10 common heart disease with ecg changes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive reference covering the 10 most common heart diseases and their ECG changes, synthesized from Harrison's Principles of Internal Medicine 22E, Ganong's Review of Medical Physiology, Braunwald's Heart Disease, and Tintinalli's Emergency Medicine.
10 Common Heart Diseases and Their ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia. Three simultaneous electrical events occur: rapid repolarization, decreased resting membrane potential (K+ leak), and delayed depolarization - all generating a current of injury toward overlying leads.
ECG Changes (evolve over hours to weeks):
- Hyperacute phase (minutes): Tall, broad, peaked "hyperacute" T waves
- Acute phase (hours): ST elevation (convex/tombstone) in leads overlying the infarct; reciprocal ST depression in opposite leads
- Established phase (days): Pathological Q waves (>40 ms wide, >25% of R-wave amplitude); T-wave inversions develop
- Chronic phase (weeks-months): Persistent Q waves; ST normalizes; T waves may normalize or remain inverted
Localization:
| Territory | Elevated leads | Reciprocal depression |
|---|---|---|
| Anterior (LAD) | V1-V4 | II, III, aVF |
| Inferior (RCA/LCx) | II, III, aVF | I, aVL |
| Lateral (LCx) | I, aVL, V5-V6 | V1-V3 |
| Posterior | Tall R in V1-V2, ST depression V1-V3 | (mirror image) |
| Right ventricle | ST elevation V1, V4R | - |
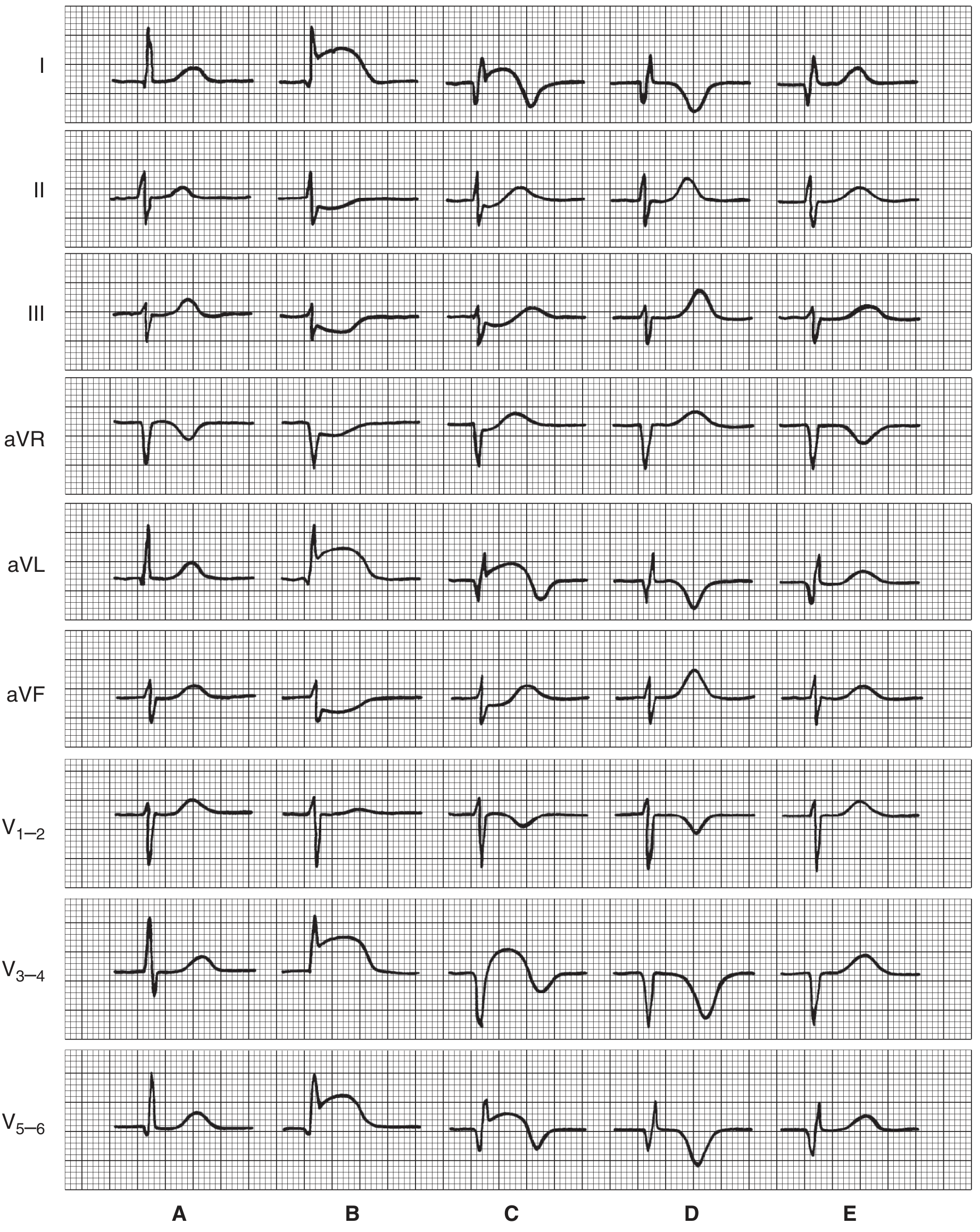
Serial ECG patterns in anterior infarction - Ganong's Review of Medical Physiology, p.534
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
Pathophysiology: Partial/transient coronary occlusion causing subendocardial ischemia. The ischemic ST vector shifts toward the endocardium and ventricular cavity.
ECG Changes:
- ST depression (horizontal or downsloping) ≥0.5 mm in 2 or more contiguous leads
- T-wave inversions (symmetrical, deep) - especially V1-V4 with LAD disease
- Wellens T-wave sign: Deep symmetrical T inversions in V2-V3 = critical proximal LAD stenosis
- No ST elevation; no pathological Q waves (by definition)
- ECG may be entirely normal in ~50% of cases at presentation
3. Atrial Fibrillation (AF)
Pathophysiology: Multiple chaotic re-entrant wavelets in the atria; AV node conducts irregularly.
ECG Changes:
- No distinct P waves - replaced by chaotic fibrillatory baseline (f-waves, >350/min)
- Irregularly irregular RR intervals (the hallmark)
- Variable ventricular rate (typically 100-160/min if uncontrolled)
- QRS usually narrow (unless aberrant conduction or WPW)
- May show signs of underlying cause: RVH pattern if pulmonary hypertension (R/S >1 in V1, right axis deviation, ST depression V1-V3)
4. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: Accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle before normal conduction arrives.
ECG Changes (in sinus rhythm):
- Short PR interval (<120 ms) - AV node delay is bypassed
- Delta wave - slurred upstroke at the start of a widened QRS complex
- Wide QRS (>120 ms) due to ventricular fusion (accessory + normal)
- Secondary ST-T changes (discordant to the delta wave)
During tachycardia:
- Orthodromic AVRT: narrow-complex tachycardia (most common, 65%)
- Antidromic AVRT: wide-complex tachycardia
- AF with WPW: irregular, very rapid, wide complex - can degenerate to VF (dangerous)
5. Left Bundle Branch Block (LBBB)
Pathophysiology: Block in the main left bundle branch forces the septum and left ventricle to depolarize late via the right bundle, producing abnormally wide, discordant complexes.
ECG Changes:
- Wide QRS ≥120 ms
- Broad, notched R waves (M-shaped) in lateral leads (I, aVL, V5-V6)
- QS or rS complexes in V1 (deep S wave or QS)
- No septal Q waves in lateral leads
- Discordant ST-T changes (ST/T opposite to QRS direction)
- New LBBB = treated as STEMI equivalent if new in the setting of chest pain (Sgarbossa criteria apply)
- A new LBBB is the equivalent of ischemic ECG changes and warrants emergency evaluation
6. Right Bundle Branch Block (RBBB)
Pathophysiology: Block in the right bundle branch; right ventricle depolarizes late via the left bundle system.
ECG Changes:
- Wide QRS ≥120 ms
- RSR' ("rabbit ears" or M-shape) in V1 - the classic finding
- Wide, slurred S waves in I, aVL, V5-V6
- T-wave inversion in V1-V3 (appropriate discordance)
- RBBB with left anterior hemiblock = bifascicular block; adds right axis or left axis deviation
- New RBBB + left anterior hemiblock in acute MI context suggests spread of infarction to the conduction system
7. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Genetic sarcomere mutation leading to asymmetric septal hypertrophy, dynamic LVOT obstruction, and diastolic dysfunction.
ECG Changes (abnormal in >90% of patients):
- Left ventricular hypertrophy (LVH) - high-voltage QRS (Sokolow-Lyon: S in V1 + R in V5/V6 ≥35 mm)
- Left atrial enlargement - broad, notched P wave in II ("P mitrale"), negative terminal deflection in V1
- Deeply inverted, giant T waves - especially in mid-precordial leads (V4-V6); sometimes called "Yamaguchi pattern" in apical HCM
- Abnormal Q waves in lateral/inferior leads (septal hypertrophy)
- Left axis deviation
- ECG is abnormal in over 90% of patients with Friedreich's ataxia-related HCM; LVH increases with younger age at diagnosis
8. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes subepicardial myocardial irritation, producing widespread "current of injury."
ECG Changes (evolve through 4 stages):
- Stage 1 (days 1-2): Diffuse concave ("saddle-shaped") ST elevation in nearly all leads EXCEPT aVR and V1 (where ST is depressed); PR depression in most leads, PR elevation in aVR - this PR depression is highly specific
- Stage 2 (days to week): ST returns to baseline; T waves flatten
- Stage 3 (1-3 weeks): Diffuse T-wave inversions
- Stage 4: T waves normalize (may persist as chronic change)
Key distinction from STEMI: Concave (saddle-shaped) vs convex ST elevation; diffuse vs territorial distribution; PR depression present; no reciprocal changes; no Q waves.
9. Dilated Cardiomyopathy (DCM)
Pathophysiology: Diffuse myocardial disease leading to chamber dilation and reduced systolic function; fibrosis disrupts normal conduction.
ECG Changes:
- Sinus tachycardia (compensatory)
- Left bundle branch block (common, due to fibrosis of conduction system)
- LVH voltage criteria (may be present)
- Nonspecific ST-T changes in lateral leads
- Left atrial enlargement (P mitrale)
- Atrial fibrillation (frequent complication)
- Reduced QRS voltage (if pericardial effusion is also present)
- No specific ECG pattern is pathognomonic; nonspecific T-wave abnormalities, reduced voltage, and left atrial enlargement may be present (Braunwald's Heart Disease)
10. Hyperkalemia (Cardiac Effect - Metabolic Emergency)
Pathophysiology: Elevated extracellular K+ reduces the resting membrane potential gradient of myocardial cells, progressively impairing depolarization and conduction.
ECG Changes (progressive with K+ level):
| K+ Level | ECG Finding |
|---|---|
| 5.5-6.5 mEq/L | Tall, peaked, narrow, symmetric T waves (first sign) |
| 6.5-7.5 mEq/L | Prolonged PR interval; widening QRS |
| 7.5-8.0 mEq/L | Flattening/loss of P waves ("atrial paralysis") |
| >8.0 mEq/L | Markedly wide QRS; sine-wave pattern; ventricular arrhythmias |
| >10 mEq/L | Ventricular fibrillation; asystole |
(From Ganong's Review of Medical Physiology, p.535)
Quick Reference Summary Table
| Disease | Rate | Rhythm | P waves | PR | QRS | ST | T waves | Q waves |
|---|---|---|---|---|---|---|---|---|
| STEMI | Variable | Sinus (may have arrhythmias) | Normal | Normal | Wide if LBBB develops | Elevation (territory) | Hyperacute then inversion | Pathological Q waves |
| NSTEMI/UA | Variable | Sinus | Normal | Normal | Normal | Depression | Deep inversion (Wellens) | None |
| Atrial Fibrillation | 100-160/min | Irregularly irregular | Absent (f-waves) | None | Narrow | Variable | Variable | - |
| WPW | Variable | Sinus (or SVT) | Normal | Short (<120ms) | Wide + delta wave | Discordant | Discordant | Pseudo-Q (delta) |
| LBBB | Variable | Sinus | Normal | Normal | Wide ≥120ms (M in V5-6) | Discordant | Discordant | Absent septal Q |
| RBBB | Variable | Sinus | Normal | Normal | Wide ≥120ms (RSR' V1) | Discordant V1-V3 | Discordant V1-V3 | - |
| HCM | Variable | Sinus or AF | Left atrial enlargement | Normal | LVH voltages | - | Giant T inversions (apical) | Septal Q waves |
| Acute Pericarditis | Sinus tachycardia | Sinus | Normal | PR depression | Normal | Diffuse concave elevation | Flat then inverted | None |
| DCM | Tachycardia | AF common | Left atrial enlargement | Prolonged | LBBB common | Nonspecific | Nonspecific | - |
| Hyperkalemia | Bradycardia | Progressive block | Flat/absent | Prolonged | Widens to sine wave | - | Peaked, tall, narrow | - |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 247
- Ganong's Review of Medical Physiology 26E, Chapter 29
- Braunwald's Heart Disease, 2-Volume Set
- Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.