Thoracic duct anatomy course and it's clinical significance Full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the content needed for a comprehensive MD-exam-level answer. Let me compose the full detailed response.
Thoracic Duct - Anatomy, Course & Clinical Significance
Definition and General Description
The thoracic duct is the largest and most important lymphatic vessel in the body, measuring 38-45 cm in length and 2-5 mm in diameter. It is the principal channel through which lymph from most of the body is returned to the venous circulation. It drains approximately three-quarters of the entire body's lymph - everything except the right upper extremity, right breast, right lung, and right side of the head/neck (which are drained by the right lymphatic duct).
- Gray's Anatomy for Students, p. 270
- Fischer's Mastery of Surgery, p. 2442
Embryological Development
The thoracic duct develops from a complex fusion of bilateral lymphatic channels. It is formed by:
- The caudal part of the right thoracic duct
- The anastomosis between the left and right thoracic ducts
- The cranial part of the left thoracic duct
The right lymphatic duct is derived from the cranial part of the right thoracic duct. This complex embryological origin explains the extreme variability in the course, origin, and termination of the thoracic duct encountered in clinical practice.
- The Developing Human (Moore's Embryology), p. 885
Course and Anatomy
The course is best understood in three segments: abdominal, thoracic (posterior mediastinum), and cervical (superior mediastinum + root of neck).
1. Abdominal Segment - Origin at Cisterna Chyli
- The duct begins at the cisterna chyli (chyle cistern), a saccular dilation located in the retroperitoneal space at the level of L1-L2 (between the aorta and right crus of diaphragm)
- The cisterna chyli receives:
- Intestinal lymphatic trunks (from intestines and unpaired abdominal viscera)
- Two lumbar lymphatic trunks (from lower limbs, pelvis, kidneys, adrenals, abdominal wall)
- The cisterna chyli is absent in up to 50% of individuals (direct confluence of trunks instead)
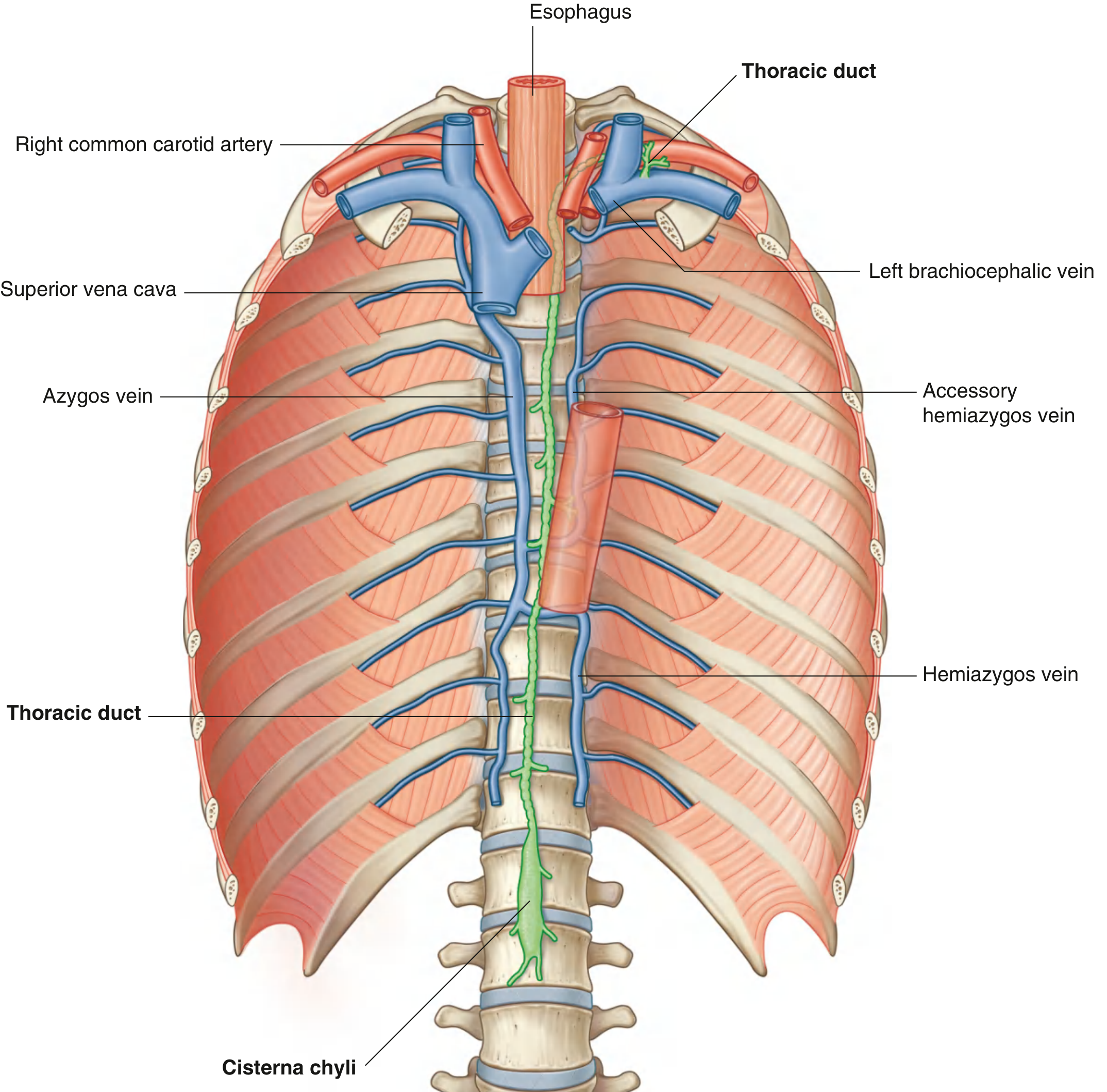
2. Thoracic Segment - Posterior Mediastinum
The thoracic duct enters the thorax through the aortic hiatus of the diaphragm at T10-T12, then travels in the posterior mediastinum:
| Level | Position | Anatomical Relations |
|---|---|---|
| T12 to ~T5 | Right of midline | Thoracic aorta on LEFT, azygos vein on RIGHT, esophagus ANTERIORLY, vertebral bodies POSTERIORLY |
| T5 (TV) | Crosses midline to the LEFT | Passes behind the aorta/aortic arch |
| T5 to thoracic inlet | Left of midline | Left mediastinal pleura laterally, esophagus medially |
The crossing at T5 is the key anatomical pivot point - above this level, injuries cause left-sided chylothorax; below T5, injuries may cause right-sided chylothorax.
The duct also receives, within the thorax:
- Descending thoracic lymph trunks from the lower 6-7 intercostal spaces (both sides)
- Upper intercostal trunks from upper left 5-6 intercostal spaces
- Ducts from posterior mediastinal nodes
- Ducts from posterior diaphragmatic nodes
3. Cervical Segment - Superior Mediastinum and Root of Neck
On entering the superior mediastinum, the duct passes:
- Posterior to the arch of the aorta
- Posterior to the initial portion of the left subclavian artery
- Between the esophagus and left mediastinal parietal pleura
In the root of the neck, it arches laterally:
- Passes posterior to the carotid sheath
- Turns inferiorly in front of the thyrocervical trunk, phrenic nerve, and vertebral artery
- Just medial to the anterior scalene muscle, it courses inferiorly
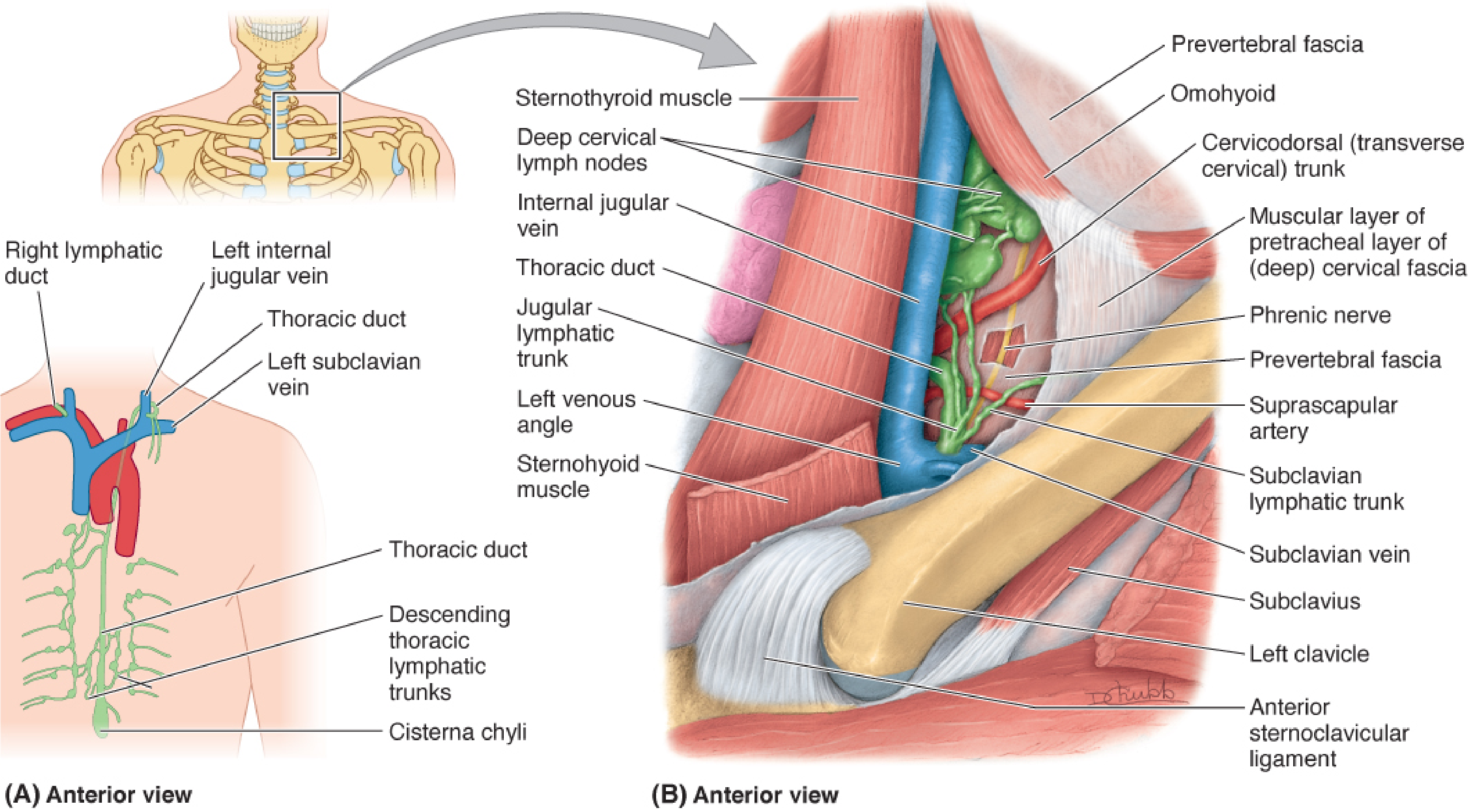
4. Termination
The thoracic duct terminates by draining into the junction (angle) of the left internal jugular vein and left subclavian vein (the left venous angle / Pirogoff's angle). Just before termination, it is joined by:
- Left jugular trunk - drains left head and neck
- Left subclavian trunk - drains left upper limb
- Occasionally, the left bronchomediastinal trunk - from left thoracic structures
On the right side: A similar but smaller confluence empties into the right venous angle, either as a single right lymphatic duct or as three separate trunks (right jugular, right subclavian, right bronchomediastinal).
Tributaries - Summary Table
| Tributary | Region Drained |
|---|---|
| Cisterna chyli | Lower limbs, pelvis, perineum, abdominal viscera and walls |
| Intercostal trunks (lower 6-7 spaces, bilateral) | Thoracic wall |
| Left upper intercostal trunks | Upper left thorax |
| Posterior mediastinal nodes | Mediastinal structures |
| Left jugular trunk (at termination) | Left head and neck |
| Left subclavian trunk (at termination) | Left upper limb |
Structural Features
- Contains bicuspid valves to prevent backflow (appears beaded on imaging)
- Wall is thin and transparent
- Chyle (milky appearance) when carrying fat absorbed from the GI tract - contains chylomicrons, lymphocytes, proteins, fat-soluble vitamins
- Daily flow: ~1.5-2.5 liters of chyle per day (up to 4L postprandially)
Clinical Significance
1. Chylothorax (Most Important)
Definition: Presence of chyle in the pleural space due to thoracic duct disruption.
Causes:
- Surgical/iatrogenic (most common): esophagectomy, pneumonectomy, neck dissection, aortic surgery, vertebral surgery
- Traumatic: blunt/penetrating chest trauma, forceful vomiting, central venous line placement
- Non-traumatic/spontaneous: lymphoma (most common malignant cause), metastatic carcinoma, thoracic aortic aneurysm, filarial lymphangitis
Side of chylothorax:
- Injury below T5 (below the crossing) → right-sided chylothorax
- Injury above T5 (above the crossing) → left-sided chylothorax
- If both pleural membranes are breached → bilateral
Diagnosis:
- Pleural fluid: milky, non-purulent (but may be clear if patient is NPO)
- Triglycerides > 110 mg/dL = almost certain chylothorax (99% accuracy)
- Triglycerides < 50 mg/dL = only 5% chance of chylothorax
- Chylomicrons in fluid: most specific test
- High lymphocyte count in pleural fluid
Consequences if untreated:
- Protein depletion (chyle contains albumin)
- Lymphopenia and immunosuppression
- Metabolic acidosis, electrolyte imbalance
- Volume depletion
- Death (in severe cases)
Management:
-
Conservative (low-output < 500 mL/day): NPO or low-fat diet with medium-chain triglycerides (MCT diet - MCTs are absorbed directly into portal blood, bypassing the lymphatics), parenteral nutrition, octreotide (somatostatin analogue - reduces lymph flow)
-
Surgical (high-output > 1000 mL/day persisting > 2 weeks): Thoracic duct ligation (at aortic hiatus, T12 level - most consistent location). Can be done via thoracotomy or VATS
-
Interventional radiology: Lymphangiography + percutaneous thoracic duct embolization
-
Schwartz's Principles of Surgery, p. 769
-
Bailey and Love's Surgery, p. 829
2. Iatrogenic Injury During Neck Dissection
The thoracic duct is vulnerable during left neck dissection at Level IV (supraclavicular region), when lymph node dissection approaches the confluence of the internal jugular and subclavian veins.
- Damage may produce a chyle fistula discharging up to 2 L/day from the wound
- If recognized intraoperatively: ligate the proximal end (safe, as anastomotic channels exist between lymphatic and venous systems in the lower neck)
- If undetected: chyle appears from wound within 24 hours of surgery
- Low-flow leaks: conservative management (low-fat diet + octreotide)
- High-output leaks: TPN + surgical re-exploration
3. Ligation is Safe
Ligation of the thoracic duct is clinically safe because:
- Numerous lymphovenous anastomoses exist in the lower neck and elsewhere
- Collateral lymphatic channels rapidly take over drainage
- This is the basis for surgical treatment of chylothorax by mass ligation at the aortic hiatus
4. Sentinel Lymph Node / Virchow's Node (Troisier's Sign)
- The thoracic duct drains into the left venous angle, which corresponds to the region of Virchow's node (left supraclavicular lymph node)
- Metastatic tumor cells from abdominal and thoracic malignancies (gastric, pancreatic, esophageal, testicular, ovarian) may travel via the thoracic duct and deposit in Virchow's node
- Troisier's sign = palpable hard left supraclavicular node = indicator of advanced intra-abdominal malignancy
5. Relation to Esophagectomy
- The thoracic duct runs immediately posterior to the esophagus throughout its thoracic course
- During esophagectomy, the duct is at direct risk of injury
- Chylothorax is the most common major lymphatic complication of esophagectomy (incidence ~1-9%)
- Prophylactic mass ligation of the thoracic duct at the level of the aortic hiatus is recommended in some centers to reduce this risk
6. Thoracic Duct Cysts
- Rare mediastinal cysts arising from the thoracic duct
- Typically found in the posterior mediastinum
- May present with dysphagia or dyspnea
- Treated by surgical excision
7. Role in Fat Absorption and Nutrition
- Long-chain fatty acids absorbed in the small intestine are packaged as chylomicrons and transported via the lymphatics (lacteals → mesenteric lymphatics → cisterna chyli → thoracic duct → venous circulation)
- Medium-chain triglycerides (MCTs) bypass this route and are absorbed directly into the portal blood - this is the pharmacological basis of MCT diet in chylothorax management
Summary Memory Aid
Origin: Cisterna chyli at L1-L2
Entry: Aortic hiatus T10-T12
Course: Right side of aorta (below T5) → Crosses at T5 → Left side (above T5)
Relations: Aorta (left), Azygos (right), Esophagus (anterior), Vertebrae (posterior)
Neck: Posterior to carotid sheath, anterior to thyrocervical trunk/phrenic nerve
Ends: Left venous angle (left IJV + left subclavian vein junction)
Drains: 3/4 of body (all except right upper limb, right chest, right head/neck)
Sources:
- Gray's Anatomy for Students, pp. 270, 1176-1177
- Fischer's Mastery of Surgery 8e, p. 2442
- Schwartz's Principles of Surgery 11e, p. 769
- Bailey and Love's Short Practice of Surgery 28e, p. 829
- The Developing Human (Moore's Embryology), p. 885
- Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.