Ingestional paracetamol poisoning
Reading File
Finding Sources
Searching PubMed
"paracetamol poisoning" AND "N-acetylcysteine"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of ingestional paracetamol (acetaminophen) poisoning, drawn from multiple authoritative textbooks.
Ingestional Paracetamol (Acetaminophen) Poisoning
Epidemiology
Paracetamol is the most popular over-the-counter analgesic worldwide and one of the most common toxic exposures reported to poison centers. In the United States, it is the leading cause of drug-induced liver failure, accounting for nearly half of all cases of acute liver failure and approximately 500 deaths annually. Most serious poisonings involve intentional self-harm, though overdoses also occur due to the erroneous belief that the drug is inherently safe, or from unknowing co-ingestion in combination products. - Tintinalli's Emergency Medicine, p. 1294
Pharmacology & Normal Metabolism
After a therapeutic oral dose:
- Rapidly absorbed from the GI tract; peak levels within 30 min - 2 hours
- Volume of distribution ~0.85 L/kg; ~20% protein-bound; half-life ~2.5 hours
- ~90% conjugated as glucuronide (40-67%) or sulfate (20-46%) - both renally excreted
- 5-15% oxidized by CYP450 (mainly CYP2E1) to the reactive metabolite NAPQI (N-acetyl-p-benzoquinoneimine)
- At therapeutic doses, NAPQI is rapidly conjugated by hepatic glutathione (via glutathione-S-transferase) to a non-toxic mercaptate compound, excreted in urine
Recommended Maximum Doses
| Population | Maximum |
|---|---|
| Adults (325 mg tabs) | 3900 mg/day |
| Adults (500 mg tabs) | 3000 mg/day |
| Children | 10-15 mg/kg q4-6h; max 75 mg/kg/day |
Mechanism of Toxicity
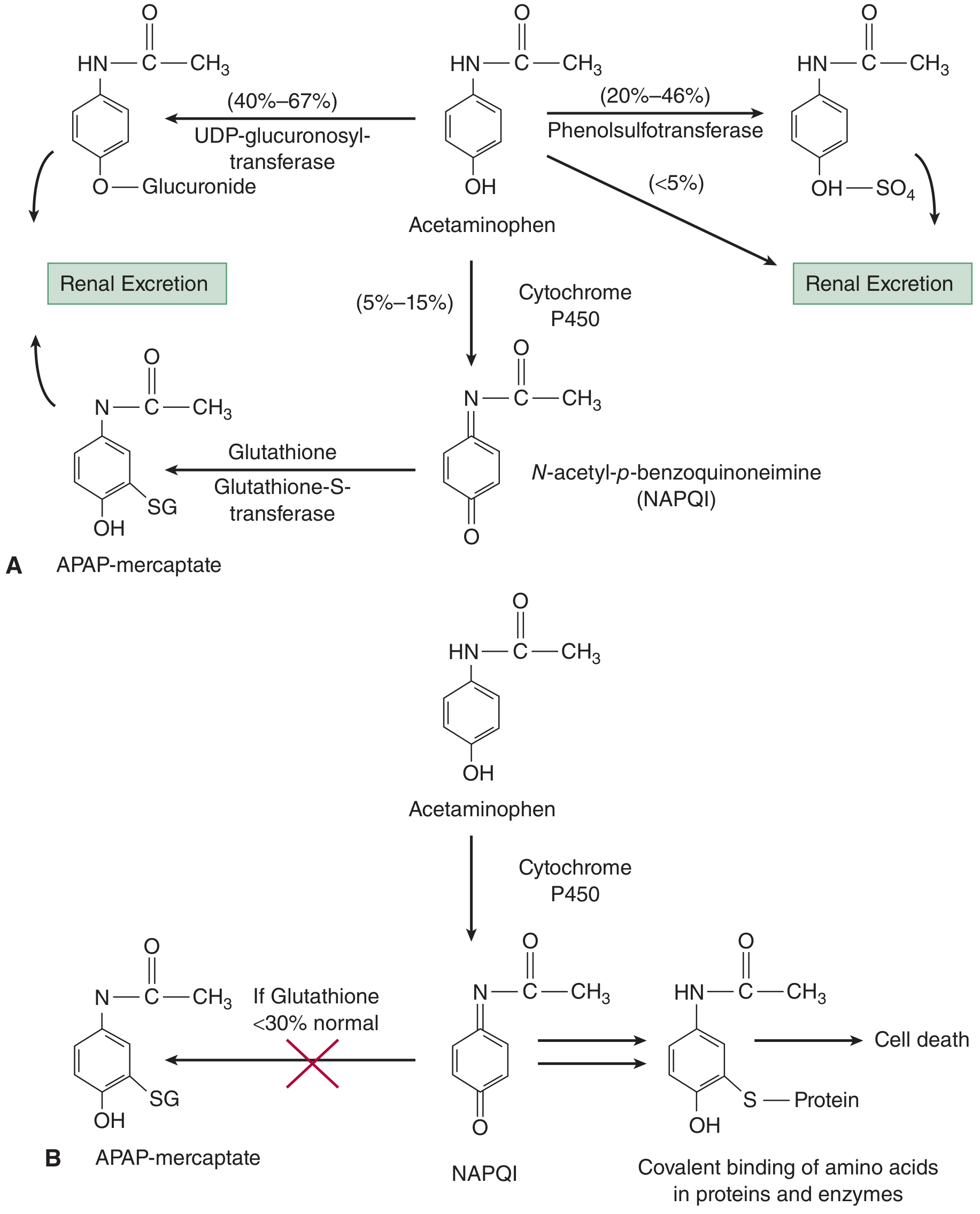
Figure: (A) Normal - glucuronidation/sulfation predominate; small NAPQI detoxified by glutathione. (B) Overdose - CYP450 pathways saturated, NAPQI overwhelms glutathione. When stores fall <30% of normal, free NAPQI binds covalently to hepatocyte proteins, causing centrilobular necrosis.
In overdose:
- Glucuronidation and sulfation pathways become saturated
- A larger fraction is shunted through CYP450 to NAPQI
- NAPQI production depletes hepatic glutathione; when stores fall below 30% of normal, free NAPQI accumulates
- NAPQI binds covalently to intracellular proteins and organelles, primarily in Zone 3 (centrilobular) hepatocytes - the area furthest from portal blood supply
- Result: centrilobular hepatic necrosis - the hallmark histological lesion
- Tintinalli's Emergency Medicine, p. 1295; Histology: A Text and Atlas, p. 1672
High-Risk Groups
- Alcoholics - both reduced glutathione stores AND CYP2E1 induction (dual hit)
- Patients on anticonvulsants (phenytoin, carbamazepine) or antituberculous drugs (rifampicin, INH) - CYP450 induction
- Malnourished patients - depleted glutathione
- HIV/AIDS patients
- Children under 6 years are relatively protected - greater capacity for hepatic sulfation
Clinical Features: Four Stages
| Stage | Timing | Features |
|---|---|---|
| Stage 1 | First 24 h | Anorexia, nausea, vomiting, malaise - or asymptomatic |
| Stage 2 | Days 2-3 | Stage 1 symptoms improve; RUQ pain/tenderness; transaminases rise |
| Stage 3 | Days 3-4 | Fulminant hepatic failure: metabolic acidosis, coagulopathy (elevated PT/INR), encephalopathy, renal failure, recurrent GI symptoms |
| Stage 4 | After day 5 | Recovery over 2 weeks; complete hepatic recovery in 1-3 months in survivors |
Important: The "improvement" in Stage 2 can be deceptive - patients may feel better while liver necrosis is progressing.
Extrahepatic Toxicity
- Isolated acute kidney injury (direct renal tubular toxicity)
- Pancreatitis
- Rarely, cardiac toxicity
- In massive overdose (>500 mg/kg or serum level >750 mcg/mL): early metabolic acidosis with elevated lactate and altered mental status, even without liver failure - likely from glutathione depletion generating 5-oxoproline and mitochondrial respiratory inhibition
Diagnosis
When to Suspect Toxic Exposure
| Patient | Threshold |
|---|---|
| Age ≥6 years | >10 g or >200 mg/kg single ingestion; >10 g or 200 mg/kg over 24 h; or >6 g / 150 mg/kg per day for ≥2 consecutive days |
| Age <6 years | ≥200 mg/kg single or over 8 h; or ≥150 mg/kg/day for preceding 48 h |
Measure serum acetaminophen concentration in all patients with intentional overdose, regardless of history - patients who deny paracetamol ingestion may still have toxic levels.
The Rumack-Matthew Nomogram
- Plots serum acetaminophen concentration (y-axis) against time post-ingestion (x-axis) to predict hepatotoxicity risk
- Only valid for single acute oral ingestion, serum drawn 4-24 hours post-ingestion
- Original line: 4-hour level of 200 mcg/mL; modified (current) treatment line: 4-hour level of 150 mcg/mL (1000 micromol/L) - to increase safety margin
- Above the treatment line: ~60% risk of hepatotoxicity (ALT >1000 IU/L), 1% renal failure risk, 5% mortality (based on pre-antidote era data)
- Very high levels (parallel line at 4-hour concentration of 300 mcg/mL): near-certain hepatotoxicity, higher mortality
Treatment
1. Initial Resuscitation & GI Decontamination
- Secure airway if GCS impaired
- Activated charcoal (1 g/kg orally) if presentation within 1-2 hours of ingestion and airway is protected - reduces absorption
- IV fluids, antiemetics (paracetamol causes nausea)
2. N-Acetylcysteine (NAC) - The Antidote
NAC works by:
- Replenishing glutathione (precursor supply)
- Directly conjugating NAPQI
- Acting as antioxidant
Timing is everything:
- Given within 8 hours of ingestion: nearly 100% effective at preventing hepatotoxicity
- Effectiveness declines with each hour of delay
- Still beneficial even in late presentation with established hepatic failure (improves cerebral perfusion, reduces oxidative stress)
IV NAC Protocol (Standard 21-hour "Three-Bag" Regimen)
| Bag | Dose | Duration |
|---|---|---|
| 1st | 150 mg/kg in 200 mL 5% dextrose | Over 1 hour (loading) |
| 2nd | 50 mg/kg in 500 mL 5% dextrose | Over 4 hours |
| 3rd | 100 mg/kg in 1000 mL 5% dextrose | Over 16 hours |
A newer two-bag regimen (fewer anaphylactoid reactions from the rapid 1st bag) has been compared in recent meta-analysis (PMID: 40013897, 2025) and is gaining acceptance.
Oral NAC
- Loading dose: 140 mg/kg, then 70 mg/kg q4h x 17 doses (total 72 hours)
- Used when IV not available; limited by vomiting
3. Special Situations
Multiple-dose / staggered ingestions:
- Nomogram cannot be applied (no single time of ingestion)
- Assume ingestion started at the earliest stated time and plot accordingly (conservative approach)
Extended-release preparations:
- Obtain a second acetaminophen level 4-6 hours after the first (at 4-8 hours post-ingestion)
- If second level rises above nomogram line, treat with full NAC course
Massive overdose (>40 g or >500 mg/kg):
- Standard 21-hour protocol may be inadequate
- Options: add oral NAC to IV protocol; increase 3rd bag to 200 mg/kg over 16 hours; reload regimen if serum levels remain high at completion
4. Monitoring During Treatment
- LFTs (AST/ALT), bilirubin, PT/INR, creatinine, glucose every 12-24 hours
- Serum lactate, blood gas in severe cases
- Consider stopping NAC when: serum acetaminophen undetectable, ALT/AST normalizing, INR <2, and patient asymptomatic
5. Liver Transplantation
- For fulminant hepatic failure not responding to NAC
- King's College Criteria (KCC) used to stratify transplant candidacy:
- Arterial pH <7.3 after resuscitation, OR
- All three of: PT >100 sec, creatinine >300 micromol/L, Grade III-IV encephalopathy
Key Labs to Order
| Test | Significance |
|---|---|
| Serum paracetamol level (at ≥4 h) | Nomogram assessment |
| AST/ALT | Hepatotoxicity marker (>1000 IU/L = hepatotoxicity) |
| PT/INR | Severity marker; prognostic |
| Serum creatinine | Renal toxicity |
| Blood glucose | Hypoglycemia in hepatic failure |
| Arterial blood gas + lactate | Metabolic acidosis in massive OD |
| Bilirubin | Late hepatic failure marker |
Summary Points
- Paracetamol poisoning is the #1 cause of acute liver failure in the UK and USA
- Toxicity is mediated by NAPQI overwhelming hepatic glutathione stores
- Pathological lesion: centrilobular (Zone 3) necrosis
- Use the Rumack-Matthew nomogram (4-24 h post single ingestion) to guide NAC treatment
- NAC within 8 hours = ~100% prevention of hepatotoxicity
- Monitor for the "Stage 2 trap" - apparent clinical improvement while hepatic necrosis progresses
- Always check serum levels in ALL intentional overdose patients
- In massive overdose, consider augmented NAC dosing or liver transplantation
Recent evidence note: A 2025 systematic review and meta-analysis (PMID: 40013897) comparing two-bag vs. three-bag NAC regimens is worth reviewing, as practice in some centers is shifting toward the two-bag protocol to reduce anaphylactoid reactions from the rapid first infusion.
Sources: Tintinalli's Emergency Medicine (A Comprehensive Study); Henry's Clinical Diagnosis and Management by Laboratory Methods; Histology: A Text and Atlas with Correlated Cell and Molecular Biology; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.