is no role for gluten - the enteropathy does not respond to a gluten-free diet.
Diagnosis
The condition should be suspected in any patient on an ARB (especially olmesartan) presenting with:
- Chronic, severe diarrhea with weight loss
- Biopsy showing villous atrophy
- Negative celiac antibodies (seronegative villus atrophy)
- No response to a gluten-free diet
The differential diagnosis of seronegative villous atrophy includes:
- Celiac disease with seronegative presentation
- Common variable immunodeficiency (CVID)
- Autoimmune enteropathy
- GI infections (Giardia, Cryptosporidium)
- Tropical sprue
- Collagenous sprue
- Olmesartan/ARB enteropathy - always check the drug list
Treatment
Withdraw the offending ARB. This is both diagnostic and curative.
- Clinical improvement (cessation of diarrhea, weight gain) typically occurs within weeks to months of stopping the drug
- Histological recovery (villous regeneration) follows clinical improvement
- Rechallenge with the drug leads to relapse, confirming the diagnosis
- No specific pharmacological treatment is needed beyond drug withdrawal; supportive nutritional replacement may be needed in severe cases
Importantly, a gluten-free diet does not help - this differentiates it from celiac disease.
Clinical Importance
This entity is clinically significant for several reasons:
-
Missed diagnosis: Because olmesartan is commonly prescribed for hypertension (typically in older adults), and the latency is long, clinicians often investigate for celiac disease, IBD, or malignancy without recognizing the drug as the cause.
-
Hospitalization and morbidity: Cases have required IV nutrition and hospitalization due to severe malabsorption - simply stopping a blood pressure pill would have been curative.
-
Misdiagnosis as refractory celiac disease: Patients placed on a gluten-free diet for presumed celiac disease naturally fail to improve if olmesartan is the true cause. Olmesartan should be in the differential for all cases of non-responsive celiac disease.
-
Regulatory action: The FDA updated the olmesartan label in 2013 to warn of this complication.
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Yamada's Textbook of Gastroenterology, 7th Ed. | Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.