Microteaching on hallucinogens in mental health nursing 6th semester
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive textbook data to deliver a thorough microteaching lesson. Let me compile it all into a structured format.
Microteaching Lesson Plan: Hallucinogens in Mental Health Nursing
6th Semester | Subject: Mental Health Nursing | Duration: 10-15 minutes
LESSON PLAN STRUCTURE
| Element | Detail |
|---|---|
| Topic | Hallucinogens - Classification, Mechanism, Effects, and Nursing Management |
| Class | B.Sc. Nursing, 6th Semester |
| Duration | 10-15 minutes (microteaching) |
| AV Aids | Blackboard/whiteboard, diagrams, flashcards |
| Method | Lecture with discussion |
LEARNING OBJECTIVES
By the end of this microteaching session, students will be able to:
- Define hallucinogens and classify them with examples
- Explain the mechanism of action of hallucinogens
- Describe the signs and symptoms of hallucinogen intoxication ("bad trip")
- Identify specific drugs (LSD, psilocybin, mescaline, PCP, ketamine) and their effects
- List nursing interventions for a client under hallucinogen intoxication
INTRODUCTION (2 minutes)
Start with a trigger question:
"Have you ever heard of someone 'tripping' on mushrooms or LSD? What did they experience?"
Definition: Hallucinogens are a group of psychoactive substances that alter perception, thought, and mood - primarily causing illusions, sensory distortions, and altered states of consciousness, while maintaining a clear level of wakefulness.
Key distinction: Hallucinogens more commonly cause illusions (distortions of real sensory input) rather than true hallucinations (perceptions without any stimulus).
- Stahl's Essential Psychopharmacology, p. 584
PART 1 - CLASSIFICATION (3 minutes)
Three Major Classes (all act as 5HT2A receptor agonists):
| Class | Example Drugs | Source |
|---|---|---|
| Tryptamines | Psilocybin ("magic mushrooms"), DMT | Natural/synthetic |
| Ergolines | LSD (lysergic acid diethylamide) | Semi-synthetic from ergot fungus |
| Phenethylamines | Mescaline (from peyote cactus) | Natural |
Additional hallucinogens (dissociatives):
- PCP (phencyclidine) - acts at NMDA receptors
- Ketamine - dissociative anesthetic, NMDA antagonist
Empathogens (related category):
- MDMA (ecstasy) - acts on serotonin transporters (SERT)
- Kaplan and Sadock's Synopsis of Psychiatry, p. 991; Stahl's Essential Psychopharmacology, p. 583
PART 2 - MECHANISM OF ACTION (2 minutes)
Primary Mechanism: 5HT2A Receptor Agonism
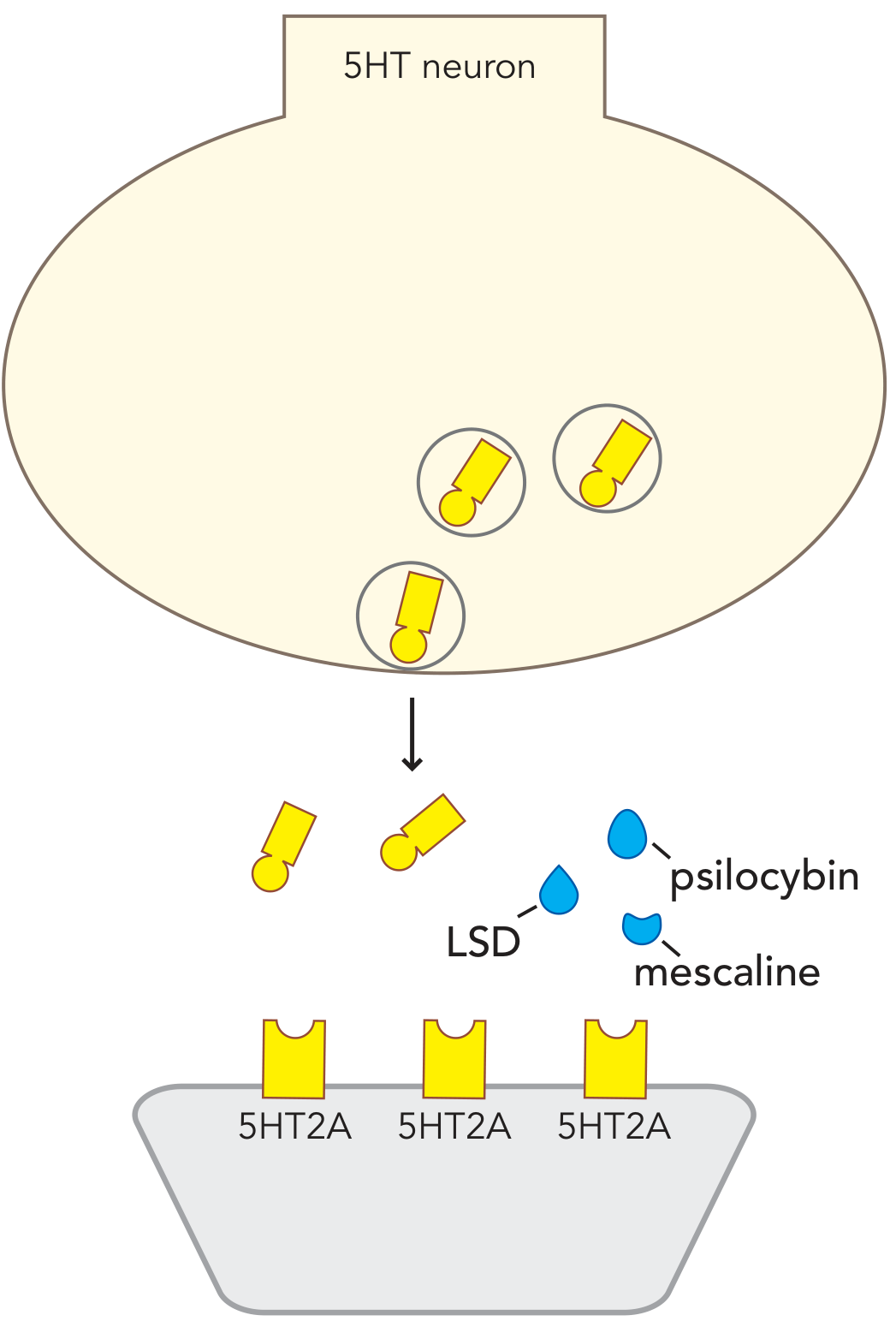
Figure: Hallucinogens (psilocybin/psilocin, LSD, mescaline) act as agonists at postsynaptic 5HT2A receptors, mimicking serotonin's action and producing psychedelic effects.
Key pharmacological points:
- LSD, psilocybin, and mescaline all act predominantly as 5HT2A agonists
- They also bind 5HT2B, 5HT7, 5HT1D, and other serotonin receptor subtypes
- 5HT2A antagonists (not D2 blockers) can reverse hallucinogen effects - confirming the primary mechanism
- PCP/Ketamine act differently - they block NMDA receptors (dissociative mechanism)
Relative potency comparison:
100 mcg LSD = 10-15 mg psilocybin = 300-400 mg mescaline
- Kaplan and Sadock's Synopsis of Psychiatry, p. 991
PART 3 - SIGNS & SYMPTOMS OF INTOXICATION (3 minutes)
The "Trip"
The hallucinogenic state (called a "trip") produces perceptual, psychological, and physiological effects:
Perceptual/Psychological:
- Visual illusions, visual "trails" (smearing of moving images)
- Macropsia and micropsia (objects appear larger/smaller)
- Synesthesia: colors are "heard," sounds are "seen"
- Depersonalization and derealization
- Intensification of sound
- Emotional and mood lability
- Subjective slowing of time
- Euphoria, peaceful floating, bodily warmth
- Paranoia, delusions (with escalating doses)
- Auditory and visual hallucinations
Physiological (LSD - Table 4-40, Kaplan & Sadock):
| Common | Occasional |
|---|---|
| Dilated pupils | Tachycardia |
| Increased deep tendon reflexes | Hypertension |
| Muscle tension | Nausea, decreased appetite |
| Mild motor incoordination | Sweating, blurred vision |
| Ataxia | Salivation |
LSD time course:
- Onset: within 1 hour
- Peak: 2-4 hours
- Duration: 8-12 hours
"Bad Trip" - when intoxication causes acute panic, intense anxiety, fear of losing one's mind. Can escalate to:
- Delirium - disorientation, agitation
- Frank psychosis - delusions, paranoia (uncommon)
- Stahl's Essential Psychopharmacology, p. 584; Kaplan and Sadock's Synopsis of Psychiatry, p. 992
PART 4 - SPECIAL PHENOMENA (1 minute)
Tolerance
- Develops rapidly, sometimes after a single dose
- Due to desensitization (downregulation) of 5HT2A receptors
- Cross-tolerance exists among LSD, mescaline, and psilocybin
- 4-6 days free of LSD needed to lose tolerance
Flashbacks (Hallucinogen Persisting Perception Disorder - HPPD)
- Spontaneous recurrence of intoxication symptoms without recent drug use
- Lasts seconds to several hours
- Occurs days to months after last use
- Most commonly reported with LSD
- Mechanism unknown - possibly related to long-lasting serotonin system adaptation or emotional conditioning via the amygdala (similar to PTSD re-experiencing)
- Stahl's Essential Psychopharmacology, p. 584
PART 5 - NURSING MANAGEMENT (3 minutes)
Assessment Priorities
- Assess level of consciousness - are they fully awake and oriented?
- Monitor vital signs: pulse, BP, temperature (LSD is sympathomimetic - risk of hypertension, hyperthermia)
- Assess for "bad trip" - panic, extreme anxiety, paranoia
- Assess for delirium or psychosis (escalated intoxication)
- Check for self-harm risk - impaired judgment can lead to accidents (e.g., running into traffic)
Nursing Interventions
During acute intoxication ("talking down" technique):
- Maintain a calm, quiet, low-stimulation environment - reduce sensory input
- Use a calm, reassuring tone - "Talk down" the patient
- Stay with the patient (do not leave alone)
- Reassure that the experience is drug-induced and will pass
- Do NOT argue with or challenge the patient's perceptions
- Use simple, clear language
- Allow the patient to verbalize feelings
Physical safety:
- Ensure environmental safety - remove sharp objects
- Protect from accidental injury due to impaired judgment
- Monitor airway if sedation develops (especially with PCP/ketamine)
- IV access if needed for emergency medications
For PCP intoxication (more dangerous):
- Patients may be uncommunicative, aggressive, or combative
- Physical restraint may be necessary
- Monitor for cardiovascular effects and hyperthermia
- Effects can persist 1-2 days; PCP can remain in blood/urine for >1 week
For flashbacks:
- Reassurance that the experience is not true psychosis
- Short-term benzodiazepines (prescribed) for acute anxiety
- Avoid antipsychotics that worsen serotonergic imbalance
- Psychoeducation and follow-up
Pharmacological support (as prescribed):
- Benzodiazepines (e.g., diazepam, lorazepam) - for anxiety, agitation
- Antipsychotics - cautiously for psychotic features (note: D2 blockers do NOT reverse hallucinations; 5HT2A antagonists do)
- Supportive care for hyperthermia, hypertension
PART 6 - THERAPEUTIC USES (brief mention)
Emerging area: Hallucinogens (especially psilocybin) and empathogens (MDMA) are being studied for therapeutic use in:
- PTSD
- Treatment-resistant depression
- End-of-life anxiety
Ketamine (as esketamine nasal spray - Spravato) is FDA-approved for treatment-resistant depression.
- Stahl's Essential Psychopharmacology, p. 584; Kaplan and Sadock's Synopsis of Psychiatry, p. 654
SUMMARY TABLE (for blackboard)
| Drug | Class | Mechanism | Duration | Key Feature |
|---|---|---|---|---|
| LSD | Ergoline | 5HT2A agonist | 8-12 hr | Flashbacks, most potent |
| Psilocybin | Tryptamine | 5HT2A agonist | 4-6 hr | "Magic mushrooms," prodrug |
| Mescaline | Phenethylamine | 5HT2A agonist | 6-12 hr | Peyote cactus, more nausea |
| PCP | Dissociative | NMDA antagonist | 3-6 hr | Aggressive, combative |
| Ketamine | Dissociative | NMDA antagonist | 1-2 hr | Medical use, "K-hole" |
| MDMA | Empathogen | SERT releaser | 3-5 hr | Empathy, serotonin syndrome risk |
EVALUATION QUESTIONS
- What is the primary mechanism of action of classical hallucinogens?
- Differentiate between a "trip" and a "bad trip"
- What is HPPD? Which drug most commonly causes flashbacks?
- List three nursing interventions during hallucinogen intoxication
- Why can't D2 antagonists reverse hallucinogen effects?
KEY REFERENCES (for students)
- Stahl's Essential Psychopharmacology: Neuroscientific Basis and Practical Applications (Stahl's Essential Psychopharmacology, Ch. 13)
- Kaplan and Sadock's Synopsis of Psychiatry (Table 4-40, pp. 991-994)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (Table 11.6-1, Serotonergic Hallucinogens)
MICROTEACHING TIPS
- Set induction: Use a brief case scenario or newspaper headline about psilocybin clinical trials to grab attention
- Teach the mechanism with the diagram (5HT2A agonism figure above) on the board - students remember this
- Role-play "talking down" technique with a student for 2 minutes - this is highly effective for nursing skills
- Mnemonics: For LSD physiological effects - "DIMMS": Dilated pupils, Increased reflexes, Muscle tension, Motor incoordination, Sweating/Sympathomimetic signs
This is a shared conversation. Sign in to Orris to start your own chat.