S Simes amputation
Reading File
Finding Sources
Searching the Web
Syme amputation surgical technique indications
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from three major textbooks. Here is a complete overview of the Syme amputation:
Syme Amputation
Definition and History
First described by James Syme in 1843, the Syme amputation is an ankle disarticulation with bone section at the distal tibia and fibula, 0.5-1.0 cm proximal to the ankle joint, passing through the dome of the ankle centrally. The tough, durable plantar skin of the heel flap provides normal weight-bearing tissue on the residual limb.
Indications
- Extensive forefoot or midfoot trauma not amenable to reconstruction
- Non-viable tissue distal to the hindfoot (gangrene, severe infection)
- Diabetic foot with gangrene, Charcot neuroarthropathy, or non-healing ulcers
- Congenital anomalies - fibular hemimelia, congenital pseudarthrosis of tibia (allows direct load transfer and enhanced walking)
- Severe crush injuries or non-reconstructible forefoot/midfoot lesions
Contraindications
- Absent or damaged heel pad (non-supple)
- Poorly vascularized hindfoot tissue flap
- Patent posterior tibial artery is mandatory - it perfuses the heel pad; if it is occluded, the amputation will fail
Advantages
- Preserves limb length and epiphyseal growth plates (especially important in children)
- Allows occasional ambulation without a prosthesis (short distances)
- Creates a stable end-bearing stump using natural plantar skin
- More energy efficient than midfoot amputation despite being more proximal
- Provides a stable gait pattern requiring little prosthetic gait training
- Improved functional independence vs. transtibial amputation when successful
Disadvantages
- Cosmetically unfavorable - the prosthesis must accommodate the flare of the distal tibial metaphysis, making it large and bulbous
- Requires a prosthesis with a removable medial window (classic design) to allow passage of the bulbous stump end
- Higher rates of reamputation and complications in adults vs. children
Surgical Technique (One-Stage - Campbell's Technique 17.9)
The incision uses a single long posterior heel flap:
- Begin the incision at the distal tip of the lateral malleolus, pass it across the anterior aspect of the ankle joint at the level of the distal end of the tibia to a point one fingerbreadth inferior to the tip of the medial malleolus; extend directly plantarward across the sole of the foot
- Extend the dorsal incision to bone; transect tendons under tension so they retract proximally
- Identify and ligate the dorsalis pedis artery; incise the anterior ankle capsule; plantarflex the foot forcibly; transect medial and lateral collateral ligaments - preserving the posterior tibial artery
- Use a bone hook in the talus to pull the foot into greater plantarflexion; begin subperiosteal dissection on the superolateral calcaneus
- Continue dissection posteriorly and medially; transect the Achilles tendon near its calcaneal insertion - protect the posterior tibial artery medially
- Continue subperiosteal dissection inferiorly along the calcaneus until the distal plantar flap is reached; remove the entire foot except the heel flap
- Retract the flap posteriorly; incise periosteum circumferentially 0.5-1.0 cm proximal to the joint line; divide the tibia and fibula so the cut surface is parallel to the ground when standing. Round all sharp corners
- Section the medial and lateral plantar nerves proximal to the bone end
- Pull and section all visible tendons to retract proximally
- Ligate the posterior tibial artery and vein just proximal to the cut edge of the heel flap; ligate the anterior tibial artery in the anterior flap
- Perform minimal debridement of plantar soft tissue; preserve the subcutaneous fat and its septa (this is specialized pressure-tolerant tissue)
- Anchor the heel flap to prevent migration: drill holes through the anterior edge of tibia/fibula and suture the deep fascia through these holes (Wagner technique); alternatives include K-wire skewering or leaving a small calcaneal sliver
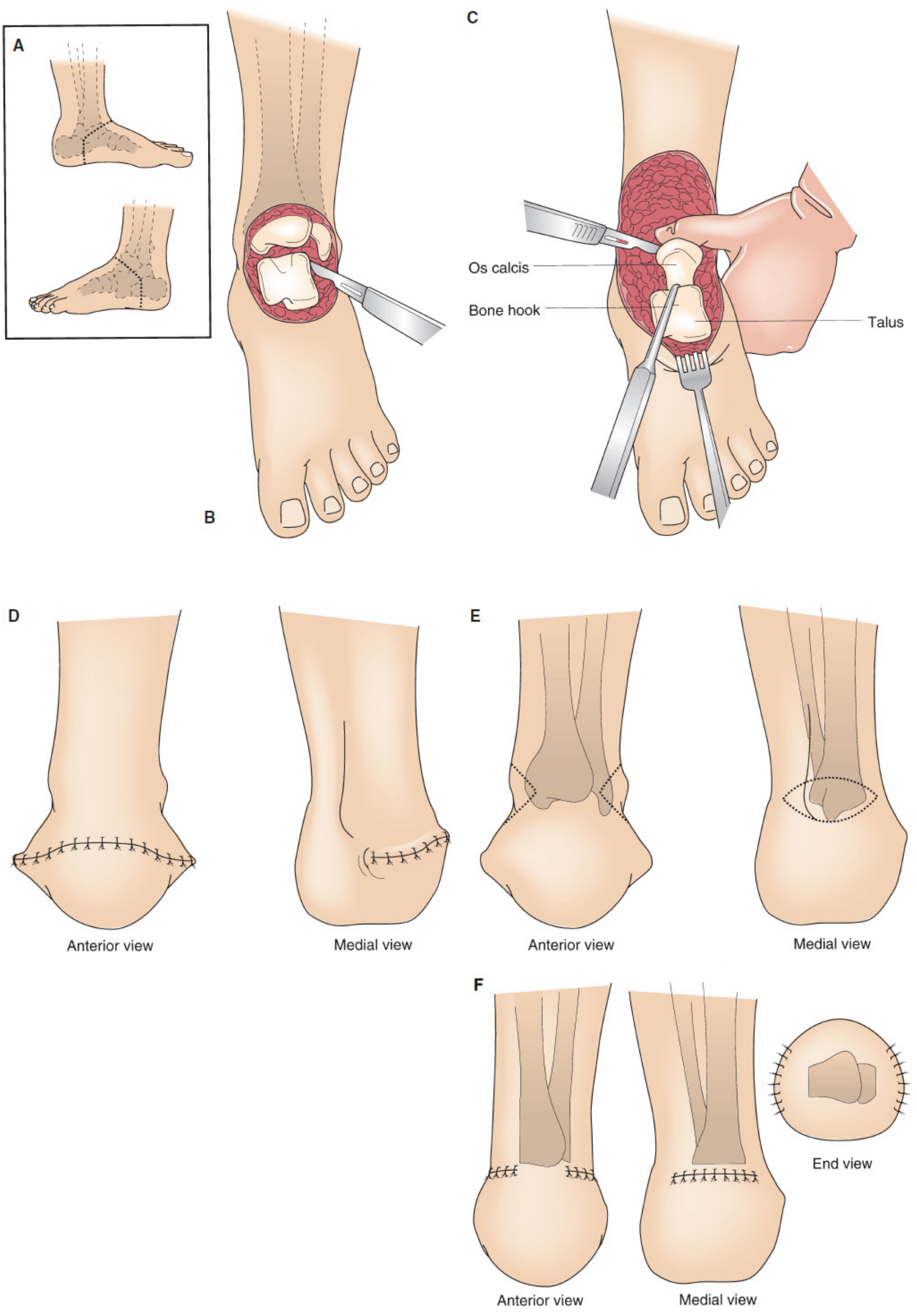
Syme amputation technique: A - Skin incision (inset, one-stage vs two-stage positions); B - Ankle disarticulation with calcaneal dissection; C - Bone hook in talus for traction during calcaneal dissection; D - Wound closure after one-stage procedure (anterior and medial views); E - Malleoli marked for excision in two-stage procedure; F - Final stump after two-stage malleolar resection (anterior, medial, and end views).
Sarmiento Modification
To reduce the bulbous stump and allow fitting with a prosthesis incorporating an expandable socket (rather than a removable window), Sarmiento advised:
- Transection of tibia and fibula approximately 1-1.5 cm proximal to the ankle joint
- Excision of the medial and lateral malleoli
Two-Stage Syme Amputation (for Infected/Gangrenous Feet)
Developed to increase success in patients with gross forefoot infection, particularly diabetic patients.
First Stage - Ankle Disarticulation:
- Incision starts 1 cm distal and 1 cm anterior to each malleolus tip (slightly longer flaps to cover malleoli)
- Ankle is disarticulated as above; the tibial articular cartilage and malleoli are preserved (not resected yet)
- Suction-irrigation tubes are inserted into the wound
- Antibiotic solution is instilled continuously until local and systemic signs of infection resolve
- Wound closed over the irrigation system
Second Stage (after ~6 weeks, once stump is healed):
- Elliptical incisions over the medial and lateral malleoli
- Malleoli and distal flares of the tibia and fibula are transected flush with the ankle joint
- Wound revised and closed - creates the final rectangular stump for prosthetic fitting
Both stages can be safely combined when infection is not adjacent to the heel pad.
Prosthetics
- Classic design: Molded plastic socket with a removable medial window (accommodates the bulbous end), with a solid-ankle cushioned-heel (SACH) foot
- Sarmiento/expandable socket design: For modified stumps with resected malleoli - no window required
- Most patients require a prosthesis for ambulation; rare patients can ambulate without one for short distances
Outcomes
- Children: ~70% participate in sports; excellent outcomes
- Adults: Promising, but higher rates of reamputation and complications
- Achieves improved functional independence compared to transtibial (below-knee) amputation when successful
- Rarely complicated by late residual limb ulcers or tissue breakdown
Related Procedures at the Ankle Level
| Procedure | Key Feature |
|---|---|
| Syme | Ankle disarticulation, heel flap, malleoli excised |
| Boyd | Talectomy + calcaneal shift + calcaneotibial arthrodesis; eliminates heel pad migration risk but more bulbous |
| Pirogoff | Calcaneus sectioned vertically, posterior part rotated forward 90° for tibial arthrodesis; technically most difficult |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, p. 866-868; Mulholland and Greenfield's Surgery 7e, p. 4997-5000; Miller's Review of Orthopaedics 9th Ed
This is a shared conversation. Sign in to Orris to start your own chat.