Fever management
Reading File
Finding Sources
Searching PubMed
fever management treatment antipyretics
Finding Sources
Finding Sources
Finding Sources
Searching the Web
fever management clinical guidelines antipyretics 2024 2025
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of fever management drawn from authoritative medical textbooks and current guidelines.
Fever Management
1. Definition and Temperature Thresholds
Fever is an abnormal elevation of body temperature above the usual range of normal (36-38°C / 96.8-100.4°F), caused by a resetting of the hypothalamic thermostat. The following temperature ranges carry distinct clinical implications:
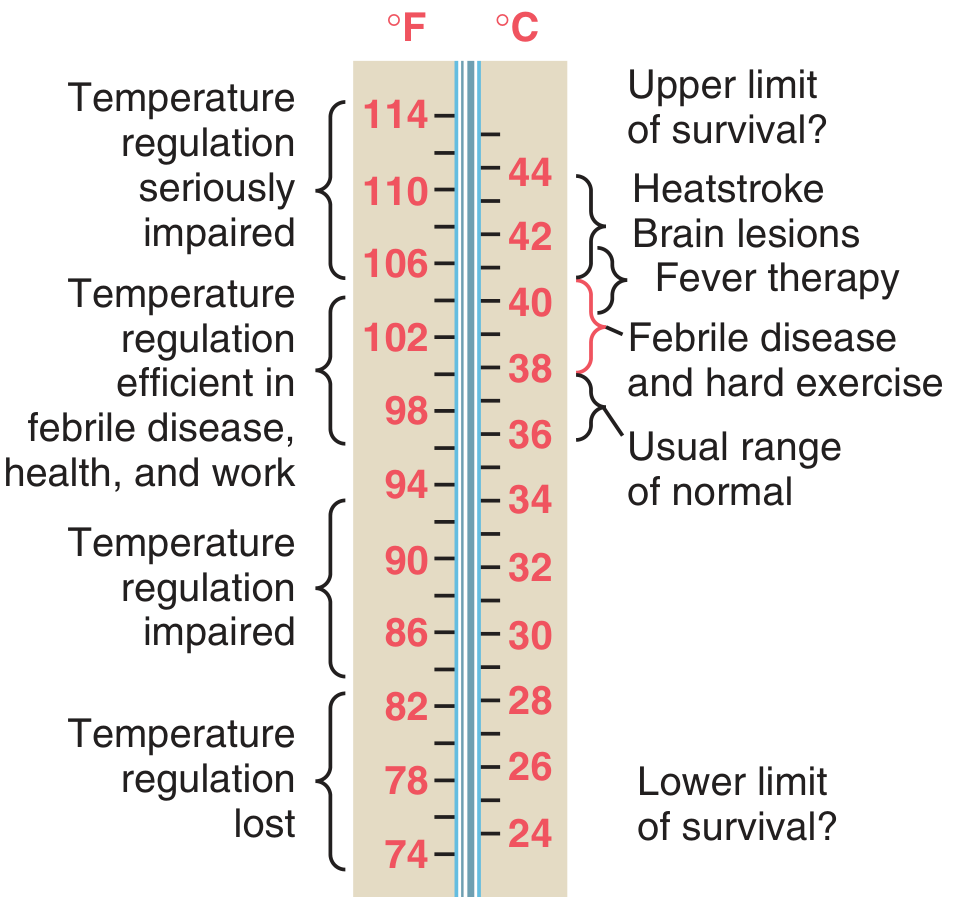
Key thresholds:
- Fever: > 38°C (100.4°F)
- High-grade fever: > 39.5°C
- Hyperpyrexia: > 41.5°C (106°F) - requires urgent treatment; associated with heatstroke and brain lesions
- Upper limit of survival: ~44°C (114°F)
2. Pathophysiology
The mechanism follows a well-defined sequence (Guyton and Hall, Costanzo Physiology):
- Trigger: Bacterial/viral products (especially LPS from gram-negative bacteria), tissue breakdown products, or inflammatory stimuli enter the circulation.
- Phagocyte activation: Macrophages, leukocytes, and NK cells phagocytize these products and release cytokines - primarily IL-1 (leukocyte pyrogen/endogenous pyrogen), as well as IL-6 and TNF.
- Hypothalamic set-point reset: IL-1 acts on the anterior hypothalamus to stimulate local prostaglandin E2 (PGE2) synthesis via COX-2 and mPGES-1, raising the thermoregulatory set point.
- Heat conservation/generation: The body perceives its current temperature as "too low" relative to the new set point - triggering vasoconstriction (chills) and shivering until the new set point is reached.
- Break of fever: When the stimulus is removed, the set point falls; the body then dissipates heat via vasodilation and sweating (the "defervescence" or "crisis" phase).
3. When to Treat Fever
General Principle (Harrison's Principles of Internal Medicine, 22E)
"Fever itself is not an illness; it is an ordinary response to a perturbation of normal host physiology."
Antipyretics do not delay resolution of common viral or bacterial infections, and there is no significant clinical evidence that fever facilitates recovery or acts as an immune adjuvant. However, clinical judgment guides whether to treat:
Treat fever when:
- Patient has significant discomfort (headache, myalgias, arthralgias)
- Pre-existing cardiac, pulmonary, or CNS impairment (fever increases O2 consumption by ~13% per 1°C above 37°C)
- Hyperpyrexia (>41°C) - direct tissue damage risk
- Children with a history of febrile seizures (treat aggressively)
- Patients with CNS disease or trauma - high temperature has direct detrimental effects on brain
Consider withholding antipyretics when:
- Monitoring antibiotic effectiveness in bacterial infections (masking fever can hide treatment failure)
- Attempting to diagnose unusual fever patterns (e.g., tertian malaria, Pel-Ebstein pattern in Hodgkin disease, temperature-pulse dissociation in typhoid/brucellosis)
- Diagnostic workup is incomplete
Special caution:
- Patients on anticytokine therapy (anti-TNF, anti-IL-1, anti-IL-6, anti-IL-17) or chronic glucocorticoids may have blunted febrile responses - even low-grade fever requires early, rigorous evaluation
- In neonates, elderly, chronic liver/kidney failure: fever may be absent despite serious infection
4. Mechanisms of Antipyretic Agents
Antipyretics work by reducing PGE2 levels in the thermoregulatory center, thereby lowering the elevated hypothalamic set point (Harrison's 22E, Firestein & Kelley's Rheumatology).
| Drug Class | Mechanism |
|---|---|
| NSAIDs / Aspirin | Inhibit cyclooxygenase (COX-1 & COX-2), blocking arachidonic acid conversion to PGE2; also reduce IL-1-induced IL-6 production |
| Selective COX-2 inhibitors | Inhibit COX-2 specifically; excellent antipyretics |
| Acetaminophen (APAP) | Weak peripheral COX inhibitor (inactivated peripherally); in the CNS, oxidized by P450 to an active form that inhibits COX activity + possibly inhibits COX-3 (CNS-specific); also signals through TRPA1 |
| Glucocorticoids | Dual action: (1) inhibit phospholipase A2 (blocks arachidonic acid release) + (2) block transcription of mRNA for pyrogenic cytokines (IL-1, IL-6, TNF) |
5. Pharmacological Treatment
First-Line: Acetaminophen (Paracetamol)
Preferred in most clinical scenarios (Lippincott Pharmacology, Harrison's 22E):
- Oral aspirin and acetaminophen are equally effective at reducing fever in adults
- Acetaminophen is preferred because it does not affect platelets, does not damage the GI tract, and is safe in children with viral infections
- Drug of choice in children - especially those with viral illness or chickenpox (aspirin carries risk of Reye syndrome)
- Available in oral, rectal, and IV formulations
- Typical adult dose: 500-1000 mg every 4-6 hours (max 4 g/day; 2 g/day in hepatic impairment)
Toxicity - the NAPQI pathway:
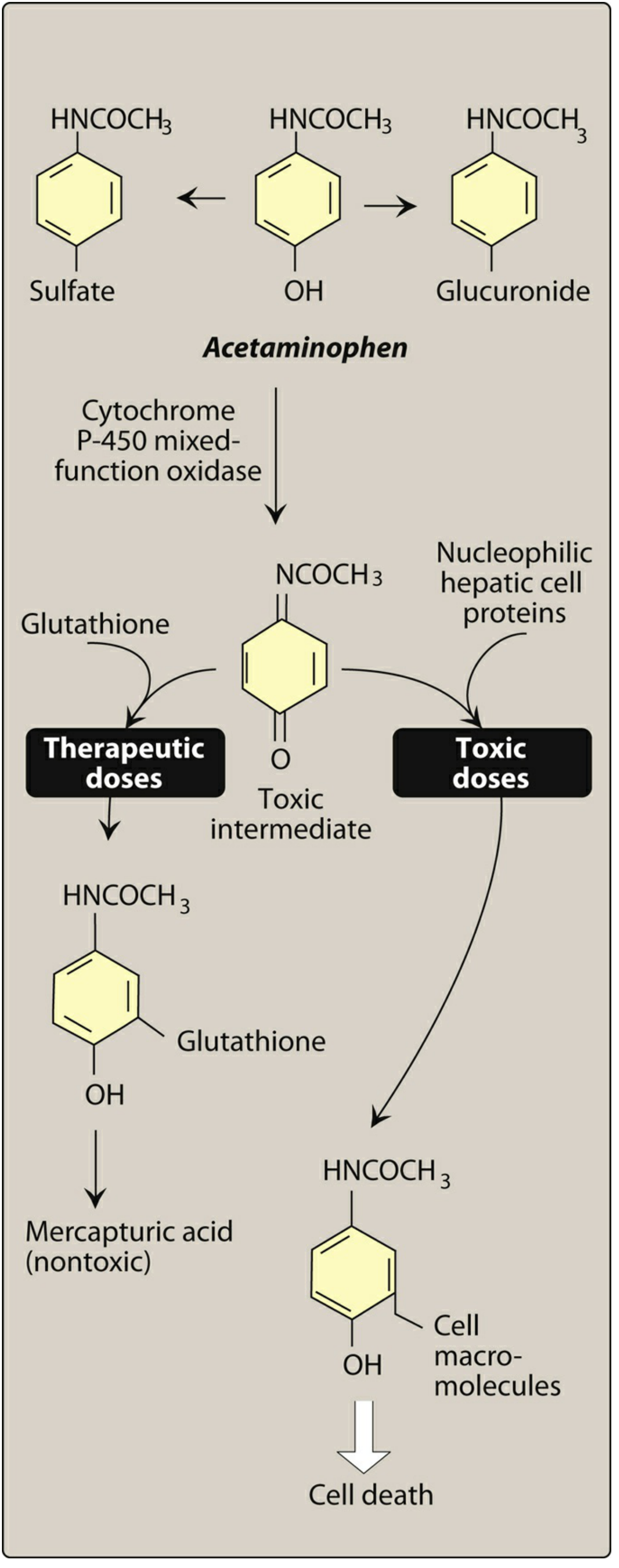
At therapeutic doses, the toxic intermediate NAPQI is safely conjugated with glutathione. At overdose doses, glutathione is depleted and NAPQI binds hepatic proteins, causing hepatic necrosis. Antidote: N-acetylcysteine (replenishes glutathione). Higher risk in: hepatic disease, alcoholism, chronic malnutrition.
NSAIDs (Ibuprofen, Naproxen, Diclofenac, etc.)
- Effective antipyretics; equivalent to acetaminophen in adults
- In children under 2 years, ibuprofen shows improved efficacy over acetaminophen within the first 24 hours, with equivalent safety (Firestein & Kelley's)
- Risks: GI toxicity, platelet inhibition, renal impairment, cardiovascular effects with prolonged use
Aspirin
- Effective but avoided in children (Reye syndrome risk) and those with bleeding risk or GI disease
- Still used in adults for specific indications
Combining/Alternating Antipyretics
- Some guidelines suggest alternating acetaminophen and ibuprofen in children, but evidence for superiority is limited and can cause confusion around dosing schedules. Current 2024-2026 guidelines (S3-Leitlinie Germany, RCH Australia) lean toward symptom-based, not temperature-based, use of a single agent.
6. Non-Pharmacological Measures
- Tepid sponging: Helpful as an adjunct to antipyretics, not as a standalone treatment (Swanson's Family Medicine)
- Cooling blankets: Used in hyperpyrexia, but must not be used without concurrent oral antipyretics (can cause shivering reflex, increasing heat production - Harrison's)
- Evaporative cooling (spray + cool air): Preferred by some for rapid temperature reduction in heatstroke
- Adequate hydration: Fever increases insensible fluid losses; maintain hydration
- Light clothing, well-ventilated environment
- Cold-water bath: Reserved for heatstroke/hyperpyrexia; may need muscle relaxants if shivering is severe
7. Special Clinical Scenarios
Febrile Seizures (Children)
- No definitive correlation between the degree of temperature elevation and seizure onset in susceptible children
- Nevertheless, fever should be aggressively treated in children with any prior history of febrile or nonfebrile seizures
Hyperpyrexia (>41.5°C)
- Requires both antipyretics and physical cooling simultaneously
- Particularly important in CNS disease/trauma where high temperature directly damages neurons (local hemorrhages and parenchymal degeneration)
- Even brief hyperpyrexia can be fatal; neuronal loss is irreversible
Post-Surgical Fever
- ~40% of patients develop fever after major surgery; most have no identifiable cause (Bailey and Love's Surgery, Goldman-Cecil Medicine)
- Workup: blood/urine/wound cultures
- Common causes include atelectasis, wound infection, pneumonia, UTI, line sepsis, DVT, transfusion reactions, drug reactions
- Treatment: address the underlying cause + supportive care (hydration, nutrition)
Neutropenic Fever
- Defined as temperature >38.3°C once, or >38°C sustained for 1 hour, in a patient with ANC <500 cells/μL
- Requires urgent empirical broad-spectrum antibiotics - delay is life-threatening
- Full management protocol in Harrison's 22E (MANAGEMENT OF NEUTROPENIC FEVER)
Critically Ill Patients (ICU Fever)
- 2024 SCCM/IDSA guidelines: against routine antipyretic use solely for temperature reduction in critically ill patients (moderate-quality evidence; no mortality benefit)
- Weak recommendation to use antipyretics for patient comfort or symptom control
- A 2025 meta-analysis of 16 RCTs (n=2,186) confirmed: antipyretics modestly reduce temperature (mean -0.41°C) but have no effect on 28-day mortality, hospital mortality, or shock reversal
Autoinflammatory/Autoimmune Diseases
- Recurrent fever in Still disease, familial Mediterranean fever, gout, idiopathic pericarditis
- IL-1 blockade (anakinra, canakinumab) dramatically reduces fever in autoinflammatory conditions
- These patients also respond to standard antipyretics
8. Summary: Antipyretic Choice at a Glance
| Patient Group | Drug of Choice | Notes |
|---|---|---|
| Adults (general) | Acetaminophen | First choice; GI-safe |
| Adults with inflammatory disease | NSAID or Acetaminophen | NSAID if anti-inflammatory effect needed |
| Children (any age, viral illness) | Acetaminophen | Aspirin contraindicated (Reye) |
| Children <2 years | Ibuprofen | Faster onset at 24 h vs. acetaminophen |
| GI risk / platelet issues | Acetaminophen | Avoid NSAIDs |
| Hepatic impairment | NSAID (short course) | Reduce/avoid acetaminophen |
| ICU / critically ill | Antipyretics for comfort only | No mortality benefit from routine use |
| Hyperpyrexia | Antipyretic + physical cooling | Combined approach mandatory |
| Neutropenic fever | Empirical antibiotics (primary) | Antipyretics for comfort only |
Sources:
- Guyton and Hall Textbook of Medical Physiology (body temperature regulation)
- Harrison's Principles of Internal Medicine, 22E (fever pathophysiology, treatment regimens)
- Lippincott Illustrated Reviews: Pharmacology (acetaminophen mechanism and toxicity)
- Firestein & Kelley's Textbook of Rheumatology (antipyretic effects of NSAIDs)
- Costanzo Physiology, 7th Ed. (fever mechanism)
- Bailey and Love's Short Practice of Surgery, 28th Ed. (post-surgical fever)
- 2024 SCCM/IDSA Guidelines on fever in critically ill patients (via mp.pl summary)
- 2026 S3 Guideline: Outpatient fever management in children (Dtsch Arztebl Int 2026; 123: 226-30)
This is a shared conversation. Sign in to Orris to start your own chat.