Abg detail clinical analysis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from authoritative textbooks. Let me compile the full clinical analysis.
ABG (Arterial Blood Gas) - Detailed Clinical Analysis
What is an ABG?
An arterial blood gas is the gold standard for assessing a patient's respiratory and metabolic status. It directly measures:
| Parameter | Normal Value | Normal Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO2 | 40 mmHg | 35 - 45 mmHg |
| PaO2 | 100 mmHg | 75 - 100 mmHg |
| HCO3- (calculated) | 24 mEq/L | 22 - 26 mEq/L |
| Base Excess/Deficit | 0 | -4 to +4 |
HCO3- is not directly measured - it is calculated from the Henderson-Hasselbalch equation. Base excess is also a calculated value.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 974
- Current Surgical Therapy 14e, p. 1608
Physiologic Basis: The Henderson-Hasselbalch Equation
pH = pKa + log [HCO3-] / (0.03 × PaCO2)
Blood pH is determined by the ratio of HCO3- to CO2. Any change in either drives a change in pH. The buffer equation:
H2O + CO2 ↔ H2CO3 ↔ H+ + HCO3-
- Acidemia: pH < 7.35 (increased H+)
- Alkalemia: pH > 7.45 (decreased H+)
Two systems tightly regulate pH:
- Respiratory system - responds within minutes to hours (alveolar ventilation)
- Renal system - responds within hours to days (HCO3- reabsorption / H+ secretion)
Step-by-Step ABG Interpretation
Step 1: Evaluate pH
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
- pH 7.35 - 7.45 = Normal (but a disorder may still be present if compensation is occurring)
Step 2: Evaluate PaCO2
- In respiratory disorders: PaCO2 changes opposite to pH
- PaCO2 ↑ + pH ↓ = Respiratory acidosis
- PaCO2 ↓ + pH ↑ = Respiratory alkalosis
- In metabolic disorders: PaCO2 changes same direction as pH (compensatory)
Step 3: Evaluate HCO3-
- HCO3- < 22 mEq/L = Metabolic acidosis
- HCO3- > 26 mEq/L = Metabolic alkalosis
Step 4: Evaluate Base Excess/Deficit
- Normal: -4 to +4
- Positive (base excess) = Alkalosis
- Negative (base deficit) = Acidosis
The base deficit is calculated as shown below:
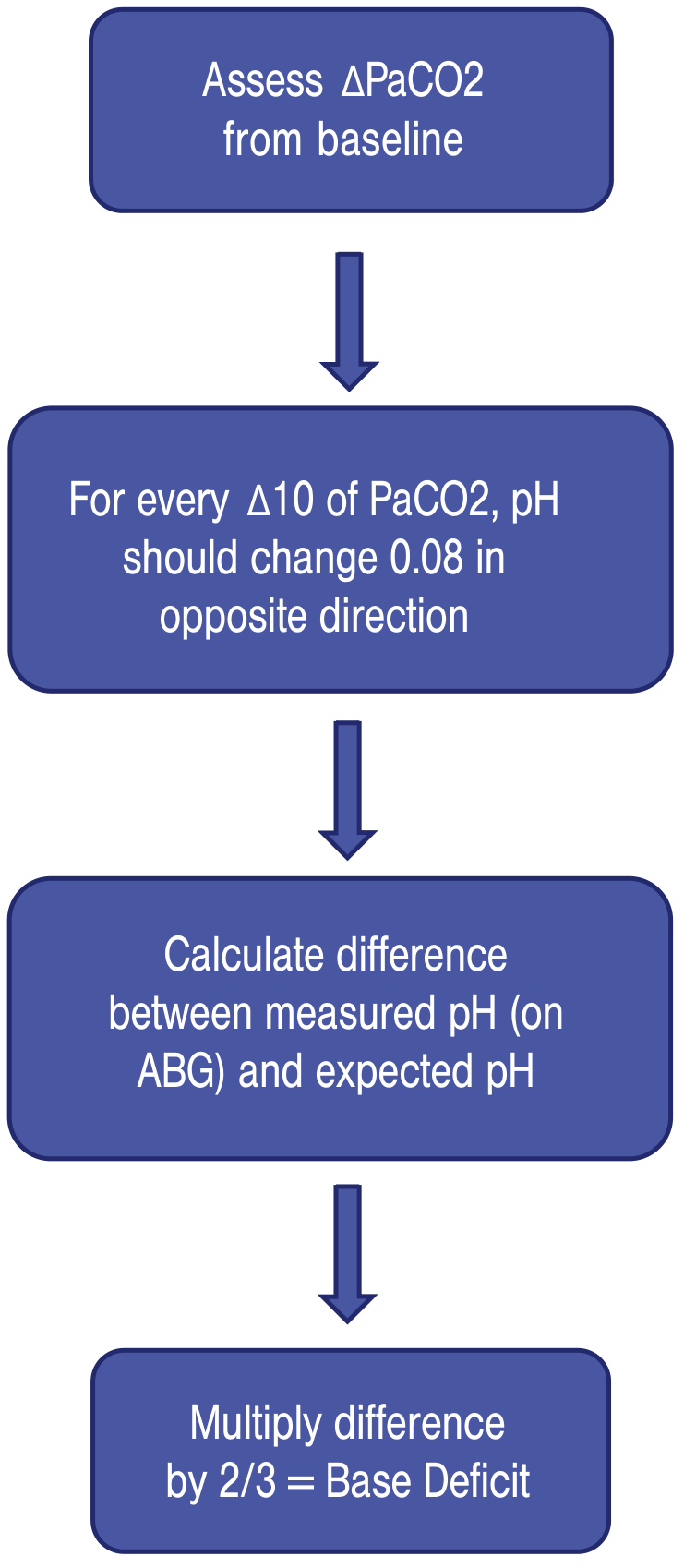
For every ΔPaCO2 of 10, pH changes by 0.08 in the opposite direction. The difference between measured and expected pH, multiplied by 2/3, gives the base deficit.
Bicarbonate deficit formula:
Bicarbonate deficit (mEq HCO3-) = 1/3 × body weight (kg) × base deficit
Step 5: Evaluate PaO2 and Oxygenation
- Hypoxemia (PaO2 < 75 mmHg) may be the cause or trigger of an acid-base disorder
- Calculate the A-a gradient: Alveolar PO2 - Arterial PO2
- Normal A-a gradient ≈ 10 mmHg (varies with age)
- A-a gradient > 20 = suggests underlying pulmonary pathology
Step 6: Check for Compensation and Mixed Disorders
The Four Primary Acid-Base Disorders
Summary Table
| Disorder | Primary Change | pH | Compensation | Renal/Respiratory Response |
|---|---|---|---|---|
| Metabolic Acidosis | ↓ HCO3- | ↓ | Hyperventilation | ↑ HCO3- reabsorption |
| Metabolic Alkalosis | ↑ HCO3- | ↑ | Hypoventilation | ↑ HCO3- excretion |
| Respiratory Acidosis | ↑ PaCO2 | ↓ | None (cause is respiratory) | ↑ HCO3- reabsorption |
| Respiratory Alkalosis | ↓ PaCO2 | ↑ | None | ↓ HCO3- reabsorption |
Key rule: If the disturbance is metabolic, the compensation is respiratory (and vice versa). The compensatory response always moves in the same direction as the original disturbance.
- Costanzo Physiology 7th Edition, p. 330
Compensation Formulas (Critical for Identifying Mixed Disorders)
| Disorder | Formula |
|---|---|
| Metabolic Acidosis | Expected PaCO2 = 1.5 × [HCO3-] + 8 ± 2 (Winter's Formula) |
| Metabolic Alkalosis | Expected PaCO2 = 0.7 × [HCO3-] + 20 ± 5 |
| Acute Respiratory Acidosis | ↑ HCO3- = ΔPaCO2 / 10 |
| Chronic Respiratory Acidosis | ↑ HCO3- = 4 × (ΔPaCO2 / 10) |
| Acute Respiratory Alkalosis | ↓ HCO3- = 2 × (ΔPaCO2 / 10) |
| Chronic Respiratory Alkalosis | ↓ HCO3- = 4 × (ΔPaCO2 / 10) |
- Current Surgical Therapy 14e, p. 1608
The Acid-Base Map
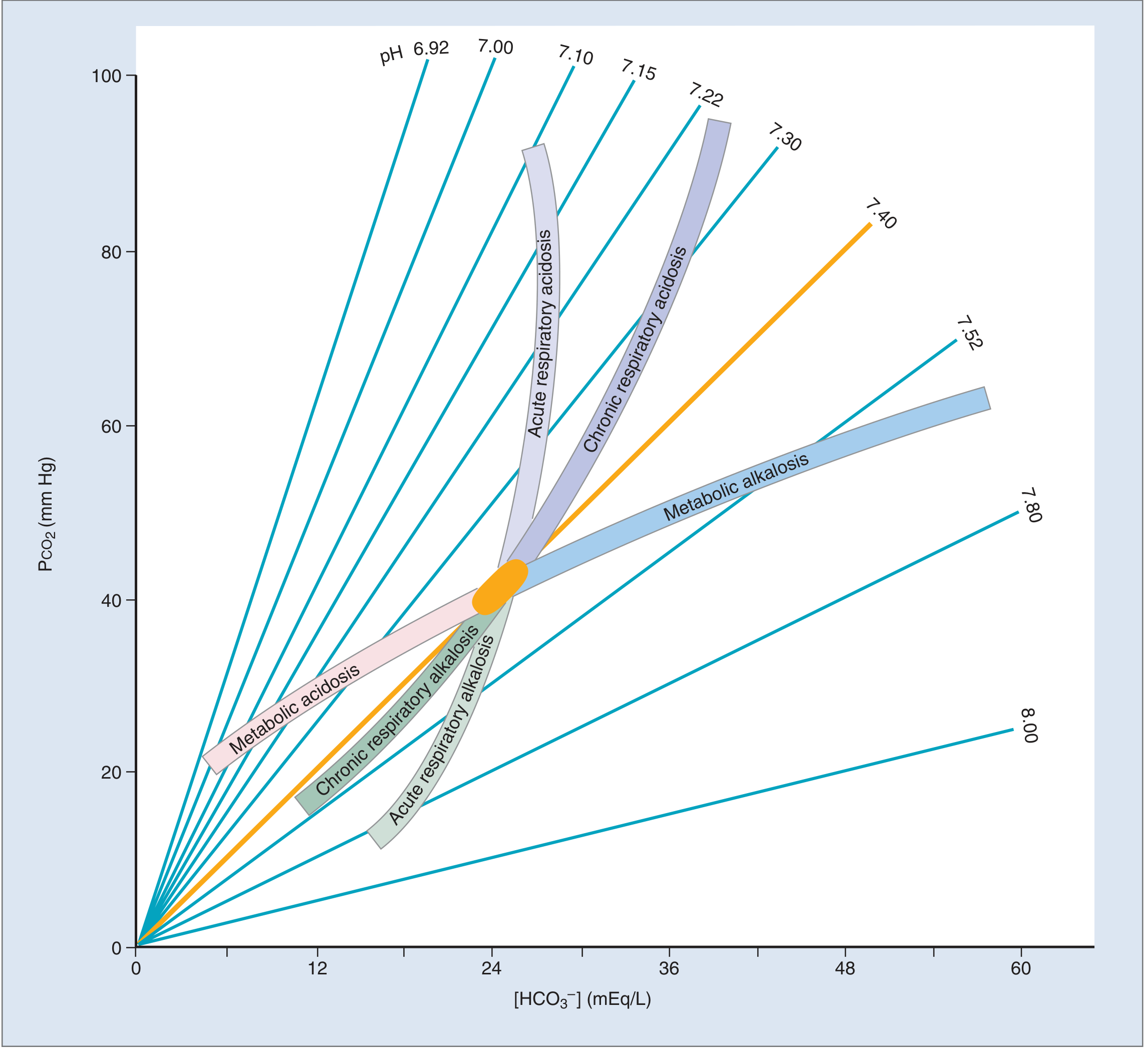
If the patient's values fall within a shaded band = simple disorder. If outside all bands = mixed disorder.
- Costanzo Physiology 7th Edition, p. 332
1. Metabolic Acidosis
Definition: HCO3- < 22 mEq/L, pH < 7.35
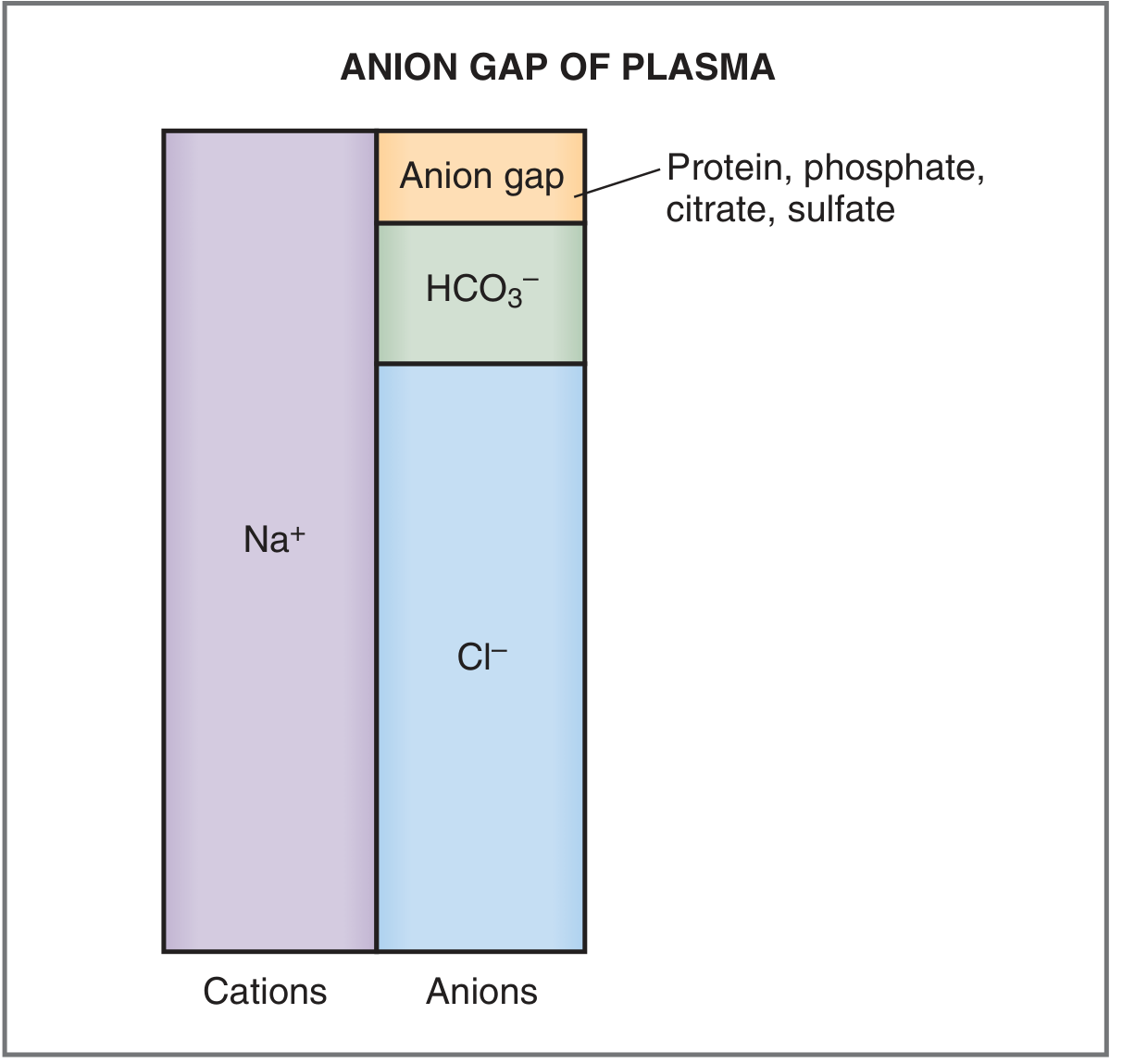
Key step: Calculate the Anion Gap (AG)
AG = Na+ - (Cl- + HCO3-) Normal AG = 8-12 mEq/L
High Anion Gap Metabolic Acidosis - MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol, Muscle injury (rhabdomyolysis), Metformin |
| U | Uremia (renal failure) |
| D | Diabetic ketoacidosis, alcoholic/starvation ketoacidosis |
| P | Propylene glycol, Paraldehyde |
| I | Isoniazid, Iron |
| L | Lactic acidosis (most common cause, ~50% of high-AG cases) |
| E | Ethanol, Ethylene glycol (antifreeze) |
| S | Salicylates, Short gut |
If AG is elevated but MUDPILES doesn't explain it, check the Osmol Gap:
Osmol gap = Measured osmolality - Calculated osmolality Calculated Osm = 2[Na+] + BUN/2.8 + glucose/18 + ethanol/4.6 Elevated osmol gap suggests toxic ingestion (methanol, ethylene glycol)
Normal Anion Gap Metabolic Acidosis (Hyperchloremic)
Causes: Diarrhea, Renal tubular acidosis (RTA), Excessive normal saline administration, GI fistulas, nasogastric suctioning
Remember: In normal saline (154 mEq/L each of Na and Cl), excess Cl displaces HCO3-, causing hyperchloremic metabolic acidosis.
Treatment: Address the underlying cause. For severe acidosis (pH < 7.15), exogenous bicarbonate may be used temporarily.
2. Metabolic Alkalosis
Definition: HCO3- > 26 mEq/L, pH > 7.45
Causes:
- Loss of H+ (vomiting, nasogastric drainage, loop/thiazide diuretics)
- Gain of HCO3- (exogenous bicarbonate, massive blood transfusion with citrate)
- Volume contraction (contraction alkalosis)
- Hyperaldosteronism
Compensation: Hypoventilation (CO2 retention), PaCO2 rises
- Expected PaCO2 = 0.7 × [HCO3-] + 20 ± 5
Risks: Associated with electrolyte disturbances (hypokalemia, hypocalcemia) and arrhythmias.
3. Respiratory Acidosis
Definition: PaCO2 > 45 mmHg, pH < 7.35 (due to hypoventilation/CO2 retention)
Acute vs. Chronic:
- Acute: For every ↑10 mmHg PaCO2, pH falls by 0.08 and HCO3- rises by ~1 mEq/L
- Chronic (3-5 days): Renal compensation - for every ↑10 mmHg PaCO2, HCO3- rises by 3.5-5 mEq/L; pH normalizes toward normal
Causes:
- CNS depression (opioids, sedatives, stroke, TBI)
- Neuromuscular disease (myasthenia gravis, GBS, ALS)
- Airway obstruction (COPD exacerbation, severe asthma)
- Chest wall disease (flail chest, kyphoscoliosis)
- Mucus plugging, pneumothorax
Treatment:
- Increase minute ventilation (↑ tidal volume or respiratory rate on ventilator)
- Non-invasive ventilation (BiPAP) - especially for COPD, heart failure
- If no improvement in 2 hours: consider intubation
- Salvage: VV-ECMO for severe refractory cases
A-a gradient guide:
- Normal A-a gradient + hypercapnia = reduced ventilatory drive (CNS, neuromuscular)
- Elevated A-a gradient (>20) + hypercapnia = pulmonary parenchymal disease
4. Respiratory Alkalosis
Definition: PaCO2 < 40 mmHg, pH > 7.45 (due to hyperventilation/CO2 loss)
Causes:
- Pain, anxiety, agitation
- Fever, sepsis (gram-negative)
- Brain tumors, CNS disorders
- Pulmonary disorders: PE, pneumothorax, pneumonia
- Pregnancy (chronic), heart failure, liver failure
- High altitude
- Classic: Salicylate toxicity initially causes respiratory alkalosis, then anion-gap metabolic acidosis
Compensation: Renal HCO3- excretion
- Acute: HCO3- falls by 2 mEq/L per 10 mmHg fall in PaCO2
- Chronic: HCO3- falls by 4 mEq/L per 10 mmHg fall in PaCO2
Treatment: Treat the underlying cause.
Mixed Acid-Base Disorders
A mixed disorder is present when the measured compensation differs from the predicted compensation (using formulas above). Examples:
- Respiratory acidosis + Metabolic acidosis: Inadequate ventilation (CO2 retention) + poor perfusion (lactic acidosis) - e.g., septic shock with respiratory failure
- Respiratory alkalosis + Metabolic alkalosis: Liver failure (hyperventilation) + vomiting
- Metabolic acidosis + Metabolic alkalosis: DKA with prolonged vomiting
Rule: If PaCO2 or HCO3- falls outside the predicted compensation range, a second disorder is superimposed.
Acute vs. Chronic Hypercapnia Quick Summary
| Feature | Acute | Chronic |
|---|---|---|
| PaCO2 | > 45 mmHg | > 45 mmHg |
| pH | < 7.35 (acidotic) | Near normal |
| HCO3- change per 10 mmHg ↑PaCO2 | +1 mEq/L | +3.5 - 5 mEq/L |
| Time course | Minutes to hours | 3-5 days |
- Murray & Nadel's Textbook of Respiratory Medicine, p. 974
Clinical Tips for Practice
- Always use a systematic approach (Steps 1-6 above) - never jump to conclusions
- HCO3- on ABG is calculated, not measured - use the simultaneous BMP for the true measured value when checking for mixed disorders
- PaO2 can be normal even with respiratory failure if the patient is on supplemental O2 - the PaCO2 is the better indicator of ventilation
- Pain or anxiety during arterial puncture can cause transient hyperventilation - use local lidocaine to minimize this artifact
- Base deficit is a useful trend marker for illness severity and correlates with mortality in surgical/trauma patients
- Check osmol gap whenever toxic alcohol ingestion is on the differential for a high AG metabolic acidosis
Sources:
- Current Surgical Therapy 14e (Enumah & Harris), pp. 1607-1610
- Costanzo Physiology 7th Edition, pp. 330-333
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 974-975
- ROSEN's Emergency Medicine, pp. 1481-1649
- Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.