Spread of Ludwig’s angina through what and to what spaces am areas flow diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive information to construct a detailed flow diagram of Ludwig's angina spread. Let me compile everything.
Ludwig's Angina — Spread Through Fascial Planes: Flow Diagram
Spread is direct through fascial planes, NOT via lymphatics — hence bilateral involvement without lymphadenopathy. — K.J. Lee's Essential Otolaryngology; ROSEN's Emergency Medicine
Primary Source → Initial Spaces
Periapical abscess of mandibular molar teeth
(roots insert below the mylohyoid muscle; lingual cortex is thin)
│
│ erodes through cortical plate of mandible
▼
Tracks along deep fascial planes
│
┌─────┼─────────────┐
▼ ▼ ▼
Sublingual Submental Submandibular
space space space
(above (midline, (below mylohyoid,
mylohyoid) anterior) bilateral)
│ │ │
└────────────┴─────────────┘
│
All 3 spaces involved = LUDWIG'S ANGINA
(bilateral, brawny, board-like cellulitis)
The sublingual and submandibular spaces communicate at the posterior border of the mylohyoid muscle. The submandibular space can bypass the anterior belly of digastric, entering the submental and contralateral submandibular space.
— ROSEN's Emergency Medicine
Secondary Spread (from Ludwig's spaces → deep neck)
Ludwig's Angina
(sublingual + submental + submandibular spaces)
│
│ via styloglossus muscle / posterior communication
▼
Parapharyngeal space
(lateral pharyngeal space)
│
┌─────┴──────────────┐
▼ ▼
Retropharyngeal Carotid sheath
space (carotid artery,
internal jugular vein,
vagus nerve)
│
┌─────┴──────────────┐
▼ ▼
"Danger space 4" Prevertebral
(between alar & space
prevertebral fascia)
│
▼
MEDIASTINUM
(mediastinitis, pleural
effusion, empyema,
pericarditis)
— Harrison's Principles of Internal Medicine 22e; ROSEN's Emergency Medicine; Current Surgical Therapy 14e
Anatomical Cross-Section (textbook image)
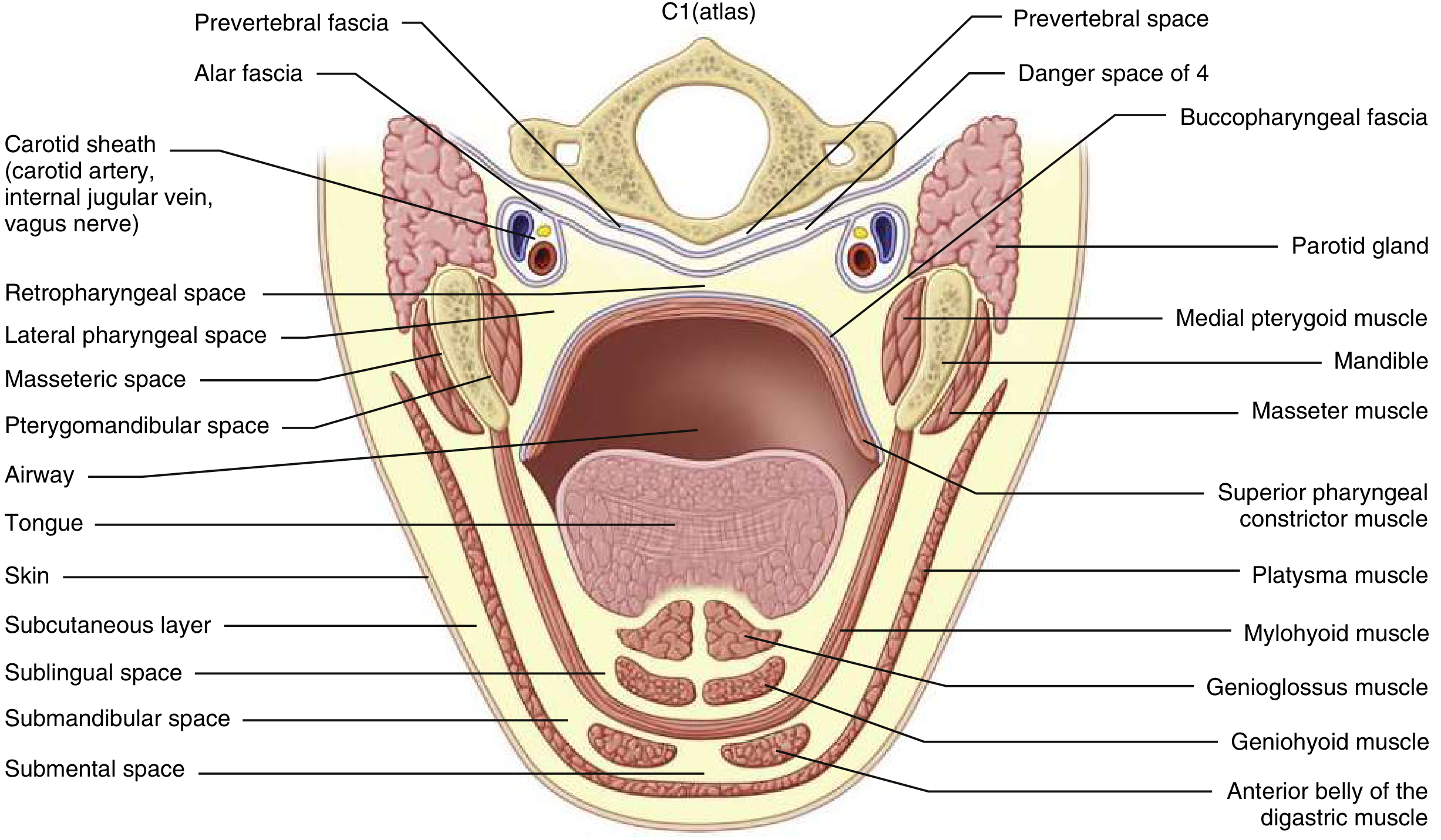
Anatomy of maxillofacial space infections showing all relevant spaces — ROSEN's Emergency Medicine, Fig. 56.8
Complications Along the Spread Path
| Space Involved | Complication |
|---|---|
| Sublingual/Submandibular/Submental | Tongue elevation → airway obstruction (most feared) |
| Parapharyngeal space | Deep neck infection, trismus |
| Retropharyngeal space | Retropharyngeal abscess |
| Carotid sheath | Jugular vein thrombosis (→ Lemierre syndrome) |
| Danger space 4 / Mediastinum | Descending necrotizing mediastinitis, empyema, pericarditis |
| Meninges / skull base | Meningitis, brain abscess |
Key Mechanism Points
- Medium of spread: Fascial planes (NOT lymphatics) → bilateral, symmetric, no lymphadenopathy
- Most common source: Mandibular 2nd/3rd molar periapical abscesses (~80%)
- Other sources: Mandibular fracture, tongue piercing, oral trauma, iatrogenic lacerations, secondarily infected malignancy
- Microbiology: Polymicrobial — oral flora; anaerobes + aerobes (Streptococcus spp. most common aerobe; Bacteroides, Fusobacterium anaerobes)
- Why bilateral: The posterior submandibular spaces communicate openly with each other, allowing direct crossing to the contralateral side
— ROSEN's Emergency Medicine; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22e; K.J. Lee's Essential Otolaryngology
Surgical importance of Retropharyngeal space
Finding Sources
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.