Coup and counter coup injury
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive account of coup and contrecoup (counter-coup) injury, drawn from multiple forensic medicine textbooks.
Coup and Contrecoup (Counter-Coup) Brain Injury
Definitions
- Coup injury (French: coup = blow): Brain injury located directly beneath the point of impact, resulting from the impacting force itself.
- Contrecoup injury (French: contre = opposite, coup = blow): Brain injury located on the side opposite to the impact, away from where the head was struck.
Mechanism
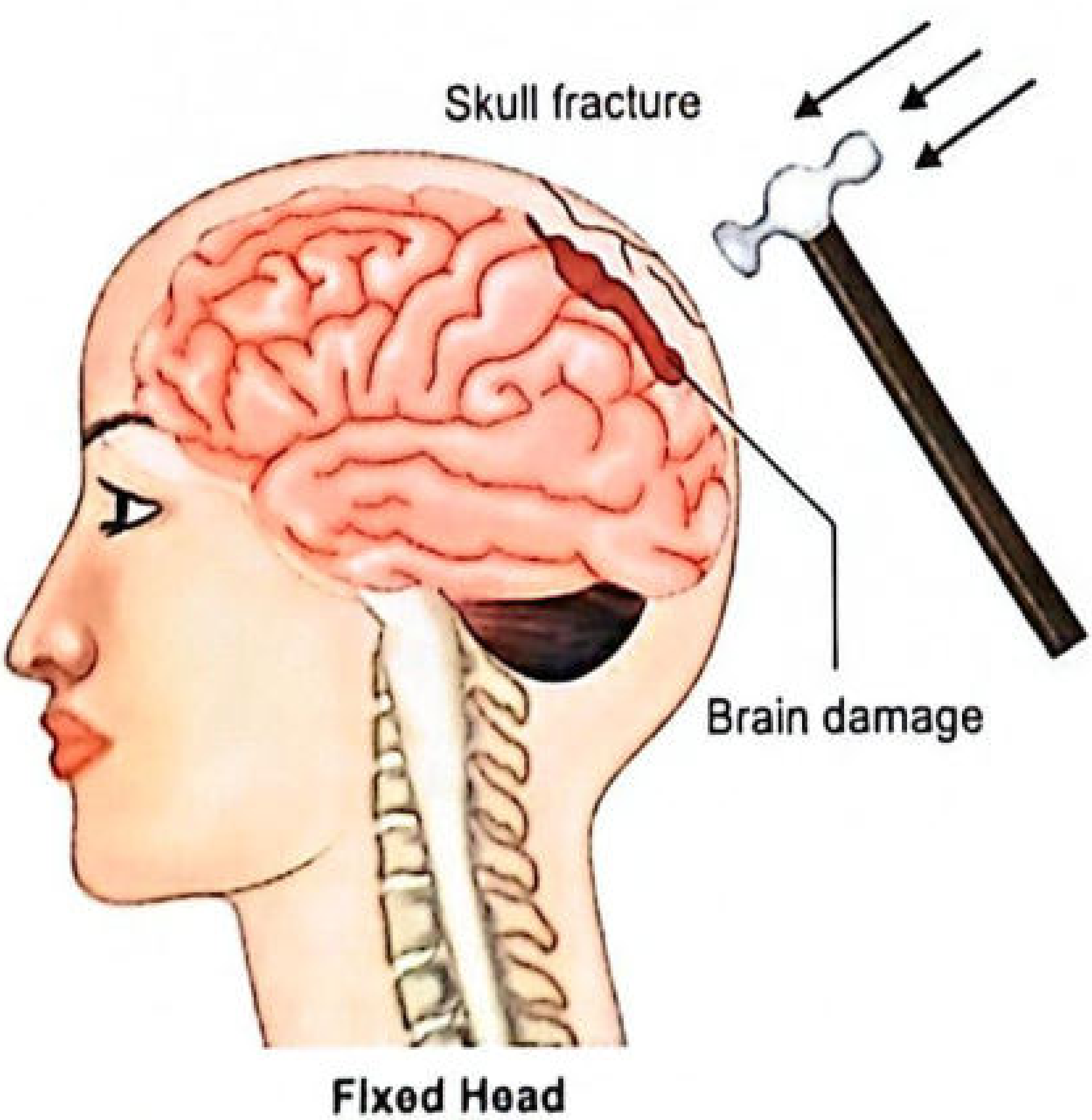
Coup Injury
When a head is fixed (e.g., lying on the ground) and receives a blow, the skull fractures and brain damage occurs at the site of impact. The skull is struck, and the brain immediately beneath the impact is damaged by direct compression and shear forces.
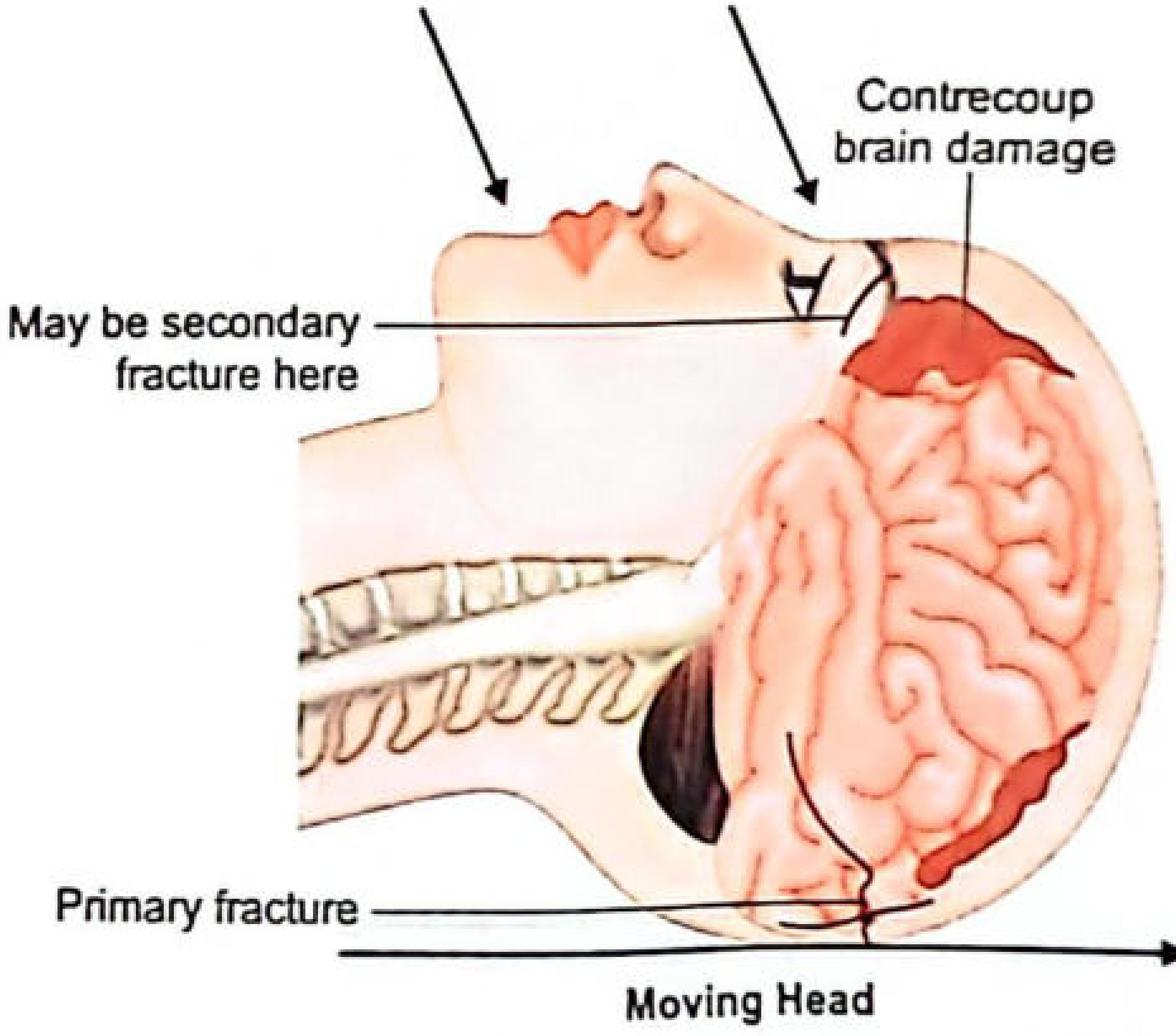
Contrecoup Injury
Contrecoup injury occurs when a moving head is suddenly decelerated by hitting a firm surface (e.g., falling and striking the ground). The brain, still in motion due to inertia, strikes the arrested skull on the opposite side. A vacuum/cavity forms on the contralateral side, exerting a suction effect that further damages brain tissue.
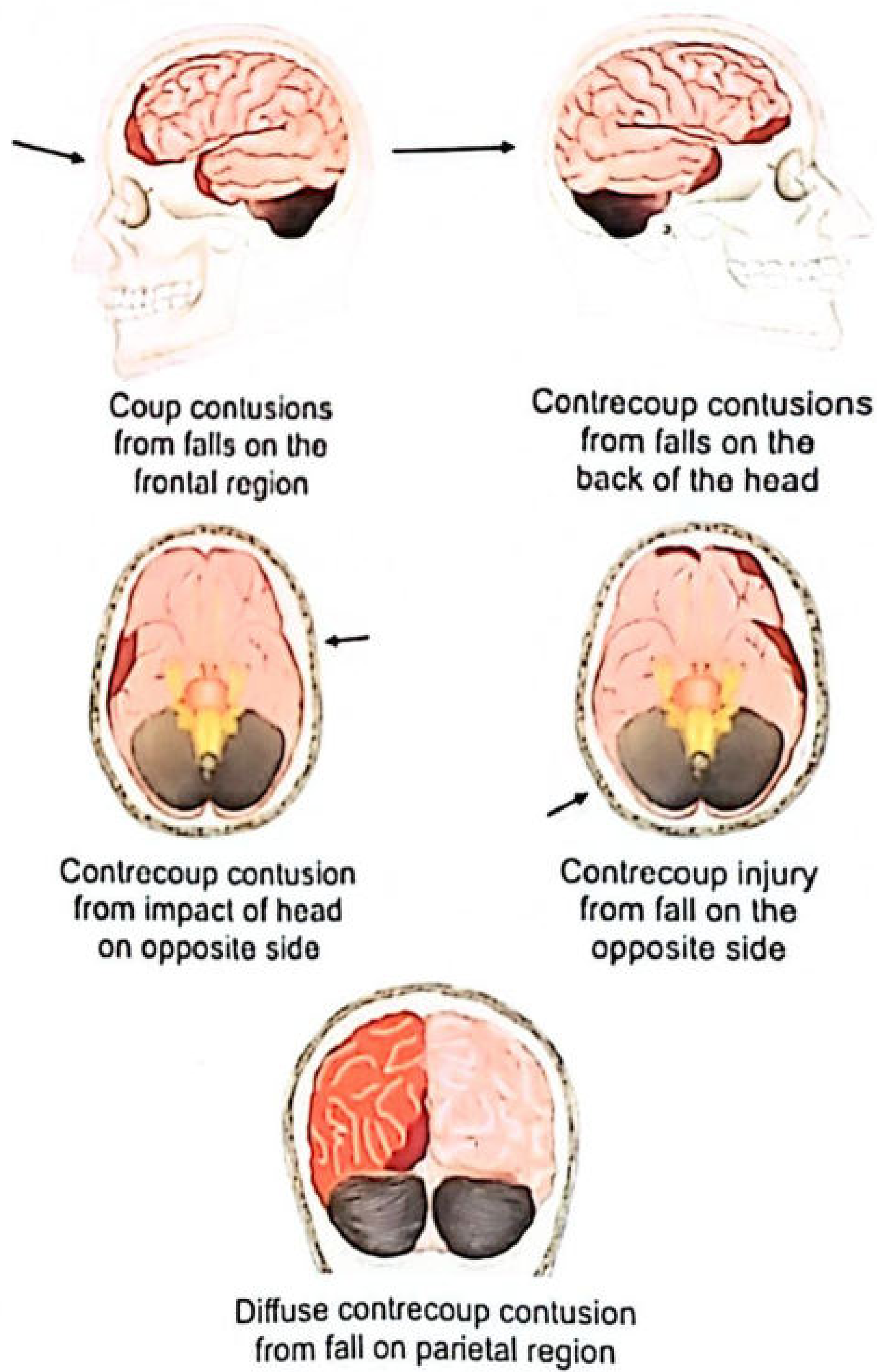
Types of Contusions
| Type | Location | Associated with |
|---|---|---|
| Coup | Directly under point of impact | Blows to a fixed head |
| Contrecoup | Opposite to point of impact | Falls (moving head decelerates) |
| Intermediary coup | Between coup and contrecoup (deep structures - white matter, basal ganglia, brainstem, corpus callosum) | Falls, vertex impact |
Theories Explaining Contrecoup Lesions
-
Struck Hoop Theory: Elasticity of the skull causes it to flatten at the point of impact, becoming ovoid. This transmits forces to the opposite side.
-
Russell's Theory: The brain shifts toward the impact site (like a jelly mass). A potential space develops on the opposite side, injuring vessels and causing subdural and cortical injuries.
-
Gaggio's Pressure Gradient Theory: Impact creates positive pressure at the site of impact and negative pressure on the opposite side, causing vessel rupture on the far side.
-
Holbourn's Shear Strain Theory (Rotational Force Theory) - most accepted: Contrecoup lesions result from local distortion of the skull and sudden rotational acceleration of the head. This produces shear strains (sliding of adjacent brain particles relative to each other) that are greatest at the pole opposite to the impact. This explains why contrecoup injuries are often more extensive than coup injuries.
-
Deceleration/Inertia Theory: Sudden arrest of the moving head causes the brain (still in motion) to strike the inner surface of the stationary skull on the far side.
-
Rawling's Theory of Bony Irregularities: Irregular bony prominences (orbital plates, cribriform plate, lesser wings of sphenoid) lacerate the base of the frontal lobes and temporal lobe tips as the brain slides across them during impact.
Practical Points
- Sometimes only the contrecoup lesion is present with no coup damage at all.
- Skull fracture is not required for coup or contrecoup injuries to occur.
- The most common site for contrecoup injury is the frontal lobe (tips of frontal poles), especially after a fall on the occiput - often bilateral/symmetrical.
- In temporal and parietal impacts, contrecoup lesions tend to be diametrically opposite on the contralateral brain surface.
- A fall on the frontal region virtually never produces occipital contrecoup (due to the relatively smooth posterior cranial fossa floor).
- In temporal impact, contrecoup damage may occur on the opposite side of the ipsilateral hemisphere (striking the falx cerebri) rather than the contralateral hemisphere.
- Severe contrecoup from occipital fall can fracture the orbital plate floor, allowing meningeal blood to track into the orbits and present as bilateral black eyes ("raccoon eyes").
- Contrecoup lesions can also occur when a fixed head is struck (not only in falls), if force is sufficient.
- Contrecoup lesions take the form of cortical contusions or lacerations.
- Contrecoup injuries are rare before age 3 years.
Medicolegal Importance (Blow vs. Fall)
This distinction is of significant medicolegal value:
| Feature | Blow to the head | Fall on the head |
|---|---|---|
| Coup contusions | Large/prominent | Small or absent |
| Contrecoup contusions | Small or absent | Large/prominent |
| Head condition | Fixed | Moving (decelerates on impact) |
A line drawn between the centers of the coup and contrecoup lesions indicates the direction of impact relative to the head, which helps reconstruct the event.
Classic example: A person struck on the chin falls backward and strikes their occiput on the pavement. The autopsy may show a skull fracture at the occiput and severe contrecoup contusions of the frontal lobes with bilateral black eyes - consistent with a single blow to the chin, vindicating the assailant of a more serious charge. (Parikh's Textbook of Medical Jurisprudence)
Common Sites of Contrecoup Injury
- Frontal poles and orbital surfaces of frontal lobes
- Temporal poles
- (Rarely) Occipital lobes (almost never seen even after frontal falls)
Sources: P.C. Dikshit Textbook of Forensic Medicine and Toxicology; Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology; The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026); DiMaio's Forensic Pathology, 3rd ed.
This is a shared conversation. Sign in to Orris to start your own chat.