Kinematics & kinetics of Gait - MPT level 15 marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent! I now have all the content I need for a comprehensive MPT-level 15-mark answer. Let me compile it.
Kinematics and Kinetics of Gait
(MPT Level - 15 Marks)
Introduction
Human gait is the pattern of movement of the limbs during locomotion. It is studied under two broad categories:
- Kinematics - describes the geometry of motion (joint angles, displacement, velocity, acceleration) without reference to the forces that cause it.
- Kinetics - describes the forces acting during motion (ground reaction forces, joint moments, joint powers, muscle forces).
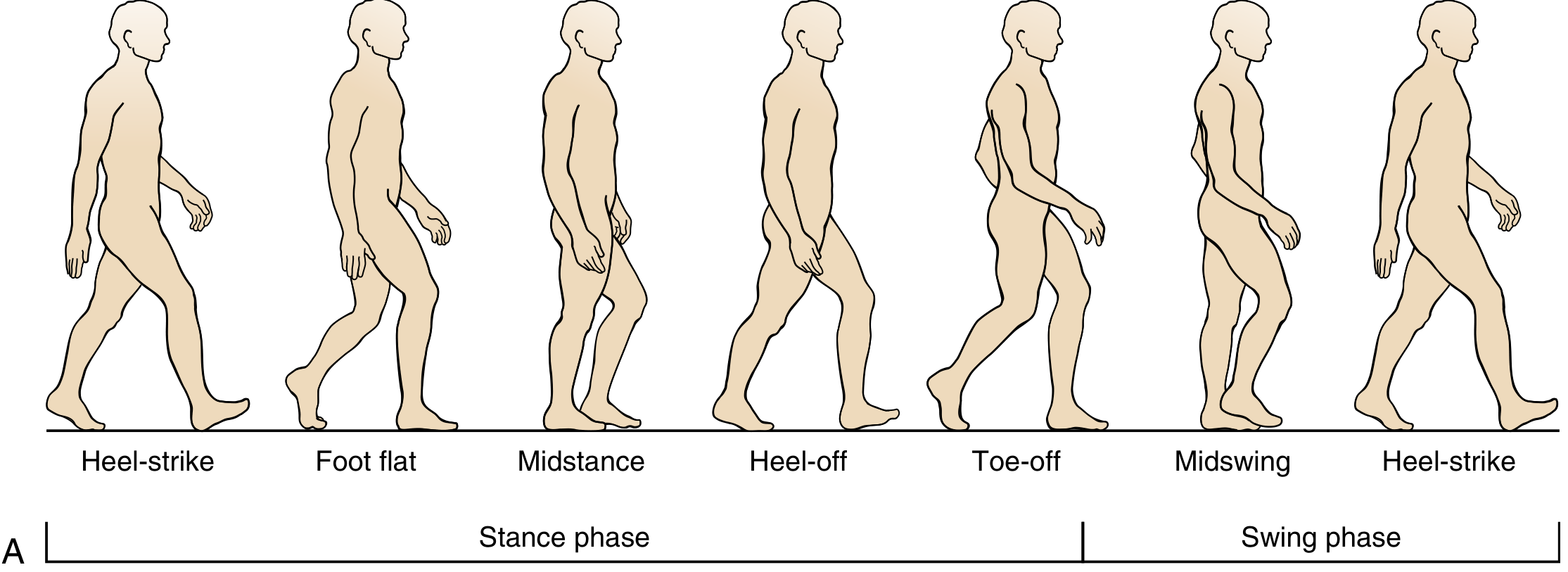
I. THE GAIT CYCLE
One complete gait cycle = heel strike to next heel strike of the same limb = one stride.
The normal phases of gait (Miller's Review of Orthopaedics, 9th Ed.)
Temporal Parameters
| Parameter | Value |
|---|---|
| Stride length | Heel strike to heel strike, same limb |
| Step length | Heel strike to heel strike, opposite limbs |
| Cadence | Steps per minute (~100-120 steps/min) |
| Walking speed | Stride length x Cadence/2 |
| Stance phase | 60% of gait cycle |
| Swing phase | 40% of gait cycle |
| Double limb support | Two periods, each ~10-12% (velocity-dependent) |
Walking differs from running in that one foot is always in contact with the ground during walking, while running has a float phase (no foot contact).
II. PHASES OF THE GAIT CYCLE
A. Stance Phase (60%)
Divided into five sub-phases:
- Initial Contact (IC) / Heel Strike - the instant the reference foot contacts the ground
- Loading Response (LR) - from IC to initial swing of the contralateral foot (double limb support)
- Midstance (MSt) - from contralateral toe-off to when the body's center of gravity (COG) is directly over the supporting forefoot
- Terminal Stance (TSt) - begins with heel rise, continues until IC of the contralateral foot
- Preswing (PSw) - from IC of the contralateral limb to when the stance foot lifts off (second double limb support period)
B. Swing Phase (40%)
Divided into three sub-phases:
- Initial Swing (ISw) - reference foot leaves ground to when the swinging foot is opposite the stance foot
- Midswing (MSw) - ends when tibia is perpendicular/vertical to the ground
- Terminal Swing (TSw) - tibia vertical to when the foot makes IC again
III. KINEMATICS OF GAIT
Kinematics describes joint angular displacements in the sagittal, frontal, and transverse planes throughout the gait cycle.
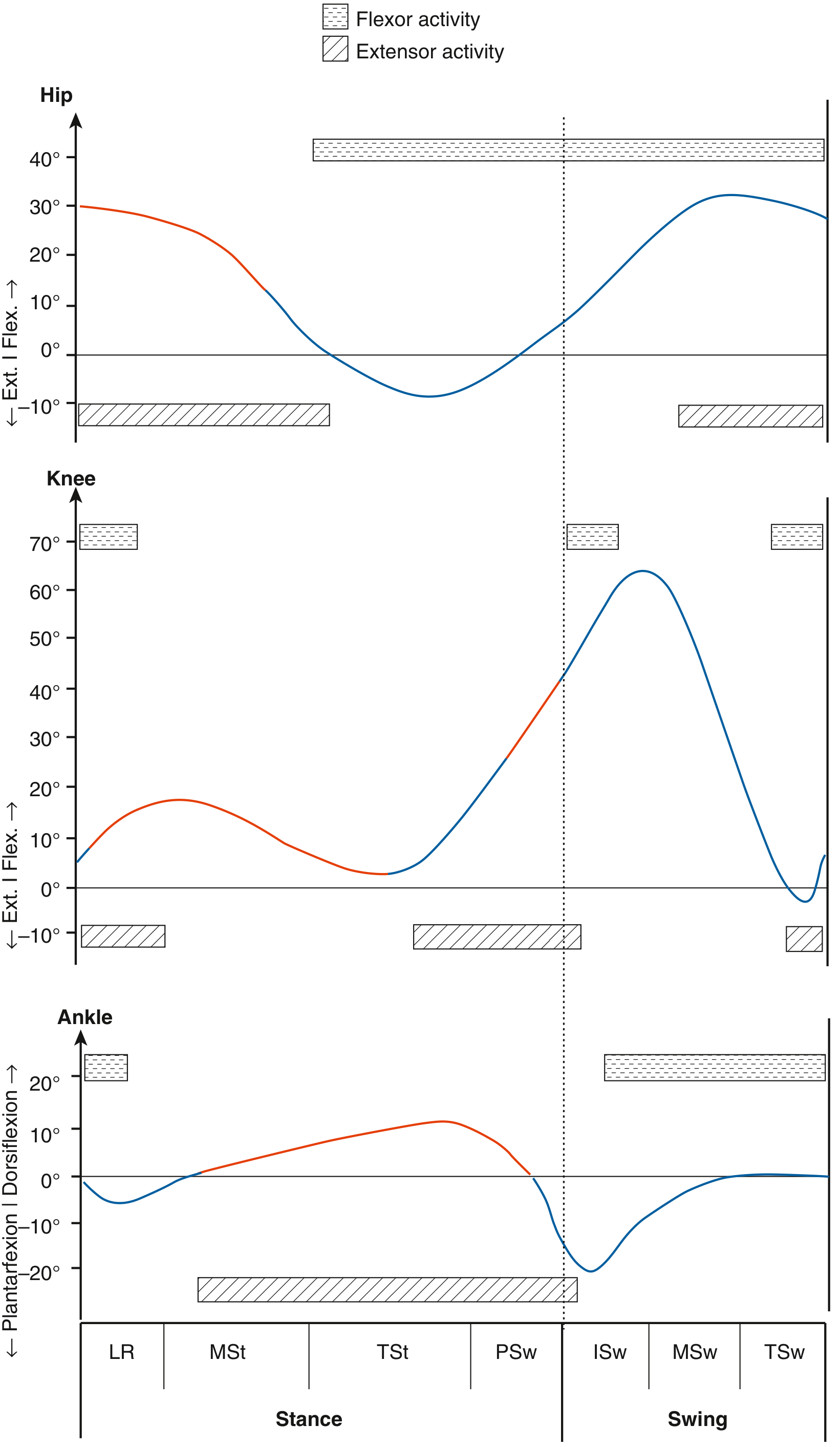
Kinematics and kinetics of the hip, knee, and ankle through the gait cycle. Red curves = phases when GRF is anterior to hip, posterior to knee, and anterior to ankle in stance. (Miller's Review of Orthopaedics, 9th Ed.)
A. Hip Kinematics
| Phase | Motion |
|---|---|
| IC | ~30° flexion |
| LR to MSt | Progressive extension (hip moves from ~30° flex to neutral) |
| TSt | ~10° hyperextension |
| PSw | Rapid flexion begins |
| ISw to TSw | Hip flexes to ~30° for limb advancement |
- Hip flexors (iliopsoas) advance the limb in swing; hip extensors decelerate the limb in terminal swing before IC.
B. Knee Kinematics
| Phase | Motion |
|---|---|
| IC | ~5° flexion |
| LR | Flexes to ~15-18° (shock absorption) |
| MSt | Extends towards full extension |
| TSt | Near full extension |
| PSw | Rapid flexion |
| ISw-MSw | Peak flexion ~60-65° (for foot clearance) |
| TSw | Extends to ~0-5° in preparation for IC |
- The double "wave" of knee flexion is a classic kinematic feature: a small flexion wave in loading response, and a large flexion wave in swing.
C. Ankle Kinematics
| Phase | Motion |
|---|---|
| IC | ~0° (neutral) or slight plantarflexion |
| LR | Plantarflexes ~5° (controlled by tibialis anterior eccentrically) |
| MSt | Progressively dorsiflexes to ~10° |
| TSt | Peak dorsiflexion ~10° |
| PSw | Rapid plantarflexion ~20° (push-off) |
| Swing | Returns to neutral/slight dorsiflexion (tibialis anterior concentrically) |
D. Pelvis & Trunk Kinematics
In the sagittal and frontal planes, the body's COG moves in a smooth sinusoidal curve:
- Vertical displacement - 5 cm amplitude (rises in midstance, falls at double support)
- Lateral displacement - 6 cm amplitude (shifts over the weight-bearing limb)
IV. DETERMINANTS OF GAIT (Saunders' 6 Determinants)
Six mechanisms work in concert to minimize COG excursion and maximize energy efficiency:
- Pelvic rotation - pelvis externally rotates ~4° each side during forward progression; reduces the drop of COG
- Pelvic list (tilt) - non-weight-bearing side drops 5°; reduces superior deviation of COG
- Knee flexion at loading - ~15° flexion in early stance; dampens impact, smooths COG trajectory
- Foot and ankle mechanism - subtalar joint pronation at LR for shock absorption; supination at TSt for rigid propulsion
- Knee motion - works with foot/ankle; flexion at IC, extension at MSt
- Lateral displacement control - shifts COG ~5 cm over the weight-bearing limb, narrowing base of support
V. KINETICS OF GAIT
Kinetics describes forces and moments produced during gait.
A. Ground Reaction Force (GRF)
The GRF is the force exerted by the ground on the foot - equal and opposite to the force the foot exerts on the ground (Newton's 3rd Law).
Magnitude:
- During walking: ~1.2-1.5 times body weight
- During running: ~3-4 times body weight (due to the impact after the float phase)
GRF Components:
- Vertical: double-peaked "M" shape in normal walking - first peak at loading (~1.2 BW), trough at midstance (~0.8 BW), second peak at push-off (~1.2 BW)
- Anterior-posterior: braking force (posterior) in early stance, propulsive force (anterior/forward) in late stance
- Mediolateral: lateral force in early stance, medial force in late stance
B. Joint Moments (Torques)
A joint moment is created when the GRF vector passes at a distance from the joint center. It represents the external demand placed on the joint, which must be met by an equal and opposite internal muscular response.
Key moments in stance:
| Joint | GRF Position | External Moment | Muscle Response |
|---|---|---|---|
| Hip (IC-MSt) | Posterior to hip | Hip flexion moment | Gluteus maximus (eccentric) |
| Hip (TSt-PSw) | Anterior to hip | Hip extension moment | Iliopsoas (concentric) |
| Knee (IC-LR) | Posterior to knee | Knee flexion moment | Quadriceps (eccentric) |
| Knee (MSt-TSt) | Anterior to knee | Knee extension moment | Hamstrings/gastrocnemius |
| Ankle (LR-TSt) | Anterior to ankle | Dorsiflexion moment | Gastrocnemius-soleus (eccentric) |
| Ankle (PSw) | Anterior to ankle | Dorsiflexion moment | Gastroc-soleus (concentric push-off) |
Hip abductor moment in single limb stance:
During single limb support (MSt), the GRF passes medial to the hip joint, creating an external hip adduction moment. The hip abductors (gluteus medius) must generate an equal and opposite internal abduction moment to keep the pelvis level. Failure produces Trendelenburg gait (contralateral pelvic drop). - Firestein & Kelley's Rheumatology, 2022
Knee adduction moment:
The GRF passes medial to the knee joint axis, creating an external knee adduction moment. This loads the medial compartment more than the lateral compartment, and is implicated in the development and progression of medial compartment knee OA.
C. Joint Power
Joint power = Joint moment x Joint angular velocity
- Positive power = energy generation (concentric muscle action)
- Negative power = energy absorption (eccentric muscle action)
Key power events:
- H1 - hip extension power generation (push-off assist, late stance)
- A2 - large ankle plantarflexor power generation at push-off (the main propulsive energy source in normal gait)
- K1 - knee absorption at loading response
- K3 - knee absorption in late stance
D. Inverse Dynamics
Joint forces and moments are calculated using inverse dynamics - applying Newton's 2nd Law to each body segment starting distally (from the foot, using measured GRF) and working proximally. This requires knowledge of:
- Segment masses and inertial properties
- 3D segment motion (from kinematic analysis)
- GRF (from force plates)
VI. MUSCLE ACTIONS DURING GAIT
Most muscle activity during gait is eccentric (muscle active while lengthening - controlling motion rather than producing it).
| Muscle | Type of Contraction | Phase | Function |
|---|---|---|---|
| Gluteus maximus | Eccentric | IC to MSt | Controls hip flexion rate; stabilizes pelvis |
| Gluteus medius | Eccentric | MSt | Controls pelvic tilt (Trendelenburg prevention) |
| Iliopsoas | Concentric | PSw-ISw | Powers hip flexion for limb advancement |
| Hip adductors | Eccentric | Late stance | Control lateral sway |
| Quadriceps | Eccentric | LR | Stabilizes knee against flexion at loading |
| Hamstrings | Eccentric | TSw | Decelerates knee extension before IC |
| Tibialis anterior | Eccentric at IC, Concentric in swing | Dual role | Slows plantarflexion at IC; dorsiflexes in swing for clearance (loss = foot drop/steppage gait) |
| Gastrocnemius-soleus | Eccentric in MSt, Concentric at PSw | MSt to PSw | Controls forward tibial progression; generates propulsive push-off power |
| Posterior tibialis | Active at TSt | Inverts hindfoot | Locks transverse tarsal joint; enables rigid lever for heel rise/toe-off |
- Miller's Review of Orthopaedics, 9th Ed.
VII. ENERGY EFFICIENCY OF GAIT
- The six determinants minimize COG excursion, reducing the mechanical work required.
- The COG follows a sinusoidal path; the body converts between kinetic and potential energy like an inverted pendulum in midstance.
- At push-off, stored elastic energy in the Achilles tendon and plantar fascia contributes to propulsion.
- Plantar fascia / windlass mechanism: As the MTP joints dorsiflex at toe-off, the plantar fascia tightens (windlass), accentuating the longitudinal arch and locking the transverse tarsal joint - converting the foot from a flexible shock absorber into a rigid propulsive lever arm.
VIII. GAIT ANALYSIS METHODS
Modern quantitative gait analysis combines:
- Kinematic data - high-speed motion capture cameras with retroreflective markers on skeletal landmarks; 3D joint angles presented as waveforms across the gait cycle
- Kinetic data - force platforms measuring GRF; inverse dynamics for joint moments and powers
- EMG - documents muscle activation patterns and detects out-of-phase firing
- Pedobarography - foot pressure distribution
- Oxygen consumption - measures metabolic cost of gait
Clinical application: preoperative planning (especially in cerebral palsy), treatment outcome assessment, and guiding physical therapy protocols. Studies show that adding gait analysis to clinical observation changes surgical recommendations in up to 52% of cases. - Campbell's Operative Orthopaedics, 15th Ed.
Summary Table: Kinematics vs. Kinetics
| Feature | Kinematics | Kinetics |
|---|---|---|
| Definition | Geometry of motion | Forces causing motion |
| Parameters | Joint angles, displacement, velocity | GRF, joint moments, powers, muscle forces |
| Tools used | Motion capture | Force plates, inverse dynamics |
| Key concept | Joint angular curves through gait cycle | GRF vector relationship to joint centers |
| Clinical relevance | Detecting range-of-motion deficits | Understanding loading patterns, OA risk |
References:
- Miller's Review of Orthopaedics, 9th Edition
- Campbell's Operative Orthopaedics, 15th Edition (2026)
- Firestein & Kelley's Textbook of Rheumatology, 2022
This is a shared conversation. Sign in to Orris to start your own chat.