






+10 more
Diagnosis
Reading File
Finding Sources
Searching PubMed
"adult T-cell leukemia lymphoma" HTLV-1 diagnosis treatment
Finding Sources
Reading Article
PMID: 37300656
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Here is my full diagnostic interpretation:
Diagnosis: Adult T-Cell Leukemia/Lymphoma (ATLL) - Acute Subtype (Most Likely)
This is the formal laboratory conclusion, and the flow cytometry data strongly supports it. Here is a structured breakdown.
Patient Summary
- Patient: Mr. Rajendra Dagu Nagare, Male, 56 years
- Referring physician: Dr. Nilesh Wasekar (Hematologist), Nashik
- Clinical history: Lymphocytosis
CBC Findings (NHS Diagnostics, 9 Jul 2026)
| Parameter | Value | Reference | Comment |
|---|---|---|---|
| WBC | 49,880/cmm | 4,000-11,000 | Markedly elevated |
| Lymphocytes | 57.4% (28,640/cmm abs.) | 20-40% | Absolute lymphocytosis |
| Neutrophils | 15.7% | 40-80% | Relative neutropenia |
| Monocytes | 25.4% | 4-7% | Elevated |
| Platelets | 85,000 | 150,000-450,000 | Thrombocytopenic |
| Hb | 14.2 g/dL | 13-17 | Normal |
Peripheral smear (NHS report): 57% atypical lymphoid cells with pale cytoplasm and polar villi - initially suspected Splenic Marginal Zone Lymphoma with villous lymphocytes (SMZL). Flow cytometry was advised and performed.
Immunophenotyping (Unipath/Unigenome, 10 Jul 2026)
Abnormal population: 74% of cells
| Positive Markers | Negative Markers |
|---|---|
| CD45 (Bright), CD2, CD3 (Bright), CD4 (Variable), CD5, CD7, CD8 (Bright), CD25 (Moderate), CD26 (Dim), CD52 (Moderate) | CD19, Kappa, Lambda, CD38, CD34, CD10, CD16, CD56, CD57, TCRγδ, TRBC1 |
Key findings in the flow cytometry plots:
- CD3+: 99.26% of T-cells
- CD8+: 99.00% (dominant; unusual for typical ATLL which is usually CD4+ CD8-)
- CD4+: only 0.65%
- TCR αβ expressing cells (TRBC1 negative = 98.47%) - clonal T-cell population
- CD52 expression on 92.69% of abnormal cells (targeted immunotherapy relevant)
- Small cell size, low side scatter
- B cells only 0.71%, NK cells 0.85% - virtually absent
Why ATLL and Not SMZL
The initial peripheral smear impression of SMZL was revised by flow cytometry. SMZL is a B-cell neoplasm (CD19+, CD20+, surface Ig+, villous lymphocytes), but this patient's cells are:
- CD19 negative, Kappa/Lambda negative (B-cell markers all absent)
- Mature T-cell phenotype: CD3+ CD2+ CD5+ CD7+ CD25+
- TRBC1 negative = clonal T-cell expansion (TCR beta chain clonality marker)
- The "villi" on smear were likely cytoplasmic protrusions of atypical T-cells, not true B-cell villi
ATLL Subtype Consideration
ATLL has 4 subtypes (Shimoyama classification):
| Subtype | Features | % of ATLL |
|---|---|---|
| Acute | High WBC, hypercalcemia, LDH elevated, skin lesions, rapid progression | ~55% |
| Lymphoma | Lymphadenopathy without leukemia | ~20% |
| Chronic | Moderate lymphocytosis, exfoliative dermatitis | ~20% |
| Smoldering | Skin/lung involvement, low WBC | ~5% |
This patient's high WBC (~50,000/cmm), thrombocytopenia (85K platelets), and 74% circulating abnormal cells point toward the acute leukemic subtype, the most aggressive form with median survival under 1 year without aggressive treatment.
The CD8-dominant pattern (CD8+ 99%, CD4+ 0.65%) is atypical - classic ATLL is CD4+CD8-, but CD8+ ATLL variants do exist and carry similar or worse prognosis. This warrants careful review.
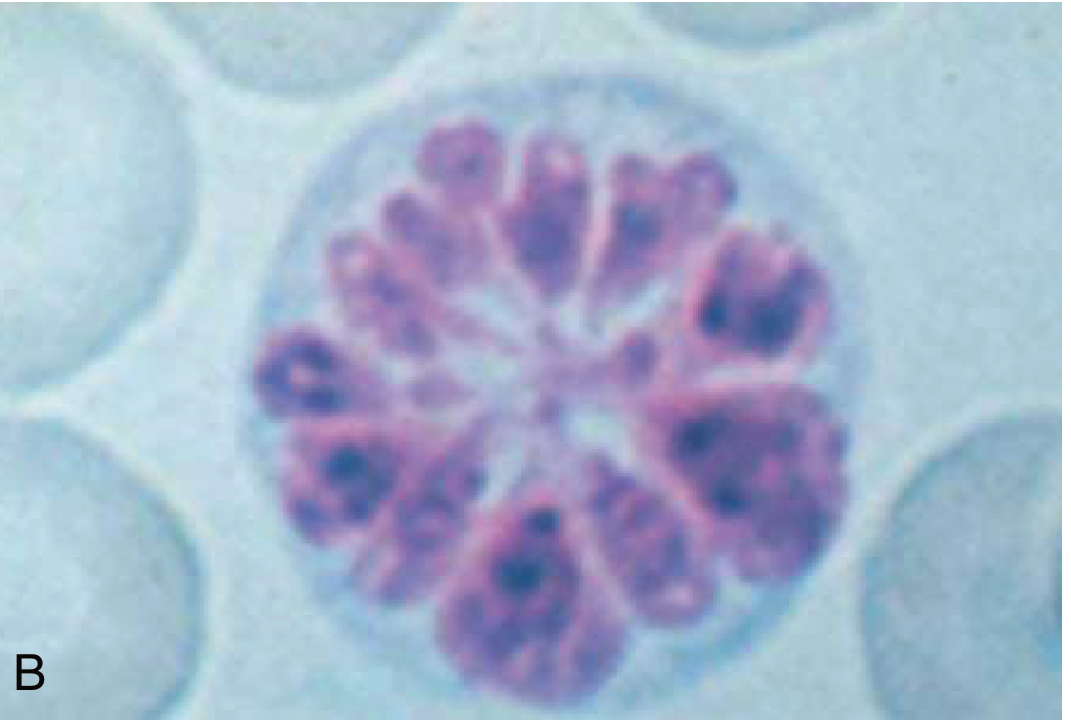
Characteristic "Flower Cell" of ATLL
The pathognomonic flower cell (polylobulated nucleus) of ATLL:
Mandatory Next Step: HTLV-1 Serology
The lab report itself advises: "HTLV-1 by serology"
HTLV-1 (Human T-Lymphotropic Virus type 1) is the causative retrovirus of ATLL. Confirmation requires:
- HTLV-1 antibody serology (ELISA + confirmatory Western blot)
- PCR for HTLV-1 proviral load - confirms infection and quantifies burden
- Cytogenetics/FISH - complex chromosomal abnormalities are common
- If serology confirms, bone marrow biopsy for staging
Note: Isolated flow cytometry alone is not sufficient for final diagnosis - must be correlated with HTLV-1 serology, clinical staging, and imaging (CT chest/abdomen/pelvis for lymphadenopathy and organomegaly).
Targeted Immunotherapy Note
The report identifies CD52 expression at 92.69% on abnormal cells, suggesting potential eligibility for Alemtuzumab (anti-CD52 monoclonal antibody), though its use in ATLL is investigational rather than standard-of-care.
Summary
Adult T-Cell Leukemia/Lymphoma (ATLL), likely acute subtype - caused by HTLV-1 retrovirus. Mature T-cell neoplasm with clonal CD3+/CD8+/CD25+ population, 74% abnormal circulating cells, thrombocytopenia, and leukocytosis. HTLV-1 serology is urgently required to confirm etiology. This is a high-grade malignancy requiring urgent hematology-oncology referral for treatment planning, including consideration of allogeneic stem cell transplantation in eligible patients.
Sources: Goldman-Cecil Medicine International Edition; Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis and Management by Laboratory Methods; Stuver et al., 2023, Curr Treat Options Oncol - treatment review
Create a summary document for the treating clinician
Reading File
Running Command
mkdir -p /home/daytona/workspace/atll-summary && ls /home/daytona/workspace/
Writing File
~/atll-summary/create_summary.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, Header, Footer, PageNumber, NumberFormat, UnderlineType,
TableBorders
} = require('docx');
const fs = require('fs');
// ── Color palette ──────────────────────────────────────────────
const DARK_BLUE = "1B3A6B";
const MED_BLUE = "2E6DA4";
const LIGHT_BLUE = "D6E4F7";
const RED_ALERT = "C0392B";
const AMBER = "E67E22";
const WHITE = "FFFFFF";
const LIGHT_GREY = "F2F2F2";
const MID_GREY = "D0D0D0";
const DARK_GREY = "4A4A4A";
// ── Helpers ────────────────────────────────────────────────────
function hRule() {
return new Paragraph({
border: { bottom: { color: MED_BLUE, space: 1, value: BorderStyle.SINGLE, size: 12 } },
spacing: { before: 100, after: 100 },
children: []
});
}
function sectionHeading(text, color = DARK_BLUE) {
return new Paragraph({
heading: HeadingLevel.HEADING_2,
spacing: { before: 280, after: 80 },
border: { bottom: { color: MED_BLUE, space: 1, value: BorderStyle.SINGLE, size: 6 } },
children: [new TextRun({ text, bold: true, color, size: 26, font: "Calibri" })]
});
}
function bodyText(text, opts = {}) {
return new Paragraph({
spacing: { before: 60, after: 60 },
children: [new TextRun({ text, size: 21, font: "Calibri", color: DARK_GREY, ...opts })]
});
}
function bulletText(text, bold = false, color = DARK_GREY) {
return new Paragraph({
bullet: { level: 0 },
spacing: { before: 40, after: 40 },
children: [new TextRun({ text, size: 21, font: "Calibri", bold, color })]
});
}
function subBullet(text) {
return new Paragraph({
bullet: { level: 1 },
spacing: { before: 20, after: 20 },
children: [new TextRun({ text, size: 20, font: "Calibri", color: DARK_GREY })]
});
}
function cell(text, opts = {}) {
const {
bold = false, bg = WHITE, color = DARK_GREY, align = AlignmentType.LEFT,
isHeader = false
} = opts;
return new TableCell({
shading: bg !== WHITE ? { fill: bg, type: ShadingType.CLEAR, color: "auto" } : undefined,
verticalAlign: VerticalAlign.CENTER,
margins: { top: 80, bottom: 80, left: 120, right: 120 },
children: [new Paragraph({
alignment: align,
children: [new TextRun({ text: String(text), bold: bold || isHeader, size: isHeader ? 20 : 20, font: "Calibri", color: isHeader ? WHITE : color })]
})]
});
}
function hCell(text, align = AlignmentType.LEFT) {
return cell(text, { bold: true, bg: DARK_BLUE, color: WHITE, isHeader: true, align });
}
function thinBorder() {
return {
top: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY },
bottom: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY },
left: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY },
right: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY },
insideHorizontal: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY },
insideVertical: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY }
};
}
// ═══════════════════════════════════════════════════════════════
// DOCUMENT
// ═══════════════════════════════════════════════════════════════
const doc = new Document({
numbering: {
config: [
{
reference: "default-bullet",
levels: [
{ level: 0, format: "bullet", text: "\u2022", alignment: AlignmentType.LEFT, style: { paragraph: { indent: { left: 360, hanging: 260 } } } },
{ level: 1, format: "bullet", text: "\u25E6", alignment: AlignmentType.LEFT, style: { paragraph: { indent: { left: 720, hanging: 260 } } } }
]
}
]
},
styles: {
default: {
document: {
run: { font: "Calibri", size: 21, color: DARK_GREY }
}
}
},
sections: [{
properties: {
page: {
margin: { top: 900, right: 900, bottom: 900, left: 900 }
}
},
headers: {
default: new Header({
children: [
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: { top: { style: BorderStyle.NONE }, bottom: { style: BorderStyle.SINGLE, size: 8, color: MED_BLUE }, left: { style: BorderStyle.NONE }, right: { style: BorderStyle.NONE }, insideHorizontal: { style: BorderStyle.NONE }, insideVertical: { style: BorderStyle.NONE } },
rows: [new TableRow({ children: [
new TableCell({
width: { size: 70, type: WidthType.PERCENTAGE },
borders: { top: { style: BorderStyle.NONE }, bottom: { style: BorderStyle.NONE }, left: { style: BorderStyle.NONE }, right: { style: BorderStyle.NONE } },
children: [
new Paragraph({ children: [new TextRun({ text: "CLINICAL SUMMARY REPORT", bold: true, size: 28, color: DARK_BLUE, font: "Calibri" })] }),
new Paragraph({ children: [new TextRun({ text: "Adult T-Cell Leukemia / Lymphoma (ATLL)", size: 22, color: MED_BLUE, font: "Calibri" })] })
]
}),
new TableCell({
width: { size: 30, type: WidthType.PERCENTAGE },
borders: { top: { style: BorderStyle.NONE }, bottom: { style: BorderStyle.NONE }, left: { style: BorderStyle.NONE }, right: { style: BorderStyle.NONE } },
children: [
new Paragraph({ alignment: AlignmentType.RIGHT, children: [new TextRun({ text: "Nashik Haematology Service", size: 18, color: DARK_GREY, font: "Calibri" })] }),
new Paragraph({ alignment: AlignmentType.RIGHT, children: [new TextRun({ text: "Report Date: 11-Jul-2026", size: 18, color: DARK_GREY, font: "Calibri" })] })
]
})
]})]
})
]
})
},
footers: {
default: new Footer({
children: [new Paragraph({
alignment: AlignmentType.CENTER,
border: { top: { style: BorderStyle.SINGLE, size: 4, color: MID_GREY } },
children: [
new TextRun({ text: "CONFIDENTIAL - For treating clinician use only | ", size: 18, color: DARK_GREY, font: "Calibri" }),
new TextRun({ text: "Page ", size: 18, color: DARK_GREY, font: "Calibri" }),
new TextRun({ children: [PageNumber.CURRENT], size: 18, font: "Calibri" }),
new TextRun({ text: " of ", size: 18, color: DARK_GREY, font: "Calibri" }),
new TextRun({ children: [PageNumber.TOTAL_PAGES], size: 18, font: "Calibri" })
]
})]
})
},
children: [
// ── ALERT BANNER ──
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [new TableRow({ children: [
new TableCell({
shading: { fill: RED_ALERT, type: ShadingType.CLEAR, color: "auto" },
margins: { top: 120, bottom: 120, left: 200, right: 200 },
children: [new Paragraph({
alignment: AlignmentType.CENTER,
children: [new TextRun({ text: "⚠ URGENT HAEMATOLOGY-ONCOLOGY REFERRAL REQUIRED ⚠", bold: true, size: 24, color: WHITE, font: "Calibri" })]
})]
})
]})]
}),
new Paragraph({ spacing: { before: 200, after: 0 }, children: [] }),
// ── PATIENT DEMOGRAPHICS ──
sectionHeading("1. Patient Details"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [
hCell("Patient Name"), hCell("Age / Sex"), hCell("Reg. No."), hCell("Sample Date")
]}),
new TableRow({ children: [
cell("Mr. Rajendra Dagu Nagare"), cell("56 Years / Male"), cell("60700200476"), cell("10-Jul-2026")
]}),
new TableRow({ children: [
hCell("Referring Physician"), hCell("Source"), hCell("Report Lab"), hCell("Report Date")
]}),
new TableRow({ children: [
cell("Dr. Nilesh Wasekar (DM Haematology)"), cell("Shrinath Hospital, Nashik"), cell("Unipath / Unigenome, Ahmedabad"), cell("11-Jul-2026")
]})
]
}),
// ── DIAGNOSIS ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("2. Diagnosis"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [new TableRow({ children: [
new TableCell({
shading: { fill: LIGHT_BLUE, type: ShadingType.CLEAR, color: "auto" },
margins: { top: 140, bottom: 140, left: 200, right: 200 },
children: [
new Paragraph({ children: [new TextRun({ text: "Primary Diagnosis:", bold: true, size: 22, color: DARK_BLUE, font: "Calibri" })] }),
new Paragraph({ spacing: { before: 80 }, children: [new TextRun({ text: "Adult T-Cell Leukemia / Lymphoma (ATLL) - Acute Subtype (Most Likely)", bold: true, size: 28, color: RED_ALERT, font: "Calibri" })] }),
new Paragraph({ spacing: { before: 80 }, children: [new TextRun({ text: "Causative agent: HTLV-1 retrovirus (serology confirmation pending)", size: 21, color: DARK_GREY, font: "Calibri", italics: true })] })
]
})
]})]
}),
new Paragraph({ spacing: { before: 160, after: 0 }, children: [] }),
bodyText("The flow cytometry immunophenotyping (Leukemia/Lymphoma Panel, Unipath) identifies a clonal, mature T-cell neoplasm comprising 74% of the circulating lymphoid cells. The morphological and immunophenotypic features are consistent with ATLL, a high-grade T-cell malignancy driven by HTLV-1 infection."),
// ── CBC SUMMARY ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("3. CBC & Peripheral Smear (NHS Diagnostics, 09-Jul-2026)"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Parameter"), hCell("Value"), hCell("Reference Range"), hCell("Status")] }),
new TableRow({ children: [cell("Haemoglobin"), cell("14.2 g/dL"), cell("13.0-17.0"), cell("Normal", { color: "2E7D32" })] }),
new TableRow({ children: [cell("Total Leucocytes (WBC)"), cell("49,880 /cmm"), cell("4,000-11,000"), cell("HIGH ▲", { bold: true, color: RED_ALERT })] }),
new TableRow({ children: [cell("Neutrophils"), cell("15.7% (7,810/cmm abs.)"), cell("40-80%"), cell("LOW ▼", { bold: true, color: AMBER })] }),
new TableRow({ children: [cell("Lymphocytes"), cell("57.4% (28,640/cmm abs.)"), cell("20-40%"), cell("HIGH ▲", { bold: true, color: RED_ALERT })] }),
new TableRow({ children: [cell("Monocytes"), cell("25.4% (12,690/cmm abs.)"), cell("4-7%"), cell("HIGH ▲", { bold: true, color: AMBER })] }),
new TableRow({ children: [cell("Platelets"), cell("85,000 /μL"), cell("150,000-450,000"), cell("LOW ▼ (Thrombocytopenia)", { bold: true, color: RED_ALERT })] }),
new TableRow({ children: [cell("Platelet Distribution Width"), cell("20.3%"), cell("10.0-17.9%"), cell("Elevated", { color: AMBER })] })
]
}),
new Paragraph({ spacing: { before: 120, after: 0 }, children: [] }),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [new TableRow({ children: [
new TableCell({
shading: { fill: LIGHT_GREY, type: ShadingType.CLEAR, color: "auto" },
margins: { top: 100, bottom: 100, left: 160, right: 160 },
children: [
new Paragraph({ children: [new TextRun({ text: "Peripheral Smear Findings:", bold: true, size: 21, font: "Calibri", color: DARK_BLUE })] }),
new Paragraph({ spacing: { before: 60 }, children: [new TextRun({ text: "57% atypical lymphoid cells with pale cytoplasm and predominantly polar villi. Platelets reduced. No haemoparasites. RBCs normocytic normochromic. Initial morphological impression: Chronic Lymphoproliferative Disorder (? Splenic Marginal Zone Lymphoma). Flow cytometry confirmed T-cell phenotype - B-cell differential excluded.", size: 20, font: "Calibri", color: DARK_GREY })] })
]
})
]})]
}),
// ── FLOW CYTOMETRY ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("4. Flow Cytometry Immunophenotyping (Unipath, 10-Jul-2026)"),
bodyText("Method: 10-colour flow cytometry, Beckman Coulter DxFLEX. Gating: CD45 vs SSC. Specimen: Peripheral blood."),
new Paragraph({ spacing: { before: 120, after: 60 }, children: [new TextRun({ text: "Abnormal Population: 74% of cells | Cell size: Small | Side scatter: Low | Viability: 94%", bold: true, size: 22, color: RED_ALERT, font: "Calibri" })] }),
new Paragraph({ spacing: { before: 100, after: 60 }, children: [new TextRun({ text: "Marker Expression", bold: true, size: 21, color: DARK_BLUE, font: "Calibri" })] }),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Marker"), hCell("Intensity"), hCell("Result"), hCell("Marker"), hCell("Intensity"), hCell("Result")] }),
new TableRow({ children: [cell("CD45"), cell("Bright"), cell("POSITIVE", { bold: true, color: "2E7D32" }), cell("CD2"), cell("Moderate"), cell("POSITIVE", { bold: true, color: "2E7D32" })] }),
new TableRow({ children: [cell("CD3"), cell("Bright"), cell("POSITIVE", { bold: true, color: "2E7D32" }), cell("CD5"), cell("Moderate"), cell("POSITIVE", { bold: true, color: "2E7D32" })] }),
new TableRow({ children: [cell("CD7"), cell("Dim-Moderate"), cell("POSITIVE", { bold: true, color: "2E7D32" }), cell("CD8"), cell("Bright"), cell("POSITIVE", { bold: true, color: "2E7D32" })] }),
new TableRow({ children: [cell("CD4"), cell("Variable"), cell("POSITIVE (0.65%)", { color: AMBER }), cell("CD25"), cell("Moderate"), cell("POSITIVE", { bold: true, color: "2E7D32" })] }),
new TableRow({ children: [cell("CD26"), cell("Dim"), cell("POSITIVE", { bold: true, color: "2E7D32" }), cell("CD52"), cell("Moderate (92.69%)"), cell("POSITIVE", { bold: true, color: "2E7D32" })] }),
new TableRow({ children: [cell("CD19"), cell("-"), cell("Negative"), cell("Kappa / Lambda"), cell("-"), cell("Negative (B-cell markers absent)")] }),
new TableRow({ children: [cell("CD34"), cell("-"), cell("Negative"), cell("TCRγδ"), cell("-"), cell("Negative")] }),
new TableRow({ children: [cell("TRBC1"), cell("-"), cell("Negative*"), cell("CD16 / CD56 / CD57"), cell("-"), cell("Negative")] })
]
}),
new Paragraph({ spacing: { before: 80, after: 40 }, children: [new TextRun({ text: "* TRBC1 negativity (98.47% of cells) confirms clonal T-cell receptor beta-chain expression - diagnostic of clonal T-cell neoplasm.", size: 19, font: "Calibri", color: DARK_GREY, italics: true })] }),
new Paragraph({ spacing: { before: 120, after: 60 }, children: [new TextRun({ text: "T-Cell Subset Analysis", bold: true, size: 21, color: DARK_BLUE, font: "Calibri" })] }),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Parameter"), hCell("Value"), hCell("Significance")] }),
new TableRow({ children: [cell("CD3+ T-cells"), cell("99.26% of lymphoid gate"), cell("Near-total T-cell expansion")] }),
new TableRow({ children: [cell("CD8+ (within TCRαβ)"), cell("99.00%"), cell("Dominant CD8+ phenotype (atypical for ATLL)", { color: AMBER })] }),
new TableRow({ children: [cell("CD4+"), cell("0.65%"), cell("Markedly suppressed normal CD4+ T-helpers")] }),
new TableRow({ children: [cell("TCRγδ+"), cell("1.11%"), cell("Normal range - not a γδ T-cell lymphoma")] }),
new TableRow({ children: [cell("NK cells (CD3-/CD56+)"), cell("0.85%"), cell("Near absent")] }),
new TableRow({ children: [cell("B cells"), cell("0.71%"), cell("Near absent - B-cell lymphoma excluded")] })
]
}),
// ── IMMUNOTHERAPY TARGET ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("5. Immunotherapy Target (Lab-Identified)"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Target"), hCell("Clone"), hCell("Expression (%)"), hCell("Drug"), hCell("Status")] }),
new TableRow({ children: [
cell("CD52"), cell("ALEMMUT.RMAB"), cell("92.69% of abnormal cells", { bold: true, color: "2E7D32" }), cell("Alemtuzumab (anti-CD52)"), cell("Investigational in ATLL")
]})
]
}),
new Paragraph({ spacing: { before: 80 }, children: [new TextRun({ text: "Note: CD52 expression is high but Alemtuzumab is not standard first-line for ATLL. Discuss in MDT.", size: 19, font: "Calibri", color: DARK_GREY, italics: true })] }),
// ── DIAGNOSTIC REASONING ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("6. Diagnostic Reasoning & Differential Diagnosis"),
bodyText("The combination of findings below supports ATLL as the unifying diagnosis:"),
bulletText("Markedly elevated WBC with absolute lymphocytosis (ALC ~37,320/cmm per flow report)"),
bulletText("74% circulating clonal T-cells - small cell, low side scatter morphology"),
bulletText("Mature T-cell phenotype: CD3+, CD2+, CD5+, CD7+, CD8 bright - all negative for B-cell, NK-cell, and precursor markers"),
bulletText("CD25 (IL-2 receptor alpha) expression - a hallmark of ATLL malignant T-cells"),
bulletText("TRBC1 negativity confirms clonality (TCR beta chain clonal rearrangement)"),
bulletText("Thrombocytopenia (85K) - consistent with bone marrow infiltration"),
bulletText("Age 56 (fifth-to-seventh decade peak for ATLL)"),
new Paragraph({ spacing: { before: 140, after: 60 }, children: [new TextRun({ text: "Differentials Considered and Excluded:", bold: true, size: 21, color: DARK_BLUE, font: "Calibri" })] }),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Differential"), hCell("Reason Excluded")] }),
new TableRow({ children: [cell("Splenic Marginal Zone Lymphoma (initial smear impression)"), cell("B-cell neoplasm; CD19 neg, Kappa/Lambda neg - definitively excluded by flow cytometry")] }),
new TableRow({ children: [cell("T-Prolymphocytic Leukemia (T-PLL)"), cell("T-PLL is typically CD4+ (60%) or CD4+/CD8+; our case is CD8-dominant; CD25 usually negative in T-PLL; TCL1 not tested")] }),
new TableRow({ children: [cell("Sezary Syndrome / Mycosis Fungoides"), cell("Requires skin biopsy evidence and CD4+ Sezary cells; CD8 dominant here makes it less likely")] }),
new TableRow({ children: [cell("T-LGL Leukemia"), cell("T-LGL is CD8+/CD57+/CD56+; CD57 and CD56 are negative here; neutropenia not dominant")] }),
new TableRow({ children: [cell("NK/T-cell Lymphoma"), cell("CD56 negative; TCRγδ negative; EBV-driven - different entity")] })
]
}),
new Paragraph({ spacing: { before: 80 }, children: [new TextRun({ text: "The CD8-dominant phenotype (99% CD8+) is atypical for classic ATLL (which is usually CD4+CD8-). However, CD8+ ATLL variants are documented and carry comparable or worse prognosis. Confirmation with HTLV-1 serology is essential.", size: 19, font: "Calibri", color: AMBER, italics: true })] }),
// ── PENDING INVESTIGATIONS ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("7. Urgent Pending Investigations"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Test"), hCell("Purpose"), hCell("Priority")] }),
new TableRow({ children: [cell("HTLV-1 Serology (ELISA + Western Blot)"), cell("Confirm causative retrovirus - mandatory for ATLL diagnosis"), cell("URGENT", { bold: true, color: RED_ALERT })] }),
new TableRow({ children: [cell("HTLV-1 Proviral Load (PCR)"), cell("Quantify viral burden; aids prognosis"), cell("Urgent", { color: RED_ALERT })] }),
new TableRow({ children: [cell("LDH, Uric Acid, Calcium, Beta-2 Microglobulin"), cell("Staging markers; hypercalcaemia is a hallmark of acute ATLL"), cell("Urgent", { color: RED_ALERT })] }),
new TableRow({ children: [cell("CT Chest / Abdomen / Pelvis with contrast"), cell("Assess lymphadenopathy, hepatosplenomegaly, organ involvement"), cell("Urgent", { color: RED_ALERT })] }),
new TableRow({ children: [cell("Bone Marrow Aspirate & Trephine Biopsy"), cell("Assess marrow infiltration; staging"), cell("Urgent", { color: RED_ALERT })] }),
new TableRow({ children: [cell("Cytogenetics / FISH / Molecular Panel"), cell("Complex karyotype common in ATLL; CCR4 mutation (prognostic)"), cell("High Priority", { color: AMBER })] }),
new TableRow({ children: [cell("TCR Gene Rearrangement (Southern blot or PCR)"), cell("Confirm clonality at molecular level"), cell("High Priority", { color: AMBER })] }),
new TableRow({ children: [cell("Serum Albumin, BUN (renal function)"), cell("Elevated BUN + low albumin = unfavourable chronic ATLL prognosis"), cell("Standard")] }),
new TableRow({ children: [cell("HTLV-1 PCR on CSF (if neurological symptoms)"), cell("Exclude CNS involvement / HAM-TSP"), cell("As indicated")] })
]
}),
// ── SUBTYPE & PROGNOSIS ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("8. ATLL Subtype Classification (Shimoyama) & Prognosis"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [
new TableRow({ children: [hCell("Subtype"), hCell("Key Features"), hCell("Proportion"), hCell("Median OS")] }),
new TableRow({
children: [
new TableCell({
shading: { fill: "FDECEA", type: ShadingType.CLEAR, color: "auto" },
margins: { top: 80, bottom: 80, left: 120, right: 120 },
children: [new Paragraph({ children: [new TextRun({ text: "Acute ← LIKELY", bold: true, size: 20, color: RED_ALERT, font: "Calibri" })] })]
}),
cell("High WBC, hypercalcaemia, LDH elevation, skin lesions, circulating leukemic cells"),
cell("~55%"),
cell("< 1 year without alloHCT", { bold: true, color: RED_ALERT })
]
}),
new TableRow({ children: [cell("Lymphoma"), cell("Lymphadenopathy dominant; WBC normal or mildly elevated"), cell("~20%"), cell("< 1 year")] }),
new TableRow({ children: [cell("Chronic"), cell("Moderate lymphocytosis, skin involvement; slower course"), cell("~20%"), cell("~2 years")] }),
new TableRow({ children: [cell("Smoldering"), cell("Low WBC, skin/lung involvement; indolent"), cell("~5%"), cell(">5 years")] })
]
}),
new Paragraph({ spacing: { before: 80 }, children: [new TextRun({ text: "Prognostic factors conferring adverse outcome in acute ATLL: age >40, PS ≥2, hypercalcaemia, elevated LDH, ≥4 involved lesions, high BUN, low albumin.", size: 19, font: "Calibri", color: DARK_GREY, italics: true })] }),
// ── TREATMENT ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("9. Treatment Framework (Per Current Evidence)"),
bodyText("Treatment is determined by ATLL subtype, HTLV-1 confirmation, patient fitness (ECOG PS), and intent for allogeneic haematopoietic cell transplantation (alloHCT)."),
new Paragraph({ spacing: { before: 120, after: 60 }, children: [new TextRun({ text: "Acute / Lymphoma ATLL (Aggressive Subtypes):", bold: true, size: 21, color: DARK_BLUE, font: "Calibri" })] }),
bulletText("First-line: VCAP-AMP-VECP (Japan) or CHOP-based regimens (Western centres)"),
bulletText("Mogamulizumab (anti-CCR4) approved in Japan and USA for relapsed/refractory ATLL; CCR4 expression >90% in ATLL"),
bulletText("Allogeneic HCT: Only potentially curative option; 3-year OS ~30-40% in transplanted patients"),
subBullet("Refer for HLA typing and donor search early if patient is transplant-eligible"),
bulletText("Brentuximab vedotin (if CD30+), Pralatrexate, Romidepsin - alternative agents for relapsed disease"),
bulletText("Lenalidomide: Active in relapsed ATLL; being studied in combination regimens"),
new Paragraph({ spacing: { before: 120, after: 60 }, children: [new TextRun({ text: "Smoldering / Chronic ATLL (Indolent Subtypes):", bold: true, size: 21, color: DARK_BLUE, font: "Calibri" })] }),
bulletText("Antiviral: Zidovudine 500-1000 mg/day + Interferon-alpha 6-9 MU - improves 5-year survival in indolent disease"),
bulletText("Watch-and-wait acceptable for truly asymptomatic smoldering type"),
bulletText("~50% transform to aggressive disease at median 18 months - close surveillance mandatory"),
// ── SUMMARY BOX ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("10. Clinical Summary & Action Points"),
new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: thinBorder(),
rows: [new TableRow({ children: [
new TableCell({
shading: { fill: LIGHT_BLUE, type: ShadingType.CLEAR, color: "auto" },
margins: { top: 140, bottom: 140, left: 200, right: 200 },
children: [
new Paragraph({ spacing: { before: 0, after: 80 }, children: [new TextRun({ text: "Mr. Rajendra Dagu Nagare, 56M, presents with lymphocytosis (WBC ~50,000/cmm) and thrombocytopenia. Peripheral smear showed atypical lymphoid cells initially suggesting SMZL. Flow cytometry (10-colour panel) identifies a 74% clonal, mature T-cell population expressing CD3, CD2, CD5, CD7, CD8, CD25, CD26, and CD52, with absent B-cell and NK-cell markers. TRBC1 negativity confirms clonal T-cell receptor rearrangement.", size: 20, font: "Calibri", color: DARK_GREY })] }),
new Paragraph({ spacing: { before: 60, after: 80 }, children: [new TextRun({ text: "The immunophenotype is consistent with Adult T-Cell Leukemia/Lymphoma (ATLL), most likely acute subtype. HTLV-1 serology is mandatorily required to confirm the diagnosis. The CD8-dominant phenotype (unusual for ATLL) warrants specialist review but does not exclude ATLL.", size: 20, font: "Calibri", color: DARK_GREY })] }),
new Paragraph({ spacing: { before: 60, after: 40 }, children: [new TextRun({ text: "Immediate action steps:", bold: true, size: 21, color: DARK_BLUE, font: "Calibri" })] }),
new Paragraph({ bullet: { level: 0 }, children: [new TextRun({ text: "Send HTLV-1 ELISA serology TODAY", bold: true, size: 20, color: RED_ALERT, font: "Calibri" })] }),
new Paragraph({ bullet: { level: 0 }, children: [new TextRun({ text: "Order serum calcium, LDH, uric acid, B2M, albumin, renal function", size: 20, font: "Calibri", color: DARK_GREY })] }),
new Paragraph({ bullet: { level: 0 }, children: [new TextRun({ text: "Arrange urgent CT chest/abdomen/pelvis", size: 20, font: "Calibri", color: DARK_GREY })] }),
new Paragraph({ bullet: { level: 0 }, children: [new TextRun({ text: "Plan bone marrow biopsy for staging", size: 20, font: "Calibri", color: DARK_GREY })] }),
new Paragraph({ bullet: { level: 0 }, children: [new TextRun({ text: "Urgent haematology-oncology referral / MDT discussion", bold: true, size: 20, color: RED_ALERT, font: "Calibri" })] }),
new Paragraph({ bullet: { level: 0 }, children: [new TextRun({ text: "If transplant-eligible: initiate HLA typing and donor search early", size: 20, font: "Calibri", color: DARK_GREY })] })
]
})
]})]
}),
// ── REFERENCES ──
new Paragraph({ spacing: { before: 240, after: 0 }, children: [] }),
sectionHeading("References"),
bodyText("1. Goldman-Cecil Medicine International Edition (26th Ed). Chapter 360: HTLV-1 and ATLL."),
bodyText("2. Harrison's Principles of Internal Medicine, 22nd Edition (2025). Chapter: Human T-Cell Lymphotropic Virus."),
bodyText("3. Henry's Clinical Diagnosis and Management by Laboratory Methods. Chapter 34: T-Cell Neoplasms."),
bodyText("4. Stuver R, Horwitz SM, Epstein-Peterson ZD. Treatment of Adult T-Cell Leukemia/Lymphoma. Curr Treat Options Oncol. 2023 Aug. PMID: 37300656."),
bodyText("5. Letafati A et al. Therapeutic approaches for HTLV-1-associated adult T-cell leukemia/lymphoma. Med Oncol. 2023. PMID: 37689806."),
new Paragraph({ spacing: { before: 160 }, children: [new TextRun({ text: "Disclaimer: This report is a clinical decision-support summary generated from laboratory data provided. It does not replace specialist medical judgment. Final diagnosis must integrate clinical findings, HTLV-1 serology, and additional investigations.", size: 18, font: "Calibri", color: "888888", italics: true })] })
]
}]
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync('/home/daytona/workspace/atll-summary/ATLL_Clinical_Summary_Rajendra_Nagare.docx', buffer);
console.log('Document created successfully.');
}).catch(err => {
console.error('Error:', err);
process.exit(1);
});
Running Command
cd /home/daytona/workspace/atll-summary && node create_summary.js 2>&1
Running Command
python3 /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/works…
Running Command
python3 -c "import zipfile; z = zipfile.ZipFile('/home/daytona/workspace/atll-su…
Running Command
ls -lh /home/daytona/workspace/atll-summary/
The clinical summary document is ready for download:
ATLL Clinical Summary Rajendra Nagare
Word Document · DOCX
What's in the document (10 sections):
- Patient Details - demographics, referring physician, lab details
- Diagnosis - highlighted primary diagnosis with ATLL/HTLV-1 notation
- CBC & Peripheral Smear - formatted table with abnormal flags (red/amber), including the initial SMZL misimpression corrected by flow
- Flow Cytometry Immunophenotyping - full marker table, T-cell subset analysis, TRBC1 clonality note, 92.69% CD52 expression
- Immunotherapy Target - CD52/Alemtuzumab panel with clinical context
- Diagnostic Reasoning & Differentials - 5 differentials systematically excluded with rationale; note on atypical CD8-dominant phenotype
- Urgent Pending Investigations - prioritised table (URGENT / High Priority / Standard)
- ATLL Subtype & Prognosis - Shimoyama classification table with survival data, current case highlighted in red
- Treatment Framework - aggressive vs. indolent subtypes, mogamulizumab, alloHCT pathway
- Summary & Action Points - concise narrative + 6 immediate action steps, plus references
The document uses a professional colour-coded layout (red for urgent items, amber for warnings, blue headers) and includes a confidential footer with page numbers - suitable for direct handover at clinic.
This is a shared conversation. Sign in to Orris to start your own chat.