

17821475221045070823753106471888.jpg
17821475413348563554933128169514.jpg
Give answer for psm exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have enough textbook content. Let me compile comprehensive answers for all 16 PSM exam topics.
PSM Exam - Complete Answers
(Source: Park's Textbook of Preventive & Social Medicine, unless noted)
1. Mission Indradhanush
- Launched: December 2014, by Ministry of Health & Family Welfare
- Symbolism: 7 colours of rainbow = 7 vaccines covered initially (BCG, OPV, DPT, Measles, Hepatitis B, DT, TT)
- Aim: Fully immunize 90% of children who are unvaccinated or partially vaccinated by 2020 (later pre-poned to 2018)
- Target beneficiaries: Children under 2 years and pregnant women
- 6 phases completed (April 2015 - Dec 2018), covering 681 districts; 3.39 crore children reached
- Led to 6.7% increase in full immunization coverage in one year (vs. 1% earlier)
- Intensified Mission Indradhanush (IMI): Launched October 2017; focused on 190 districts/urban areas in 24 states; targeted urban slums and areas with slowest progress
- IMI 2.0 and 3.0 were further phases focusing on districts with lowest coverage
- Vaccines now include: BCG, OPV, IPV, DPT, Hepatitis B, Hib, Measles-Rubella (MR), JE (in endemic areas), PCV (in selected states), Rotavirus
2. Essential Newborn Care (ENC)
Essential Newborn Care refers to a set of evidence-based interventions for all newborns at birth and in the first days of life:
At birth (immediate care):
- Warmth: Dry and warm the baby immediately; delay bath for at least 24 hours
- Cord care: Clean cut, tie, and keep cord dry (no application of harmful substances)
- Breathing: Stimulate by drying; only suction if airway blocked
- Initiation of breastfeeding within 1 hour of birth
- Eye care: Clean wipes from inner to outer canthus
After birth:
- Exclusive breastfeeding for 6 months
- Thermal protection - skin-to-skin contact (Kangaroo Mother Care for LBW)
- Vitamin K prophylaxis (to prevent hemorrhagic disease)
- Early identification of danger signs (jaundice, feeding difficulty, respiratory distress, infection signs)
- Immunization: BCG, OPV-0, Hepatitis B at birth
Key danger signs in newborn:
Not feeding well, convulsions, very fast breathing (>60/min), severe chest indrawing, fever (>37.5°C) or low temp (<35.5°C), umbilical infection signs
3. Janani Suraksha Yojana (JSY)
- Launched: 12th April 2005 (modified from National Maternity Benefit Scheme)
- Objective: Reduce maternal and neonatal mortality by encouraging institutional delivery, focusing on BPL families
Key Features:
- 100% centrally sponsored scheme under NHM
- Integrates cash assistance with institutional care (antenatal, delivery, post-partum)
- ASHA is the link worker in Low Performing States (LPS)
Cash Benefits (from 2012-13):
| State Type | Rural (Mother) | Rural (ASHA) | Urban (Mother) | Urban (ASHA) |
|---|---|---|---|---|
| LPS | Rs. 1400 | Rs. 600 | Rs. 1000 | Rs. 400 |
| HPS | Rs. 700 | Rs. 600 | Rs. 600 | Rs. 400 |
Low Performing States (LPS) - 10 states: UP, Uttarakhand, MP, Jharkhand, Bihar, Rajasthan, Chhattisgarh, Odisha, Assam, J&K
- In LPS: All women delivering in govt. health centres or accredited private institutions
- In HPS: Only BPL women + SC/ST women; limited to 2 live births
- ASHA package available in all LPS, NE states, and tribal districts of all states/UTs
4. Mamata Day (Mamata Diwas)
- Mamata Day (also called VHND - Village Health, Nutrition and Sanitation Day) is held once a month at the Anganwadi Centre
- A platform for provision of maternal and child health services at the village level
Services provided on Mamata Day:
- Antenatal check-up (ANC) of pregnant women
- Immunization of children and pregnant women
- Nutrition counselling and supplementation
- Registration of pregnancies
- Health education - breastfeeding, complementary feeding, sanitation, hygiene
- Growth monitoring of children (0-5 years)
- Distribution of IFA tablets, Calcium, albendazole
- Identification of high-risk pregnancies
- Referral services
Service providers involved:
- ANM (Auxiliary Nurse Midwife)
- AWW (Anganwadi Worker)
- ASHA
Beneficiaries:
- Pregnant women, lactating mothers, children under 5, adolescent girls
(Mamata is a scheme from Gujarat/Odisha context - also refers to Odisha's Mamata scheme providing cash assistance of Rs. 5000 to pregnant and lactating women)
5. HBNC - Role and Responsibility of ASHA
Home Based Newborn Care (HBNC) is aimed at improving newborn survival through home visits by ASHA.
Objectives of HBNC:
- Provide essential newborn care and prevent complications
- Early detection and special care of preterm/LBW babies
- Early identification of illness and referral
- Build mother's confidence and skills
ASHA's Responsibilities in HBNC:
- Mobilize all pregnant mothers for full ANC package
- Birth planning and birth preparedness with family
- Home visits providing:
- Weighing the newborn
- Measuring temperature
- Ensuring warmth
- Supporting exclusive breastfeeding (positioning and attachment)
- Promoting hand-washing
- Skin, cord, and eye care
- Counselling against unhealthy practices (early bathing, bottle feeding)
- Identifying signs of sepsis
- Assess high-risk babies (preterm/LBW): increase visits, monitor weight, support warmth and breastfeeding
- Detect sepsis signs, provide first-level care and refer
- Recognize postpartum maternal complications and refer
- Counsel couple for family planning
- Provide immediate newborn care for home deliveries
ASHA Visit Schedule (up to 42 days):
- Institutional delivery: 6 visits - Day 3, 7, 14, 21, 28, 42
- Home delivery: 7 visits - Day 1, 3, 7, 14, 21, 28, 42
ASHA Incentive: Rs. 250 per newborn visited up to 42 days
6. Rastriya Bal Swasthya Karyakram (RBSK)
- Launched: 2013 under NHM
- Aim: Child health screening and early intervention services from birth to 18 years
4 D's of RBSK (screening for):
- Defects at birth (30 conditions)
- Deficiencies (Vitamin A, Iron deficiency, iodine, etc.)
- Diseases (anemia, dental caries, rheumatic heart disease, reactive airway disease, otitis media)
- Development delays including disability (vision, hearing, neurodevelopmental)
Coverage:
- Children from 0-18 years (approx. 27 crore children)
- Covers government schools, anganwadi centres (AWCs)
Service delivery:
- Mobile Health Teams (MHTs): 2 AYUSH/MBBS doctors per team; 2 teams per block
- Each team covers 100 AWCs or 2-3 schools per day
- Screening twice a year in AWCs, once a year in government schools
Referral: Children needing treatment referred to District Early Intervention Centres (DEICs)
- DEICs provide: audiological assessment, corrective surgeries, hearing aids, spectacles, physio/occupational/speech therapy
7. Components of RMNCH+A
RMNCH+A = Reproductive, Maternal, Newborn, Child Health + Adolescent
Launched in 2013 as a strategic approach to address the major causes of mortality across life stages in a continuum of care.
Components:
| Component | Key Interventions |
|---|---|
| R - Reproductive Health | Family planning, infertility services, RTI/STI treatment, pre-conception care |
| M - Maternal Health | ANC (4 visits minimum), safe delivery (institutional), EmOC, JSY, JSSK, postnatal care |
| N - Newborn Health | HBNC, SNCU, Kangaroo Mother Care, ENC, IMNCI |
| C - Child Health | Immunization, IMNCI, RBSK, nutrition, ORS/Zinc for diarrhea |
| A - Adolescent Health | RKSK (Rashtriya Kishor Swasthya Karyakram), WIFS, school health, menstrual hygiene, ARSH clinics |
Key platforms: VHND (Mamata Day), AWCs, ANM/ASHA, PHC, CHC, DH
Special initiatives under RMNCH+A:
- JSSK (Janani Shishu Suraksha Karyakram) - free services for pregnant women
- MAA programme (breastfeeding promotion)
- Home Based Care for Young Child (HBYC)
- Facility-based Newborn Care (FBNC): NBSUs and SNCUs
8. Adolescent Schemes
A. RKSK - Rashtriya Kishor Swasthya Karyakram (2014):
- Target: 10-19 years (253 million adolescents)
- Focus areas: Nutrition, Sexual & Reproductive Health, Mental Health, Non-communicable diseases, Substance misuse, Violence/injury prevention
- Delivery: Peer-led education, Adolescent Friendly Health Clinics (AFHCs)
B. WIFS - Weekly Iron & Folic Acid Supplementation:
- School-going girls + out-of-school girls 10-19 years
- Weekly IFA (large blue tablet: 100mg elemental iron + 500mcg folic acid)
- Also includes biannual deworming (albendazole 400mg)
C. SABLA - Rajiv Gandhi Scheme for Empowerment of Adolescent Girls:
- Girls 11-18 years; 14-18 year group as primary beneficiary
- Nutrition supplementation, iron/folic acid, health check-up, guidance on family welfare and childcare
D. Kishori Shakti Yojana (KSY)
E. Menstrual Hygiene Scheme: Free/subsidized sanitary napkins to adolescent girls in rural areas
F. School Health Programme: Annual health check-ups in government schools
9. Health Programme for the Elderly (Geriatric Health)
National Programme for Health Care of the Elderly (NPHCE) - Launched 2010-11:
Aim: Provide dedicated, accessible healthcare services to elderly (60+ years)
Service tiers:
| Level | Services |
|---|---|
| Sub-centre/PHC | Screening, domiciliary visits, referral |
| CHC | Dedicated OPD, physiotherapy, dedicated beds |
| District Hospital | 10-bed geriatric ward, specialist care |
| Regional Geriatric Centres (Medical Colleges) | Teaching, training, tertiary care |
Key features:
- Weekly Geriatric OPDs at CHC level
- Free medicines, diagnostics for elderly
- Training of health staff in geriatric care
- Domiciliary care for bed-ridden elderly
- Rashtriya Vayoshri Yojana: Assistive devices (spectacles, hearing aids, wheelchairs, dentures) for BPL elderly
10. Prevention and Control of Mental Health Problems
National Mental Health Programme (NMHP) - Launched 1982:
Objectives:
- Prevention and treatment of mental and neurological disorders
- Rehabilitation of patients
- Prevention of associated disabilities
- Reduce stigma
District Mental Health Programme (DMHP):
- Started 1996; extended to all districts
- Services: Outpatient, inpatient, follow-up community care, day care, emergency, IEC
- Integration with general health services
Prevention strategies:
- Primary: Health promotion, reduce risk factors (substance abuse, stress, social isolation), school mental health programmes
- Secondary: Early detection, MHGAP (Mental Health Gap Action Programme by WHO), task-sharing with non-specialists
- Tertiary: Rehabilitation, occupational therapy, preventing relapse
MHGAP priority conditions: Depression, psychosis, bipolar disorder, epilepsy, substance use, suicide/self-harm, dementia, developmental disorders
National Tele Mental Health Programme: iCall, NIMHANS helplines; 1800 as national helpline
11. Mental Health Act (India - 2017)
Mental Healthcare Act, 2017 (replaced 1987 Act):
Key Provisions:
- Right to mental healthcare: Every person has right to access mental healthcare and treatment from government
- Advance Directive: Person with mental illness can specify how they want to be treated/not treated in future
- Nominated representative: Can appoint a person to make decisions on their behalf
- Prohibition of treatments: No ECT without consent (free and informed); no ECT for minors; no chaining
- Decriminalization of suicide: Attempt to suicide is not a criminal offense; presumed to be under stress
- Mental Health Review Boards (MHRB): Set up in each district to protect rights of mentally ill
- Supported admission: Replaces earlier "voluntary/involuntary" with more nuanced 3-category admission
- Insurance parity: Mental illness to be treated at par with physical illness for insurance
- Rights of persons with MI: Right to confidentiality, dignity, non-discrimination, free legal aid, right to complain
Central/State Mental Health Authority established for regulation.
(Mental Health Act 1987 - established Mental Health Authorities, regulated psychiatric hospitals, set up procedures for admission and discharge)
12. Definition of Outbreak
An outbreak is the occurrence of more cases of disease, injury, or other health condition than expected in a given area or among a specific group of persons during a particular period.
Types:
- Common source outbreak: All cases exposed to a single source
- Point source (single exposure event): Bell-shaped epidemic curve
- Continuous/intermittent source: Prolonged exposure
- Propagated outbreak: Person-to-person spread; gradually rising curve
- Mixed outbreak: Combination of both
Epidemic vs. Outbreak:
- Epidemic: Unusually large or unexpected increase in disease in a defined community/region
- Outbreak is often used interchangeably but may imply more localized/contained event
- Cluster: Aggregation of cases in a place/time, possibly more than expected
Investigation steps (outbreak investigation):
- Confirm the diagnosis
- Establish case definition
- Count cases (descriptive epidemiology - Person, Place, Time)
- Determine epidemic type
- Identify source and mode of transmission
- Control measures
- Report findings
13. Ayushman Bharat
Announced: February 2018 (Budget announcement); Full launch September 2018
Two components:
Component 1: Health and Wellness Centres (HWCs)
- 1.5 lakh centres by 2022 (Sub-Health Centres and PHCs upgraded)
- Provide Comprehensive Primary Health Care (CPHC)
- Services: Maternal & child health, communicable diseases, NCDs (diabetes, hypertension, 3 cancers - oral, breast, cervical), mental health, ENT, ophthalmology, oral health, geriatric, palliative, trauma
- Free essential drugs and diagnostics
- Headed by Community Health Officer (CHO) - BSc/GNM nurse or Ayurveda practitioner
- First HWC inaugurated: 14 April 2018, Bijapur, Chhattisgarh
Component 2: AB-PMJAY (Pradhan Mantri Jan Arogya Yojana)
- Coverage: Rs. 5 lakh per family per year for secondary and tertiary hospitalization
- Beneficiaries: 10.74 crore poor/vulnerable families (based on SECC data) = ~50 crore individuals
- Covers: pre- and post-hospitalization expenses, day-care surgeries, 1350+ medical packages
- Cashless, paperless: At empanelled public and private hospitals
- No cap on family size, no age restriction, pre-existing conditions covered from day 1
- Not covered: OPD, fertility treatment, cosmetic surgeries, drug rehabilitation
14. Functions of Health and Wellness Centre (HWC)
HWCs are the revamped Sub-Health Centres and PHCs under Ayushman Bharat:
12 service packages provided:
- Pregnancy care and maternal health services
- Neonatal and infant health services
- Child health
- Adolescent health
- Family planning, contraceptive services and other reproductive health care
- Management of common communicable diseases (malaria, dengue, TB, leprosy)
- NCDs: Screening, prevention and management of - Hypertension, Diabetes, Oral/Breast/Cervical cancer
- Mental health (screening, basic management)
- ENT conditions
- Ophthalmology (screening for cataract, refractive errors)
- Oral health
- Geriatric and palliative care
Additional functions:
- Free essential drugs and diagnostics
- Health promotion and wellness activities: Yoga, nutrition counselling, lifestyle modification
- IEC and community outreach
- Teleconsultation support
- Team: CHO + Multi-purpose Workers (Male & Female) + ASHA
15. Health Problems of the Aged
Common health problems in elderly (60+ years):
Physical:
- Cardiovascular: Hypertension, coronary artery disease, heart failure
- Musculoskeletal: Osteoarthritis, osteoporosis, fractures (hip fracture most dangerous)
- Neurological: Parkinson's disease, stroke, peripheral neuropathy
- Cognitive: Dementia (Alzheimer's most common), delirium
- Sensory: Presbyopia, cataracts, glaucoma, presbycusis (hearing loss)
- Metabolic: Diabetes mellitus, hypothyroidism
- Cancer: Higher incidence in elderly
- Respiratory: COPD, pneumonia
- Urinary: Benign prostatic hyperplasia, urinary incontinence, UTIs
- GI: Constipation, malnutrition, malabsorption
Psychosocial:
- Depression (most common mental disorder in elderly)
- Anxiety disorders
- Social isolation, loneliness
- Elder abuse and neglect
- Retirement, bereavement
Geriatric Giants (classic 5 I's):
- Immobility
- Instability (falls)
- Incontinence
- Intellectual impairment (dementia/delirium)
- Iatrogenic illness (polypharmacy)
16. Mamata Divas - Service Providers, Beneficiaries, and Services
Mamata Divas (VHND - Village Health, Nutrition and Sanitation Day):
- Held once a month at every Anganwadi Centre
- A convergence platform of health, ICDS, and drinking water/sanitation departments
Service Providers:
- ANM (Auxiliary Nurse Midwife) - main health functionary
- ASHA - mobilizes beneficiaries, assists in services
- AWW (Anganwadi Worker) - arranges venue, maintains records
- Medical Officer - supervisory, for complicated cases
- AWH (Anganwadi Helper)
Beneficiaries:
- Pregnant women (all trimesters)
- Lactating mothers (upto 6 months of delivery)
- Children 0-5 years
- Adolescent girls (11-19 years)
- Women of reproductive age (15-49 years)
Services Available on Mamata Divas:
| Service | Details |
|---|---|
| ANC | BP, weight, hemoglobin, abdominal examination, TT vaccination |
| Immunization | BCG, OPV, DPT, Hep B, Measles/MR for children; TT for pregnant women |
| Nutrition | IFA tablets, Calcium supplementation, Vitamin A, zinc-ORS for diarrhea |
| Growth monitoring | Weight for age in children; MUAC measurement |
| Deworming | Albendazole for children and adolescents |
| Health education | Breastfeeding, complementary feeding, hygiene, family planning |
| PNC | Postnatal check-up, contraceptive counselling |
| Registration | Pregnant women, newborns, children |
| Referral | High-risk pregnancies, severely malnourished children |
| WIFS | Weekly IFA for adolescent girls (in schools and AWCs) |
Study Tips for PSM Exam:
- Questions 3 and 5 are marked "complete" in your list - focus revision on the others
- For MCQs: Remember key numbers - JSY cash amounts, RBSK 4D's, HBNC visit days (3,7,14,21,28,42), Ayushman Bharat Rs. 5 lakh coverage
- For SAQs: Use structured headings - Definition, Launch/Year, Objectives, Features, Beneficiaries, Service providers, Benefits
All answers sourced from Park's Textbook of Preventive and Social Medicine and supporting medical references. Best of luck for your exam!
Stages of disaster cycle and triage
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive textbook content on both topics. Here are the complete answers:
Stages of Disaster Cycle & Triage
(Sources: Park's Textbook of PSM; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine)
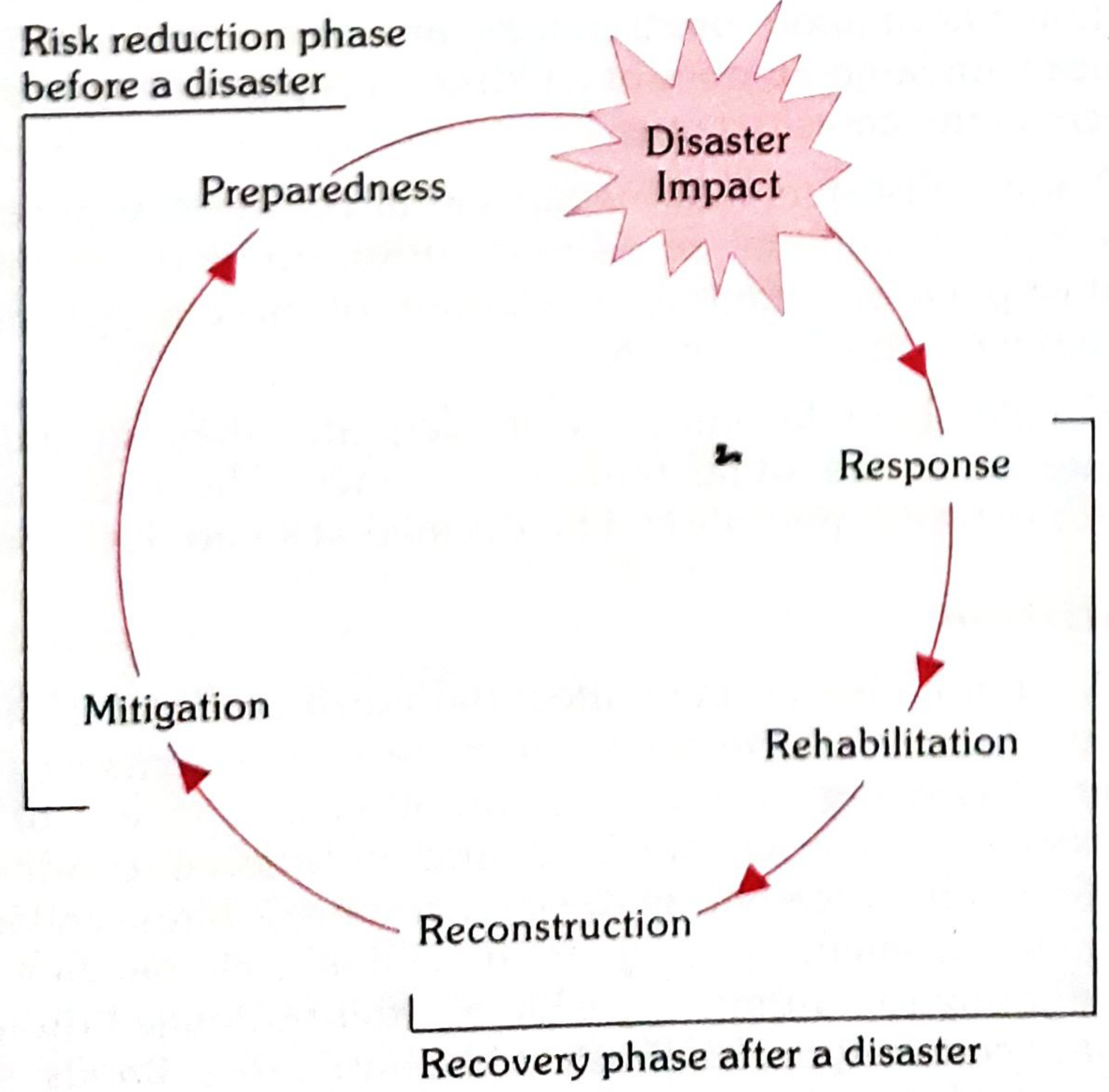
PART 1 - STAGES OF THE DISASTER CYCLE
The disaster cycle is the conceptual framework for understanding how disasters occur and are managed. It shows that disaster management is a continuous, cyclical process.
Three fundamental aspects of disaster management (Park's PSM):
- Disaster Response
- Disaster Preparedness
- Disaster Mitigation
These correspond to different phases of the disaster cycle. Rosen's Emergency Medicine describes four phases (standard WHO/UNISDR model):
The Disaster Cycle - 5 Stages
DISASTER IMPACT
↓
RESPONSE ← Recovery Phase (after disaster)
↓
REHABILITATION
↓
RECONSTRUCTION
↓
MITIGATION ← Risk Reduction Phase (before disaster)
↓
PREPAREDNESS
↓
DISASTER IMPACT (next cycle)
Stage-by-Stage Description
1. MITIGATION (Pre-disaster / Risk Reduction Phase)
- Activities to prevent or reduce the effects of a future disaster
- Undertaken during normal times, long before a disaster strikes
- Structural measures: Building earthquake-resistant structures, flood embankments, cyclone shelters, fire-proof construction
- Non-structural measures: Land-use planning, zoning laws, building codes, public education, vulnerability mapping
- Goal: Reduce hazard impact and community vulnerability
- Example: Constructing levees to prevent flood damage
2. PREPAREDNESS (Pre-disaster / Risk Reduction Phase)
- Activities taken in advance to build capacity to respond effectively
- Development of disaster plans (community/hospital emergency plans)
- Training of personnel (search & rescue teams, medical staff, NDRF)
- Stockpiling of emergency supplies (medicines, food, water, tents)
- Early warning systems (cyclone alerts, earthquake sensors)
- Mock drills and simulation exercises
- Establishing communication networks and evacuation routes
- India: National Disaster Management Authority (NDMA), SDMA, DDMA at state/district levels
- Goal: Maximize the ability to rescue lives and minimize damage when disaster strikes
3. RESPONSE (Immediate post-impact phase)
- Actions taken immediately after the disaster strikes
- Begins at time of impact and continues until the emergency is over
- Components:
- Search and Rescue (SAR) operations
- Evacuation of affected population
- First aid and emergency medical care
- Triage of mass casualties
- Emergency shelter, food, water supply
- Epidemiological surveillance
- Disease control (prevent post-disaster outbreaks)
- Activation of Emergency Operations Centre (EOC)
- Most injuries occur during impact; greatest need for emergency care is in the first few hours
- "Disaster Response" = immediate life-saving actions
4. REHABILITATION (Recovery Phase)
- Begins when the acute emergency is over; restoring basic services and normal life
- Temporary housing for displaced populations
- Restoration of health services (reopening of hospitals, PHCs)
- Psychosocial support and mental health services for affected population
- Restoration of water supply, sanitation, electricity, communication
- Resumption of livelihoods
- Surveillance for disease outbreaks continues
- Goal: Restore the affected community to pre-disaster functioning as quickly as possible
5. RECONSTRUCTION (Recovery Phase)
- Long-term rebuilding - permanent restoration of physical infrastructure
- Rebuilding homes, schools, hospitals, roads, bridges
- Economic recovery and restoration of livelihoods
- Incorporation of disaster risk reduction measures ("Build Back Better")
- Policy review and strengthening of future preparedness
- Can last months to years
- Goal: Restore or improve on pre-disaster conditions with added resilience
The Two Broad Phases
| Phase | Stages Included | Timing |
|---|---|---|
| Risk Reduction Phase | Mitigation + Preparedness | Before disaster |
| Recovery Phase | Response + Rehabilitation + Reconstruction | After disaster |
Important Points (MCQ-worthy)
- The disaster cycle is continuous - each disaster feeds into the next cycle
- UNISDR definition: Disaster risk management = systematic process using administrative decisions, operational skills, and policies to lessen impacts of natural hazards
- NDMA (National Disaster Management Authority) - set up under Disaster Management Act 2005 in India; chaired by Prime Minister
- NDRF (National Disaster Response Force) - dedicated force for specialized response
- The Sendai Framework (2015-2030): Global framework for disaster risk reduction
- Disasters most likely to need medical mass-casualty management: earthquakes, building collapse, industrial accidents, terrorist attacks, cyclones
PART 2 - TRIAGE
Definition
The word triage comes from the French verb trier = "to sort."
Triage is the process of rapidly classifying injured patients on the basis of the severity of their injuries and the likelihood of survival with prompt medical intervention, so as to provide maximum benefit to the greatest number in a disaster situation.
"The principle of first come, first treated is NOT followed in mass emergencies." - Park's PSM
Purpose / Goals
| Routine (ED) | Disaster/Mass Casualty |
|---|---|
| Identify most seriously ill for rapid care | Do the most good for the most people |
| Individual patient focus | Entire affected population focus |
| Time-dependent care | Resource-constrained care |
- In disaster triage: CPR is generally NOT performed (limited resources, poor outcomes at population level)
- Moribund patients requiring excessive resources with questionable benefit receive lowest priority
Triage Classification - Colour Code System (Internationally Accepted)
| Colour | Priority | Category | Description |
|---|---|---|---|
| 🔴 RED | 1st - Immediate | Life-threatening | Life-threatening shock or hypoxia is present or imminent; can be stabilized and will likely survive with immediate care. Needs treatment within minutes |
| 🟡 YELLOW | 2nd - Delayed/Urgent | Serious | Systemic injuries present but not yet in life-threatening shock/hypoxia; can wait 45-60 minutes without immediate risk. Needs care but can be deferred briefly |
| 🟢 GREEN | 3rd - Minor/Non-urgent | Minor/"Walking wounded" | Localized injuries without systemic implications; unlikely to deteriorate for several hours. Can wait |
| ⚫ BLACK | Last / Dead | Expectant/Dead | Dead or moribund - no spontaneous ventilation or circulation. Catastrophically injured with minimal survival chance regardless of care. Goal = comfort care/pain control only |
START Triage (Simple Triage and Rapid Treatment)
Most widely used pre-hospital triage system.
Mnemonic: RPM = Respirations, Perfusion, Mental status
Steps:
- Ask all patients who can walk to move aside → these are GREEN ("walking wounded")
- For remaining patients, assess in seconds:
- Respirations - present? rate? (>30/min = RED)
- Perfusion - capillary refill <2 sec or radial pulse present?
- Mental status - can follow simple commands?
- Only interventions at triage: open airway and control external hemorrhage
For children: JumpSTART (modification of START) - includes 5 rescue ventilations for apneic children.
Triage Levels - Where It Happens
- Field/Scene triage - at the disaster site; determines transport priority
- Transport triage - determines destination hospital
- Hospital triage - at ED entrance; reassesses and re-triages on arrival (triage is dynamic, must be repeated)
Triage Tagging
All patients receive a tag (coloured band/disaster tag) stating:
- Name, age, place of origin
- Triage category (colour)
- Diagnosis
- Initial treatment given
- Triage number (bar-coded in modern systems)
Mass Casualty Incident (MCI) Management Steps
- Triage - sort all casualties by priority
- Treatment - stabilize at scene/field hospital (life-saving procedures only)
- Transport - evacuate in priority order; RED patients leave first
- Transfer - to definitive care hospitals
Key Exam Points - Triage
| Point | Fact |
|---|---|
| Origin of word | French "trier" = to sort |
| Principle in disaster | Maximum benefit to maximum number |
| First priority colour | Red |
| Walking wounded colour | Green |
| Dead/moribund colour | Black |
| "Expectant" = | Black tag (burns >95% BSA, cardiac arrest in MCI) |
| CPR in mass casualty | Generally NOT performed |
| Field triage intervention | Only open airway + control external hemorrhage |
| Most common triage system | START (Simple Triage and Rapid Treatment) |
| Paediatric triage | JumpSTART |
| Mnemonic for START | RPM (Respirations, Perfusion, Mental status) |
| Yellow tag can wait | 45-60 minutes |
| Triage is | Dynamic - must be repeated at each level |
Epidemiological Surveillance Post-Disaster (Bonus)
Post-disaster disease threats:
- Gastroenteritis (most common post-disaster disease)
- Acute respiratory infections
- Vector-borne diseases (malaria, dengue) - appear after 2-3 weeks
- Leptospirosis (after floods)
- Zoonoses (from displaced animals)
Mass vaccination after disasters: WHO does NOT recommend routine mass vaccination for typhoid or cholera. Tetanus booster only for wounded patients not vaccinated in last 5 years. Focus should be on safe water + proper excreta disposal.


17821480453659120426662880820479.jpg
17821480629887682929951744561323.jpg
Give full detailed explanation in easy way of each question for psm exam
These are the same 16 questions from your earlier list! I already have all the content from Park's Textbook. Let me now rewrite everything in a simple, easy-to-understand, story-style explanation perfect for exam revision.
PSM Exam - Full Easy Explanations 🏥
Q1. Mission Indradhanush
🌈 Think of it like this:
Imagine a child who never got vaccinated because the health worker missed their village, or the parents never came to the clinic. Mission Indradhanush was launched to find and vaccinate those left-behind children.
What is it?
- Launched by Ministry of Health & Family Welfare in December 2014
- Named after the rainbow (Indradhanush) because it covers 7+ vaccines - just like a rainbow has 7 colours
- Main Goal: Fully immunize 90% of children who are unvaccinated or partially vaccinated by 2020 (later changed to 2018)
Who is targeted?
- Children under 2 years of age
- Pregnant women
- Specifically those missed during routine immunization (UIP - Universal Immunization Programme)
Vaccines covered:
BCG, OPV, IPV, DPT, Hepatitis B, Hib, Measles-Rubella (MR), JE (in endemic areas), PCV, Rotavirus
Key Facts to Remember:
| Fact | Detail |
|---|---|
| Launched | December 2014 |
| Symbol | Rainbow = 7 original vaccines |
| Target | 90% full immunization coverage |
| Phases completed | 6 phases (April 2015 - Dec 2018) |
| Districts covered | 681 districts |
| Children reached | 3.39 crore |
| Coverage increase | 6.7% in one year (vs 1% earlier) |
| Intensified Mission Indradhanush (IMI) | Launched October 2017 |
| IMI focus | 190 districts in 24 states; urban slums |
Simple Memory Trick:
"Rainbow for babies" - 7 colours = 7 vaccines, find every child left behind!
Q2. Essential Newborn Care (ENC)
🍼 Think of it like this:
A baby is born. What are the first things you MUST do to keep that baby alive and healthy? That is ENC - a checklist of life-saving actions for every newborn.
Definition:
Essential Newborn Care = A set of simple, evidence-based actions given to every baby at birth and in the first few days of life to prevent death and illness.
At Birth - The "ABCDE" of ENC:
A - Airway & Breathing
- Dry the baby immediately with a clean cloth (stimulates breathing)
- If breathing, no suction needed
- If not breathing → clean mouth, nose gently
B - Body Temperature (Warmth)
- Keep baby warm - skin-to-skin contact with mother immediately
- Delay the first bath for at least 24 hours (early bathing = heat loss = danger!)
- Wrap baby, cover head
C - Cord Care
- Cut cord with sterile blade
- Tie properly
- Keep cord dry and clean - no paste, no dung, no oil!
D - Feeding
- Initiate breastfeeding within 1 hour of birth
- Give colostrum (first yellowish milk) - it is liquid gold! Full of antibodies
E - Eye Care
- Clean eyes with clean cloth, wiping from inner to outer corner
After Birth:
- Exclusive breastfeeding for 6 months
- Vitamin K injection at birth (prevents bleeding in newborn)
- Immunization: BCG + OPV-0 + Hepatitis B at birth
- Kangaroo Mother Care (KMC) for low birth weight babies
Danger Signs in Newborn (MUST KNOW):
- Not feeding well
- Convulsions
- Fast breathing (>60/min)
- Very high or very low temperature
- Yellow skin (jaundice) spreading to palms and soles
- Pus from umbilicus or eyes
Easy Way to Remember:
"WARM + FEED + CLEAN" = the three pillars of essential newborn care
Q3. Janani Suraksha Yojana (JSY)
👩🍼 Think of it like this:
A poor pregnant woman in a village is afraid to go to a hospital because she cannot afford it. JSY says: "Come to the hospital, and we will pay YOU cash!" It is a cash-for-delivery scheme.
What is it?
- Full form: Janani = Mother, Suraksha = Protection, Yojana = Scheme
- Launched: 12th April 2005 under NHM
- Modified from the old "National Maternity Benefit Scheme"
- 100% Centrally Sponsored Scheme
Goal:
Reduce Maternal Mortality (MMR) and Neonatal Mortality (NMR) by encouraging institutional delivery (hospital birth instead of home birth)
Two Types of States:
LPS = Low Performing States (10 states) = States with LOW institutional delivery rate
UP, Uttarakhand, MP, Jharkhand, Bihar, Rajasthan, Chhattisgarh, Odisha, Assam, J&K
HPS = High Performing States = All remaining states
Cash Benefits (from 2012-13):
| Category | Rural - Mother | Rural - ASHA | Urban - Mother | Urban - ASHA |
|---|---|---|---|---|
| LPS | Rs. 1400 | Rs. 600 | Rs. 1000 | Rs. 400 |
| HPS | Rs. 700 | Rs. 600 | Rs. 600 | Rs. 400 |
Who gets the benefit?
- LPS: ALL women delivering in government health centres
- HPS: Only BPL women + SC/ST women; limited to 2 live births only
Role of ASHA in JSY:
- ASHA is the link worker between poor pregnant woman and health institution
- She escorts the woman to hospital
- She is responsible for ANC, postnatal care follow-up
- She gets her own cash incentive (Rs. 600 rural / Rs. 400 urban in LPS)
Memory Trick:
"LPS = More money, more eligibility" | HPS = Less money, BPL only" Remember the 10 LPS states as: "UU MP JB RC OA J" (UP, Uttarakhand, MP, Jharkhand, Bihar, Rajasthan, Chhattisgarh, Odisha, Assam, J&K)
Q4. Mamata Day (Mamata Divas / VHND)
📅 Think of it like this:
Once every month, your local Anganwadi centre becomes a mini health camp for mothers and children in the village. That day is called Mamata Day (or VHND).
Full Form:
VHND = Village Health, Nutrition and Sanitation Day
When & Where?
- Held once a month
- At every Anganwadi Centre (AWC)
The 3 People Who Run It:
- ANM (Auxiliary Nurse Midwife) - provides health services
- ASHA - mobilizes people to attend, assists
- AWW (Anganwadi Worker) - organizes the venue, maintains records
Who Comes (Beneficiaries)?
- Pregnant women
- Lactating mothers (up to 6 months after delivery)
- Children under 5 years
- Adolescent girls (11-19 years)
- Women of reproductive age (15-49 years)
What Services Are Provided?
| Service | What Happens |
|---|---|
| ANC Check-up | BP, weight, Hb check; TT injection for pregnant women |
| Immunization | BCG, OPV, DPT, Hepatitis B, MR for children |
| Nutrition | IFA tablets, Calcium, Vitamin A, Zinc-ORS distribution |
| Growth monitoring | Children weighed, MUAC measured |
| Deworming | Albendazole for children and adolescent girls |
| Health education | Breastfeeding, hygiene, family planning counselling |
| Postnatal care | PNC check-up, contraceptive advice |
| Registration | New pregnancies and newborns registered |
| Referral | High-risk cases sent to higher facility |
| WIFS | Weekly IFA tablet for adolescent girls |
Simple Summary:
"Mamata Day = Monthly health mela at Anganwadi = ANM + ASHA + AWW serve pregnant women + children + adolescent girls"
Q5. HBNC - Role & Responsibility of ASHA
🏠 Think of it like this:
After a baby is born (especially at home or after hospital discharge), the ASHA worker visits the house multiple times in the first 42 days. She checks on the baby, teaches the mother, and catches any problem early. This is HBNC.
Full Form:
HBNC = Home Based Newborn Care
Why is HBNC needed?
Many babies die at home in the first weeks of life due to:
- Infection (sepsis)
- Low birth weight complications
- Poor breastfeeding
- Hypothermia
ASHA visits the home to prevent, detect, and refer these problems.
ASHA's Main Responsibilities in HBNC:
During pregnancy:
- Ensure the mother gets full ANC (4 visits minimum)
- Help with birth planning (where to deliver, transport, money)
After delivery - during home visits, ASHA will:
- Weigh the baby - to detect Low Birth Weight (LBW)
- Check temperature - to detect hypothermia or fever
- Ensure warmth - advise skin-to-skin / proper wrapping
- Support breastfeeding - teach correct positioning and attachment
- Promote hand-washing - before touching baby
- Cord, skin and eye care - teach clean and dry cord care
- Counsel against bad practices - no early bathing, no bottle feeding
- Identify sepsis - check for pus, redness, fever, not feeding
- Manage LBW/preterm babies - increase visits, support warmth + feeding
- Detect maternal complications - bleeding, fever in mother
- Family planning counselling - for the couple
- Home deliveries - provide immediate newborn care if birth happened at home
ASHA's Visit Schedule (Up to 42 days):
| Delivery Type | Number of Visits | Days |
|---|---|---|
| Institutional delivery | 6 visits | Day 3, 7, 14, 21, 28, 42 |
| Home delivery | 7 visits | Day 1, 3, 7, 14, 21, 28, 42 |
(Extra Day 1 visit for home delivery because risk is higher)
ASHA's Incentive:
Rs. 250 per newborn for completing all visits up to 42 days
Memory Trick:
"ASHA visits 6 times for hospital baby (Day 3 onwards), 7 times for home baby (from Day 1)" ASHA = Antenatal prep + Support breastfeeding + Home visits + Alert for danger signs
Q6. Rastriya Bal Swasthya Karyakram (RBSK)
👶 Think of it like this:
The government sends a doctor team to every school and anganwadi to screen all children from birth to age 18 for diseases, defects, and delays - completely FREE. If something is found, the child gets free treatment. This is RBSK.
Full Form:
Rastriya = National | Bal = Child | Swasthya = Health | Karyakram = Programme
Launched: 2013, under NHM
Target:
Children aged 0 to 18 years - approximately 27 crore children in India
The 4 D's of RBSK (Most Important!):
| D | Meaning | Examples |
|---|---|---|
| D1 - Defects at Birth | Congenital conditions present at birth | Cleft lip/palate, club foot, Down syndrome, congenital heart disease, neural tube defects (30 conditions) |
| D2 - Deficiencies | Nutritional deficiencies | Anaemia (iron), Vitamin A deficiency, iodine deficiency, stunting, wasting |
| D3 - Diseases | Common childhood diseases | Dental caries, rheumatic heart disease, reactive airway disease, skin conditions, otitis media |
| D4 - Developmental Delays | Delays in growth, learning, senses | Vision problems, hearing loss, speech delay, autism, learning disabilities, cerebral palsy |
How is it Delivered?
Mobile Health Teams (MHTs):
- 2 teams per block
- Each team has 2 doctors (AYUSH or MBBS)
- Plus paramedics and support staff
Screening schedule:
- AWCs (Anganwadi Centres): Twice a year
- Government Schools: Once a year
Referral System:
Children with problems → referred to DEIC (District Early Intervention Centre)
What does DEIC provide?
- Audiological assessment (hearing tests)
- Corrective surgeries (for cleft lip, club foot, etc.) - FREE
- Hearing aids - FREE
- Spectacles - FREE
- Physiotherapy, Occupational therapy, Speech therapy
Memory Trick:
"RBSK = 4D programme: Defects, Deficiencies, Diseases, Delays → 0-18 years → MHT teams → DEIC for treatment"
Q7. Components of RMNCH+A
🔗 Think of it like this:
RMNCH+A is like a chain of care that follows a person through life stages - from before birth, through childhood, and into adolescence. No link in the chain should be broken.
Full Form:
Reproductive + Maternal + Newborn + Child Health + Adolescent
Launched: 2013, Strategic approach under NHM
The 5 Links of the Chain:
R - Reproductive Health
- Family planning services (spacing, limiting births)
- Treatment of RTI/STI (Reproductive Tract Infections, Sexually Transmitted Infections)
- Pre-conception care
- Infertility services
M - Maternal Health
- Antenatal Care: Minimum 4 ANC visits (now 8 recommended by WHO)
- TT vaccination in pregnancy
- IFA (Iron Folic Acid) tablets
- JSY & JSSK (free services at government hospitals)
- Safe/Institutional delivery
- Emergency Obstetric Care (EmOC)
- Postnatal care
N - Newborn Health
- HBNC (Home Based Newborn Care by ASHA)
- ENC (Essential Newborn Care at birth)
- SNCU (Special Newborn Care Unit at district hospitals)
- Kangaroo Mother Care (KMC) for LBW babies
- IMNCI (Integrated Management of Neonatal and Childhood Illness)
C - Child Health
- Universal Immunization Programme (UIP)
- RBSK (child health screening)
- Nutrition - ICDS, MAM/SAM management
- ORS + Zinc for diarrhoea
- IMNCI for sick children
- Vitamin A supplementation
A - Adolescent Health
- RKSK (Rashtriya Kishor Swasthya Karyakram) - for 10-19 years
- WIFS (Weekly Iron & Folic Acid Supplementation)
- School health programme
- Menstrual hygiene
- ARSH (Adolescent Reproductive and Sexual Health) clinics
The Service Delivery Platform:
Mamata Day (VHND) → ANM/ASHA/AWW → Sub-centre → PHC → CHC → District Hospital → Medical College
Memory Trick:
"R-M-N-C-A = Reproduction-Mother-Newborn-Child-Adolescent = Life stages from womb to youth"
Q8. Adolescent Schemes
🧒 Think of it like this:
Adolescents (10-19 years) have unique health needs - they are not children, not adults. India has multiple government schemes targeting their health, nutrition, and empowerment.
India has 253 million adolescents - the world's largest!
Key Schemes:
A. RKSK - Rashtriya Kishor Swasthya Karyakram (2014)
- Meaning: National Adolescent Health Programme
- Target: 10-19 years
- 6 Focus Areas:
- Nutrition
- Sexual & Reproductive Health
- Mental Health
- Non-Communicable Diseases prevention
- Substance abuse prevention
- Violence/injury prevention
- Services through: Adolescent Friendly Health Clinics (AFHCs), peer educators
B. WIFS - Weekly Iron & Folic Acid Supplementation
- Target: Girls AND boys 10-19 years (school-going + out-of-school)
- Large blue tablet given once a week:
- 100 mg elemental iron + 500 mcg folic acid
- Also: Biannual deworming (Albendazole 400 mg twice a year)
- Day: Given on fixed day every week (usually Monday)
- Goal: Prevent anaemia in adolescents
C. SABLA - Rajiv Gandhi Scheme for Empowerment of Adolescent Girls
- Target: Girls 11-18 years (primary focus: 14-18 years)
- Provides: Nutritional supplementation, health check-up, IFA, life skills education, guidance on family welfare
- Runs through AWCs
D. Kishori Shakti Yojana (KSY)
- Earlier scheme for adolescent girl empowerment (now merged into SABLA/RKSK)
E. Menstrual Hygiene Scheme
- Free/subsidized sanitary napkins to rural adolescent girls
- Under RKSK
F. School Health Programme
- Annual health check-ups in government schools
- Links with RBSK teams
Memory Table:
| Scheme | Age Group | Key Feature |
|---|---|---|
| RKSK | 10-19 | 6 focus areas, AFHCs |
| WIFS | 10-19 | Weekly IFA + deworming |
| SABLA | 11-18 | Nutrition + empowerment |
| School Health | School age | Annual check-up |
Q9. Health Programme for the Elderly
👴 Think of it like this:
Old people (60+) have multiple health problems but often cannot travel far for treatment. The government created NPHCE to bring special healthcare to their doorstep.
NPHCE = National Programme for Health Care of the Elderly
- Launched: 2010-11
- Target: People 60 years and above
- India's elderly population is rapidly increasing
Health Services at Different Levels:
| Level | Services |
|---|---|
| Sub-Centre / PHC | Screening for chronic diseases (BP, diabetes, cancer), domiciliary visits, home care for bedridden elderly, referral |
| CHC (Community Health Centre) | Weekly Geriatric OPD, physiotherapy, dedicated beds for elderly |
| District Hospital | 10-bed dedicated Geriatric Ward, specialist care, rehabilitation |
| Regional Geriatric Centre (Medical Colleges) | Super-specialist care, teaching, training of staff |
Key Features:
- Free medicines and diagnostics for elderly
- Domiciliary care - home visits for those who cannot come to clinic
- Training of health staff in geriatric care
- Physiotherapy and rehabilitation services
Rashtriya Vayoshri Yojana (RVY):
- Free assistive devices for BPL elderly:
- Spectacles (for vision)
- Hearing aids (for hearing loss)
- Wheelchairs / walking sticks (for mobility)
- Dentures (for teeth)
Memory Trick:
"NPHCE = Elderly health from PHC to medical college; RVY = Free devices for poor elderly"
Q10. Prevention & Control of Mental Health Problems
🧠 Think of it like this:
Mental health problems are very common but often ignored. India has the NMHP which works to prevent mental illness, treat it early, and rehabilitate patients.
NMHP = National Mental Health Programme
- Launched: 1982 (one of the oldest health programmes)
- One of the first countries in the developing world to have such a programme
Objectives (4):
- Prevention and treatment of mental and neurological disorders
- Rehabilitation of affected patients
- Prevention of disability associated with mental illness
- Reduce stigma associated with mental illness
The 3 Levels of Prevention:
Primary Prevention (Stop it before it happens):
- Health promotion and education
- Reduce risk factors: substance abuse, stress, social isolation
- School mental health programmes
- Strengthen community support systems
Secondary Prevention (Catch it early):
- Early detection and treatment
- MHGAP (WHO's Mental Health Gap Action Programme) - train non-specialist health workers to identify and manage mental illness at primary level
- Task-sharing - ANM, ASHA, community health workers trained to screen
Tertiary Prevention (Prevent worsening):
- Rehabilitation centres
- Occupational therapy
- Prevent relapse with long-term medication
- Community support groups
MHGAP Priority Conditions (8):
Depression, Psychosis, Bipolar disorder, Epilepsy, Substance use disorders, Suicide/Self-harm, Dementia, Developmental disorders (autism, ADHD)
DMHP = District Mental Health Programme:
- Started 1996, now extended to all districts
- Services: OPD, inpatient, day care, follow-up, emergency, community outreach, IEC
Helplines:
- iCall, NIMHANS helplines for mental health support
- National Tele Mental Health Programme (Tele-MANAS) - 14416
Memory Trick:
"NMHP 1982 = Prevent + Treat + Rehab + De-stigmatize = MHGAP for early detection = DMHP in every district"
Q11. Mental Health Act
⚖️ Think of it like this:
For a long time, mentally ill people had no rights - they could be admitted against their will, given shock treatment without consent, even chained. The Mental Healthcare Act 2017 changed all that - it gave rights to the mentally ill.
Two Important Acts:
A. Mental Health Act, 1987 (Old Act):
- Established Mental Health Authorities (Central and State)
- Set up procedures for admission and discharge
- Regulated psychiatric hospitals
- But was criticized for not protecting patient rights enough
B. Mental Healthcare Act, 2017 (New Act - Currently in Force):
Key Provisions (Easy to Remember):
1. Right to Mental Healthcare:
- Every person has the RIGHT to access mental healthcare from the government
- Government is responsible to provide this
2. Advance Directive:
- A person with mental illness can write instructions in advance about how they want to be treated (or NOT treated) in the future, when they cannot make decisions themselves
- Like a mental health "will"
3. Nominated Representative:
- Person can appoint someone (family member, friend) to make decisions on their behalf when they are incapacitated
4. Decriminalization of Suicide:
- Attempt to suicide is NO LONGER a crime
- Person who attempts suicide is presumed to be under severe stress
- They need care, not punishment
5. No ECT without consent:
- ECT (Electroconvulsive Therapy / shock treatment) without consent is BANNED
- ECT for minors (children) is COMPLETELY BANNED
- Must have free and informed consent of patient
6. No Chaining:
- Chaining of mentally ill persons is illegal and punishable
7. Mental Health Review Board (MHRB):
- Set up in every district
- Independent body to protect the rights of mentally ill patients
- Reviews cases of admission, discharge, rights violations
8. Insurance Parity:
- Mental illness must be treated at par with physical illness for insurance coverage
9. Rights of Persons with Mental Illness:
- Right to confidentiality
- Right to dignity
- Right to non-discrimination
- Right to free legal aid
- Right to complain against ill-treatment
Simple Summary Table:
| Feature | 1987 Act | 2017 Act |
|---|---|---|
| Suicide attempt | Criminal offence | Decriminalized |
| ECT without consent | Allowed | Banned |
| Advance Directive | Not present | Introduced |
| Patient rights | Limited | Comprehensive |
| MHRB | Not present | In every district |
| Insurance | Not mandated | At par with physical illness |
Memory Trick:
"2017 Act = Rights! No chains, no forced ECT, no punishment for suicide, insurance equality"
Q12. Define Outbreak
🦠 Think of it like this:
Normally 2 people in your village get diarrhoea per month. Suddenly 20 people get it in one week. That is MORE THAN EXPECTED. That is an outbreak.
Definition (WHO):
An outbreak is the occurrence of more cases of disease, injury, or other health condition than expected in a given area, among a specific group of persons, during a particular period.
Simple Formula:
Observed cases > Expected cases = Outbreak
Outbreak vs Epidemic vs Pandemic:
| Term | Meaning |
|---|---|
| Outbreak | More cases than expected; usually localized to a specific area or group |
| Epidemic | Large-scale outbreak affecting many people in a region/country |
| Pandemic | Epidemic that spreads across multiple countries/worldwide |
| Endemic | Disease constantly present at low, predictable levels in an area |
| Cluster | Aggregation of cases in a place/time, possibly more than expected |
Types of Outbreaks:
1. Common Source Outbreak:
- All cases exposed to ONE source (e.g., contaminated water supply)
- Two types:
- Point source: Single, brief exposure (e.g., wedding food poisoning) → Sharp bell-shaped curve
- Continuous source: Ongoing exposure (e.g., contaminated well over weeks)
2. Propagated Outbreak:
- Spread from person to person (e.g., measles, COVID)
- Epidemic curve rises gradually, wave-like pattern
3. Mixed Outbreak:
- Starts as common source, then spreads person-to-person
Steps of Outbreak Investigation (9 Steps):
- Confirm the diagnosis
- Confirm the outbreak exists
- Define and identify cases (case definition)
- Describe data by Person, Place, Time (Descriptive epidemiology)
- Develop hypotheses (what is the source/cause?)
- Test hypotheses (analytical study)
- Implement control measures
- Evaluate control measures
- Communicate findings (report)
Memory Trick:
"Outbreak = MORE than expected cases. Point source = one exposure = bell curve. Propagated = person to person = wave curve"
Q13. Ayushman Bharat
💊 Think of it like this:
Ayushman Bharat has 2 parts:
- At the village level - upgrade health centres to provide more services (HWC)
- At the hospital level - give Rs. 5 lakh insurance to poor families (PMJAY)
Announced: February 2018 (Union Budget); Full launch September 2018
Component 1: Health and Wellness Centres (HWC)
- 1.5 lakh Sub-Health Centres and PHCs upgraded to HWCs by 2022
- Bring comprehensive primary health care close to home
- First HWC launched: 14 April 2018, Bijapur, Chhattisgarh
- Services: Maternal/child health, NCDs (diabetes, hypertension, cancers), mental health, ENT, eye, oral health, geriatric care
- Free essential drugs + diagnostics
- Headed by CHO (Community Health Officer) - BSc/GNM nurse or Ayurveda practitioner
- Team: CHO + Male MPW + Female MPW (ANM) + ASHA
Component 2: AB-PMJAY (Pradhan Mantri Jan Arogya Yojana)
| Feature | Detail |
|---|---|
| Coverage amount | Rs. 5 lakh per family per year |
| Beneficiaries | 10.74 crore poor families (~50 crore individuals) |
| How identified | Based on SECC (Socio-Economic Caste Census) data |
| Hospitals | Empanelled public AND private hospitals |
| Type | Cashless and paperless |
| Pre-existing diseases | Covered from day one |
| Family size | No cap on family size |
| Age limit | No age restriction |
| Packages | 1350+ medical and surgical packages |
What is NOT covered:
- OPD (outpatient) visits
- Cosmetic surgeries
- Fertility/IVF treatment
- Drug rehabilitation
- Self-inflicted injuries
Memory Trick:
"Ayushman Bharat = HWC (village level) + PMJAY (hospital level, Rs 5 lakh, 10.74 crore families)"
Q14. Functions of Health & Wellness Centre (HWC)
🏥 Think of it like this:
The old sub-centre or PHC only handled basic maternal and child health. The new HWC does 12 full service packages - it is like a small polyclinic for the whole community.
12 Service Packages (MUST MEMORIZE):
| # | Service Package |
|---|---|
| 1 | Pregnancy care and maternal health |
| 2 | Neonatal and infant health |
| 3 | Child health |
| 4 | Adolescent health |
| 5 | Family planning and reproductive health |
| 6 | Communicable diseases (TB, malaria, dengue, leprosy) |
| 7 | NCDs - screening and management of Hypertension, Diabetes, Oral cancer, Breast cancer, Cervical cancer |
| 8 | Mental health - basic screening and management |
| 9 | ENT conditions |
| 10 | Eye care (cataract screening, refractive errors) |
| 11 | Oral health |
| 12 | Geriatric and palliative care |
Additional Functions:
- Free essential drugs and diagnostics
- Teleconsultation - connect with specialists via phone/video
- Health promotion: Yoga sessions, lifestyle modification counselling, nutrition education
- IEC activities (Information, Education, Communication)
- Community outreach
Staff at HWC:
- CHO (Community Health Officer) - team leader
- MPW Male (Health Worker Male)
- ANM (Female Multipurpose Worker)
- ASHA (Accredited Social Health Activist)
Key Difference - Old vs New:
| Old Sub-Centre / PHC | New HWC |
|---|---|
| Maternal & child health only | 12 service packages |
| No NCD screening | NCD screening included |
| No mental health | Mental health included |
| No teleconsultation | Teleconsultation available |
Memory Trick:
"HWC = 12 packages = Pregnancy + Newborn + Child + Adolescent + Reproductive + Communicable + NCD + Mental + ENT + Eye + Oral + Geriatric" Think of it as: Whole Life Healthcare under one roof
Q15. Health Problems of the Aged
👵 Think of it like this:
After age 60, the body starts wearing out. Multiple systems break down simultaneously. This is called multi-morbidity in the elderly.
The "5 I's" of Geriatric Problems (CLASSIC EXAM ANSWER!):
| I | Problem | Example |
|---|---|---|
| Immobility | Cannot move freely | Arthritis, stroke, Parkinson's |
| Instability | Falls | Hip fracture, balance problems |
| Incontinence | Loss of bladder/bowel control | Urinary incontinence, BPH in men |
| Intellectual impairment | Brain problems | Dementia, Alzheimer's, delirium |
| Iatrogenic illness | Problems caused by medicines | Polypharmacy, drug interactions |
System-wise Common Problems:
Heart & Blood Vessels:
- Hypertension (most common)
- Coronary Artery Disease (angina, heart attack)
- Heart failure, stroke
Bones & Joints:
- Osteoarthritis (joint pain, most common)
- Osteoporosis (brittle bones → hip fracture)
- Rheumatoid arthritis
Brain & Nerves:
- Dementia (Alzheimer's - most common type)
- Parkinson's disease
- Peripheral neuropathy
Senses:
- Vision: Cataracts, glaucoma, presbyopia (near vision loss)
- Hearing: Presbycusis (age-related hearing loss) - most common sensory problem
Endocrine:
- Diabetes mellitus (Type 2)
- Hypothyroidism
Lungs:
- COPD (Chronic Obstructive Pulmonary Disease)
- Pneumonia (can be fatal in elderly)
Urinary:
- BPH (Benign Prostatic Hyperplasia) in men - urinary difficulty
- UTI (Urinary Tract Infection) - common in women
- Urinary incontinence
Mental Health:
- Depression - MOST COMMON mental disorder in elderly
- Anxiety
- Social isolation and loneliness
Others:
- Cancer (incidence increases with age)
- Malnutrition
- Elder abuse (physical, financial, emotional)
- Polypharmacy (taking too many medicines)
Memory Trick:
"5 I's: Immobility, Instability, Incontinence, Intellectual impairment, Iatrogenic illness" Most common things to remember:
- Most common mental disorder = Depression
- Most common dementia = Alzheimer's
- Most common sensory problem = Presbycusis
- Most dangerous fracture = Hip fracture
Q16. Mamata Divas - Service Providers, Beneficiaries & Services
📋 Think of it like this:
This is basically an expanded version of Q4 (Mamata Day). Here the examiner specifically wants you to list service providers, beneficiaries, AND all services. Use the table format below in your exam!
What is Mamata Divas?
- Same as VHND = Village Health, Nutrition and Sanitation Day
- Held once a month at every Anganwadi Centre
- A convergence platform bringing health + nutrition + sanitation departments together at village level
SERVICE PROVIDERS (Who provides services?):
| Provider | Role |
|---|---|
| ANM (Auxiliary Nurse Midwife) | Main health provider; ANC, immunization, IUD, PNC |
| ASHA | Mobilizes beneficiaries to attend; assists ANM; home follow-up |
| AWW (Anganwadi Worker) | Organizes venue, maintains registers, weighs children |
| AWH (Anganwadi Helper) | Assists AWW; cleaning, arrangement |
| Medical Officer | Supervisory visits; manages complicated cases; quality check |
| CDPO / Supervisor | Monitoring and supervision visits |
BENEFICIARIES (Who receives services?):
| Beneficiary | Age Group |
|---|---|
| Pregnant women | All trimesters |
| Lactating mothers | Up to 6 months post-delivery |
| Children | 0 to 5 years |
| Adolescent girls | 11 to 19 years |
| Women of reproductive age | 15 to 49 years |
SERVICES AVAILABLE (Detailed List):
Maternal Health:
- ANC check-up: Blood pressure, weight, haemoglobin (Hb) testing
- Abdominal examination (fundal height, foetal heart rate)
- TT (Tetanus Toxoid) vaccination for pregnant women
- IFA (Iron Folic Acid) tablet distribution
- Calcium supplementation
- Registration of new pregnancies
- Identification and referral of high-risk pregnancies
Child Health:
- Immunization: BCG, OPV, DPT, Hepatitis B, MR (as per schedule)
- Growth monitoring: Weighing children; plotting on growth chart
- MUAC (Mid Upper Arm Circumference) to detect malnutrition
- Vitamin A supplementation (children 6 months - 5 years)
- ORS + Zinc for diarrhoea management
- Identification and referral of SAM/MAM (severely/moderately malnourished) children
Nutrition:
- Distribution of: IFA tablets, Calcium, Vitamin A, Albendazole
- Nutritional counselling to mothers
- Complementary feeding advice (from 6 months onwards)
Adolescent Health:
- WIFS - Weekly Iron & Folic Acid tablet given on fixed day
- Deworming - Albendazole 400 mg biannually
- Health education on menstrual hygiene, nutrition, reproductive health
Postnatal Care:
- Check-up of recently delivered mothers
- Counselling on exclusive breastfeeding
- Contraceptive counselling and provision (condoms, OCPs)
General:
- Health and hygiene education
- Sanitation promotion (handwashing, ODF - open defecation free)
- Referral for any sick patient to PHC/CHC
- Registration of newborns
Quick Exam Answer Format for Q16:
Mamata Divas = Monthly VHND at AWCProviders: ANM, ASHA, AWW (+ AWH, MO for supervision)Beneficiaries: Pregnant women, Lactating mothers, Children <5 years, Adolescent girls, Women 15-49 yearsServices: ANC + Immunization + Nutrition (IFA/Calcium/Vit A) + Growth monitoring + Deworming + WIFS + PNC + Health education + Referral
📌 Quick Revision - All 16 Topics at a Glance
| Q | Topic | One-Line Memory Hook |
|---|---|---|
| 1 | Mission Indradhanush | Rainbow vaccination = find left-behind children; Dec 2014; 90% coverage goal |
| 2 | Essential Newborn Care | WARM + FEED + CLEAN in first hours; delay bath 24 hrs; breastfeed in 1 hour |
| 3 | JSY | Cash for hospital delivery; LPS 10 states; rural LPS = Rs.1400 mother + Rs.600 ASHA |
| 4 | Mamata Day | Monthly VHND at AWC; ANM+ASHA+AWW; pregnant women + children + adolescents |
| 5 | HBNC-ASHA | 6 visits (hospital baby) or 7 visits (home baby) up to Day 42; Rs.250 incentive |
| 6 | RBSK | 4 D's: Defects + Deficiencies + Diseases + Delays; 0-18 yrs; MHT teams; DEIC |
| 7 | RMNCH+A | Reproductive+Maternal+Newborn+Child+Adolescent = chain of care |
| 8 | Adolescent Schemes | RKSK (10-19 yrs) + WIFS (weekly IFA) + SABLA (girls 11-18) |
| 9 | Elderly Programme | NPHCE 2010; 10-bed geriatric ward at DH; RVY = free devices for BPL elderly |
| 10 | Mental Health Prevention | NMHP 1982; DMHP in districts; MHGAP; Primary+Secondary+Tertiary prevention |
| 11 | Mental Health Act | 2017 Act: Suicide decriminalized; No forced ECT; MHRB in each district; patient rights |
| 12 | Outbreak | More cases than expected; Point source = bell curve; Propagated = wave curve |
| 13 | Ayushman Bharat | HWC (1.5 lakh) + PMJAY (Rs.5 lakh, 10.74 crore families, SECC-based) |
| 14 | HWC Functions | 12 service packages = pregnancy to geriatric; CHO leads the team |
| 15 | Elderly Health Problems | 5 I's: Immobility, Instability, Incontinence, Intellectual impairment, Iatrogenic |
| 16 | Mamata Divas | ANM+ASHA+AWW serve pregnant+lactating+children+adolescents at monthly AWC camp |
All the best for your PSM exam! 🎓
(Source: Park's Textbook of Preventive & Social Medicine)
Essential new born care for psm exam
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the textbook content needed. Here is the full, detailed, easy explanation:
🍼 Essential Newborn Care (ENC)
Complete PSM Exam Answer - Easy Explanation
(Source: Park's Textbook of Preventive & Social Medicine)
🎯 What is Essential Newborn Care?
Think of it this way: A baby is born. In the next few minutes, hours, and days - what MUST be done to keep it alive?
That exact checklist of life-saving actions = Essential Newborn Care (ENC)
Definition:
Essential Newborn Care is a set of simple, evidence-based interventions provided to every newborn at birth and in the first days/weeks of life to prevent death and disease.
Primary Goal:
Reduce perinatal and neonatal mortality
📊 Why is it Important? (Background)
- Neonatal period = First 28 days of life (most dangerous period for a child)
- Neonatal mortality rate (NMR) in India = about 23 per 1000 live births
- Most neonatal deaths occur in the first 7 days (early neonatal period)
- About 75% of all under-5 deaths occur in the first year of life
- Most of these deaths are preventable with simple, low-cost interventions
Main causes of neonatal death:
- Birth asphyxia (baby not breathing at birth)
- Infections/Sepsis
- Prematurity / Low Birth Weight (LBW)
- Hypothermia (getting too cold)
ENC directly addresses all 4 of these causes!
🔑 Main Components of ENC (Park's PSM)
Park's textbook lists 5 main components:
| # | Component | Problem it prevents |
|---|---|---|
| 1 | Resuscitation of newborn with asphyxia | Birth asphyxia deaths |
| 2 | Prevention of Hypothermia | Cold-related deaths |
| 3 | Prevention of Infection | Neonatal sepsis deaths |
| 4 | Exclusive Breastfeeding | Malnutrition + infection deaths |
| 5 | Referral of sick newborn | Deaths from unrecognized illness |
COMPONENT 1: Resuscitation of Newborn (Handling Birth Asphyxia)
🫁 What is birth asphyxia?
When a baby does not breathe on its own immediately after birth. This is an emergency - brain damage starts within minutes.
Steps at birth (FIRST 30 SECONDS):
Step 1: DRY the baby
- Immediately wipe the baby with a clean, dry cloth
- This dries the baby AND stimulates it to breathe (touch stimulates breathing reflex)
- Change wet cloth for a dry one immediately
Step 2: ASSESS breathing
- Is the baby crying? → Breathing well → Continue ENC
- Is the baby NOT crying / breathing weakly? → Start resuscitation
Step 3: CLEAR the airway (only if needed)
- Suction is needed ONLY if airway is blocked (meconium, blood, mucus)
- Routine suctioning is NOT recommended (it can cause harm)
- If suctioning needed: mouth first, then nose
Step 4: STIMULATE (if not breathing)
- Rub the back vigorously
- Flick the soles of the feet (gentle stimulation)
Step 5: Bag-Mask Ventilation (if still not breathing)
- If baby does not breathe after 30 seconds of stimulation
- Give positive pressure ventilation using bag and mask
- Rate: 40-60 breaths per minute
- Done at the Newborn Care Corner in the labour room
Newborn Care Corner:
Every delivery room should have a Newborn Care Corner with:
- Radiant warmer
- Resuscitation equipment (bag + mask in sizes for newborn)
- Suction device
- Oxygen
- Clock/timer
COMPONENT 2: Prevention of Hypothermia (Keeping Baby Warm)
🌡️ Why does the newborn get cold so easily?
- Baby comes out wet from amniotic fluid
- Huge surface area compared to body weight
- No shivering mechanism yet
- Cannot generate enough body heat on its own
- Normal baby temperature: 36.5°C - 37.5°C
- Hypothermia = body temperature below 36.5°C
The Warm Chain - 10 Steps:
1. Warm delivery room
- Room temperature should be at least 25°C
- No fans, no open windows near the delivery area
2. Warm resuscitation
- Resuscitation table should be warm (radiant warmer)
3. Immediate drying
- Dry the baby right away with warm, dry cloth
- Remove the wet cloth immediately
4. Skin-to-skin contact (SSC)
- Place baby on mother's bare chest, tummy-to-tummy
- Cover both mother and baby with a blanket
- This is the best way to keep baby warm - uses mother's body heat
5. Breastfeeding
- Breastfeeding provides warmth, nutrition, and closeness
6. Postpone bathing
- NEVER bathe the baby immediately after birth!
- Delay bath for at least 6 hours (ideally 24 hours)
- Early bathing is a traditional practice that kills babies by causing hypothermia
7. Appropriate clothing
- Dress baby in clean, warm clothes
- Always cover the head - newborns lose most heat through the head
8. Warm transportation
- If transferring baby, keep warm during transport (wrap well)
9. Warm procedures
- All procedures (injections, weighing) should be done in warm area
10. Training and awareness
- Teach mothers and family not to bathe baby early, not to put baby in cold room
For Low Birth Weight babies → Kangaroo Mother Care (KMC):
KMC = The best warmth solution for small babies!
Kangaroo Mother Care was introduced in Colombia in 1979 by Drs. Hector Martinez and Edzar Rey - because there were not enough incubators and babies were dying of infections in overcrowded hospitals.
4 Components of KMC:
- Skin-to-skin positioning - Baby placed on mother's chest in upright position (like a kangaroo's pouch!)
- Adequate nutrition - through breastfeeding or expressed breast milk
- Ambulatory care - mother carries baby, walks around, earlier discharge from hospital
- Support for the mother and family in caring for the baby
Benefits of KMC:
- Maintains normal body temperature (37°C) without incubator
- Promotes breastfeeding
- Reduces infections
- Better weight gain
- Reduces apnoea (breathing pauses)
- Improves mother-baby bonding
- Reduces hospital stay and cost
Who gets KMC?
- All Low Birth Weight babies (< 2500 g)
- All preterm babies
- Stable babies (not needing intensive care)
COMPONENT 3: Prevention of Infection
🦠 Why are newborns so prone to infection?
- Immune system not yet developed
- Any break in skin/cord can let bacteria in
- Sepsis (blood infection) kills within hours
Clean Delivery:
- Delivery on a clean surface
- Clean hands of delivery attendant (hand washing with soap)
- Clean cord cutting instrument (sterile blade/scissors)
- Clean cord tie (sterile thread/clamp)
- Nothing unclean applied to the cord
Cord Care:
The cord stump is the most common entry point for infection!
Do:
- Keep cord clean and DRY
- Keep cord exposed to air (fold nappy below cord level)
- If soiled, clean with clean water and dry thoroughly
Do NOT:
- Apply ghee, mustard oil, cow dung, ash, turmeric, or any substance to cord
- Bandage or cover the cord stump
- These traditional practices CAUSE infection (tetanus, omphalitis)
Signs of cord infection (Omphalitis):
- Redness around the cord base
- Pus or foul smell from cord
- Swelling → needs immediate referral
Eye Care:
- After birth, clean both eyes gently with a separate clean cloth for each eye
- Wipe from inner corner to outer corner (not the other way)
- Purpose: Remove blood and amniotic fluid, prevent conjunctivitis
Skin Care:
- Vernix caseosa (the white coating on baby) is PROTECTIVE - do not scrub it off
- Gentle cleaning only
- No powders, no oils on skin in first few days
Hand Hygiene:
- Anyone handling the baby must wash hands first
- This is the single most important infection prevention measure
Immunization at Birth:
| Vaccine | When | Purpose |
|---|---|---|
| BCG | At birth | Protect against tuberculosis |
| OPV-0 (Oral Polio Vaccine) | At birth (Zero dose) | Protect against polio |
| Hepatitis B | At birth (within 24 hours) | Protect against Hepatitis B (very important!) |
Vitamin K Injection:
- All newborns should receive Vitamin K 1 mg IM (into thigh muscle) at birth
- Why? Newborns have very little Vitamin K → risk of Haemorrhagic Disease of the Newborn (HDN) - serious internal bleeding
- Vitamin K is needed for blood clotting
COMPONENT 4: Exclusive Breastfeeding
🤱 What is the BEST food for a newborn?
Breast milk - and ONLY breast milk for the first 6 months!
Early Initiation of Breastfeeding:
- Start breastfeeding within 1 hour of birth - this is critical!
- Early suckling stimulates milk production
- Helps in uterine contraction (reduces maternal bleeding)
Colostrum - The First Milk (Liquid Gold!):
- Thick, yellowish first milk produced in first 3-5 days
- Rich in antibodies (IgA) - protects against infections
- Rich in protein, vitamins, minerals
- Acts as baby's first vaccine
- Traditional practice of throwing away colostrum is WRONG and HARMFUL
Exclusive Breastfeeding for 6 Months:
- No water, no other milk, no other food - ONLY breast milk for 6 months
- Even in hot weather, breast milk has enough water
Benefits of Breastfeeding:
For Baby:
- Complete nutrition (all proteins, fats, vitamins, minerals)
- Antibodies protect against diarrhoea, respiratory infections, otitis media
- Reduces risk of SIDS (Sudden Infant Death Syndrome)
- Better brain development
- Lower risk of obesity and diabetes later in life
For Mother:
- Reduces postpartum bleeding (oxytocin release)
- Natural contraception (LAM - Lactational Amenorrhoea Method)
- Faster return to pre-pregnancy weight
- Reduces risk of breast and ovarian cancer
- Strengthens mother-baby bond
For Country:
- Saves lives - reduces neonatal and infant mortality
- Saves money - no need to buy formula
Correct Breastfeeding Position (LATCH):
- Baby's whole body facing mother (tummy-to-tummy)
- Baby's mouth wide open
- More areola (dark area) in baby's mouth, not just nipple
- Baby's chin touching breast
- No pain for mother when positioned correctly
COMPONENT 5: Referral of Sick Newborn
🚨 Danger Signs - When to refer immediately:
These are called "DANGER SIGNS" in the newborn - if you see any of these, the baby must be referred to hospital IMMEDIATELY:
| # | Danger Sign | What it means |
|---|---|---|
| 1 | Not feeding at all or very poorly | Infection, neurological problem |
| 2 | Convulsions/fits | Brain problem, low blood sugar, infection |
| 3 | Fast breathing (>60 breaths/min) | Respiratory infection, heart problem |
| 4 | Severe chest indrawing | Serious respiratory distress |
| 5 | Fever (>37.5°C or feels hot to touch) | Infection/sepsis |
| 6 | Low temperature (<35.5°C or feels cold) | Hypothermia (especially dangerous in LBW babies) |
| 7 | Yellow skin (jaundice) spreading to palms and soles | Severe jaundice - can cause brain damage |
| 8 | Pus from eyes or umbilicus | Infection |
| 9 | Umbilical redness/swelling | Omphalitis |
| 10 | Baby is unconscious / very lethargic | Severe illness |
| 11 | Skin rash / blisters / pustules | Skin infection |
| 12 | Bleeding from any site | Haemorrhagic disease |
Referral Pathway:
Home → Sub-Centre/PHC → CHC/FRU → District Hospital (SNCU)
Newborn Care Facilities:
| Facility Level | Unit | Purpose |
|---|---|---|
| Labour Room | Newborn Care Corner (NBCC) | Immediate care at birth (ENC + resuscitation) |
| PHC / Sub-centre | NBSU (Newborn Stabilisation Unit) | Stabilize sick newborns before referral |
| District Hospital | SNCU (Special Newborn Care Unit) | Management of LBW, preterm, sick newborns |
| Medical College | NICU (Neonatal Intensive Care Unit) | Ventilation, surgery, intensive care |
📋 ENC at a Glance - Step by Step at Birth
IMMEDIATELY AT BIRTH (First 30 seconds):
Baby born
↓
DRY with warm cloth immediately
↓
Is baby crying/breathing?
↓ ↓
YES NO
↓ ↓
Continue ENC Stimulate (rub back, flick feet)
↓
Still not breathing?
↓
Bag-mask ventilation
(in Newborn Care Corner)
FIRST HOUR OF LIFE:
- ✅ Keep baby warm (skin-to-skin with mother)
- ✅ Initiate breastfeeding within 1 hour
- ✅ Vitamin K injection (1 mg IM)
- ✅ Eye care (clean eyes)
- ✅ BCG + OPV-0 + Hepatitis B vaccines
- ❌ Do NOT bathe baby yet
FIRST DAY:
- ✅ Continue skin-to-skin contact
- ✅ Continue exclusive breastfeeding on demand
- ✅ Cord care - keep dry and clean
- ✅ Watch for danger signs
- ✅ Assess for jaundice (yellowing of skin)
- ❌ Do NOT apply anything to the cord
AFTER DISCHARGE:
- ASHA visits home for HBNC (Day 3, 7, 14, 21, 28, 42)
- Mother counselled on:
- Exclusive breastfeeding
- Warmth
- Cord care
- Danger signs to watch for
- Next immunization visits
📝 Priority Areas to Improve Newborn Health (Park's PSM Summary Table)
| Time Period | Key Interventions |
|---|---|
| Before & during pregnancy | Delayed child-bearing, good nutrition, tetanus immunization, PMTCT of HIV |
| During pregnancy | ANC, treat anaemia/infections, monitor foetal well-being, birth preparedness |
| During & soon after delivery | Safe delivery, newborn resuscitation, warmth, cord/eye/skin care, early breastfeeding, early detection of complications |
| During first month of life | Postnatal contact (HBNC), exclusive breastfeeding, detect/manage illness, immunization |
🧠 EASY MEMORY TRICKS for Exam
The "5 C's" of ENC:
Clean birth → Clear airway → Cord care → Colostrum → Check for danger signs
Components in one line:
"RHI-BF-R" = Resuscitation + Hypothermia prevention + Infection prevention + Breastfeeding + Referral
For HBNC visit schedule:
"Hospital baby = 6 visits (Day 3 onwards)" "Home baby = 7 visits (Day 1 onwards)"
Key numbers to remember:
| What | Number |
|---|---|
| Start breastfeeding within | 1 hour of birth |
| Exclusive breastfeeding for | 6 months |
| Delay first bath until | 24 hours (minimum 6 hours) |
| Normal newborn temperature | 36.5 - 37.5°C |
| Fast breathing in newborn | >60 breaths/min |
| KMC for babies less than | 2000 g (LBW) |
| Vitamin K dose | 1 mg IM at birth |
| KMC introduced in Colombia | 1979 |
| Vaccines at birth | BCG + OPV-0 + Hepatitis B |
✍️ How to Write This in Exam (Structure)
For a 5 mark question:
- Definition + Goal (2 lines)
- Main Components (list the 5) - brief explanation of each
- Danger signs (list at least 5)
For a 10 mark question:
- Introduction + Definition + Goal + Why important (NMR data)
- All 5 Components with explanation
- Warm Chain (10 steps)
- KMC (4 components + benefits)
- Danger signs (table)
- Newborn care facilities (NBCC, NBSU, SNCU, NICU)
- Conclusion - role of HBNC + ASHA
Source: Park's Textbook of Preventive and Social Medicine
Best of luck for your PSM exam! 🎓
This is a shared conversation. Sign in to Orris to start your own chat.