Thyroid gland physiological action and their the applied physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, authoritative content from Goldman-Cecil, Katzung, and Sabiston. Let me compile the complete, well-structured answer.
Thyroid Gland: Physiological Actions and Applied Physiology
Overview
The thyroid gland is a butterfly-shaped endocrine organ (~10-20 g in adults) with two lobes bridged by an isthmus. It secretes two main hormones - thyroxine (T4) and triiodothyronine (T3) - from thyroid follicular cells, and calcitonin from parafollicular C cells. T4 and T3 are absolutely required for normal human growth, development, and maintenance of physiologic function throughout life.
Part 1: Synthesis and Secretion
Iodine Metabolism
Thyroid hormones are the only iodinated proteins in humans. The recommended daily iodide intake is 150 mcg/day (200 mcg in pregnancy/lactation). Circulating iodide is actively concentrated in the follicular cell by the sodium-iodide symporter (NIS), a 13-transmembrane protein at the basolateral membrane.
Steps of Synthesis
- Iodide uptake - NIS transports iodide into the follicular cell against an electrochemical gradient (inhibited by thiocyanate, perchlorate, pertechnetate)
- Iodide efflux - Pendrin transports iodide to the apical membrane into the colloid (mutation in pendrin causes Pendred syndrome: goiter + deafness)
- Oxidation (organification) - Thyroid peroxidase (TPO) oxidizes iodide to iodine, which iodinates tyrosyl residues on thyroglobulin (Tg), forming monoiodotyrosine (MIT) and diiodotyrosine (DIT)
- Coupling - DIT + DIT → T4; MIT + DIT → T3 (within the Tg molecule)
- Secretion - Tg is endocytosed, lysosomally digested, and T4/T3 are secreted. The T4:T3 secretion ratio is 14:1
The Wolff-Chaikoff block: large doses of iodide transiently inhibit organification - used clinically (e.g., Lugol's iodine pre-thyroidectomy, thyroid storm management)
Part 2: Transport and Peripheral Metabolism
Once secreted, T4 and T3 are tightly bound to plasma proteins:
- Thyroxine-binding globulin (TBG) - principal carrier
- Transthyretin (TTR)
- Albumin
The T4:T3 ratio in circulation is 60:1 because T4 is more tightly protein-bound and has a longer half-life (5-7 days vs ~24 hours for T3).
T3 is the principal biologically active hormone. T4 acts as a prohormone that is converted to T3 peripherally by deiodinases:
| Deiodinase | Location | Function |
|---|---|---|
| Type 1 | Liver, kidney | Converts T4→T3 (activating) and T4→rT3 (inactivating) |
| Type 2 | Pituitary, CNS, skeletal muscle, brown fat | Converts T4→T3 (activating); important for local T3 availability |
| Type 3 | Fetal CNS, sensory organs | Inactivates T4→rT3 and T3→T2 |
Thyroid hormones enter target cells via specific transporters, the most important being monocarboxylate transporter 8 (MCT8). Mutation in MCT8 causes Allan-Herndon-Dudley syndrome (X-linked severe neurologic disorder from failure of thyroid hormone to cross the blood-brain barrier in utero).
Part 3: Mechanism of Action
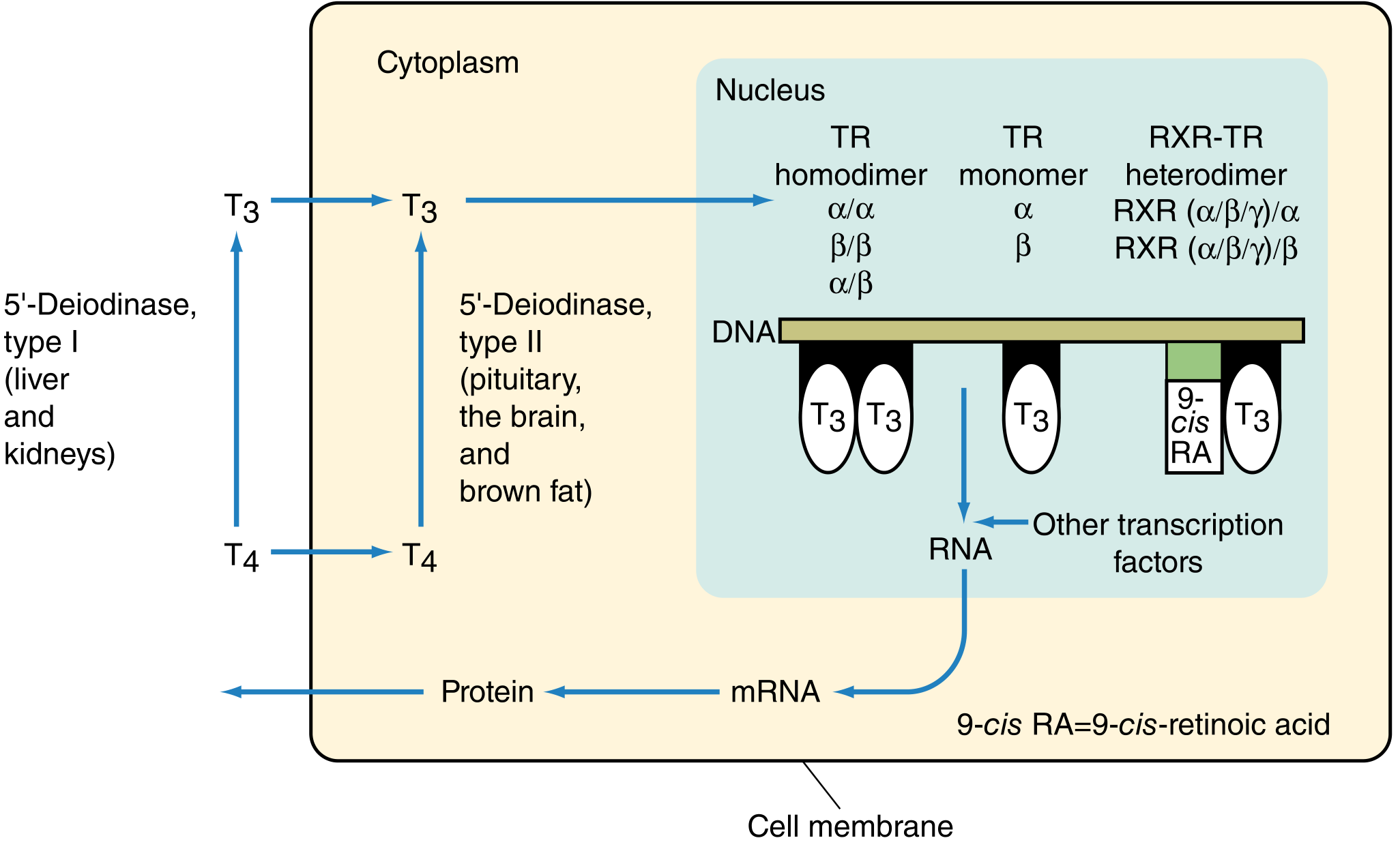
T4 is converted to T3 in the cytoplasm. T3 then enters the nucleus and binds to thyroid hormone receptors (TR), which are nuclear receptor family members with a DNA-binding domain and a ligand-binding domain. TRs bind to thyroid hormone response elements (TREs) in DNA as:
- TR homodimers (TRα/α, TRβ/β, TRα/β)
- TR monomers
- Heterodimers with retinoid X receptor (RXR)
This activates RNA transcription → mRNA → protein synthesis (e.g., Na+/K+-ATPase). This explains the latency of thyroid hormone action (hours to days).
Receptor isoforms and their tissue-specific roles:
- TRβ2 - hypothalamus and pituitary; controls TSH secretion (negative feedback)
- TRβ1 - liver; regulates cholesterol and fatty acid metabolism
- TRα1 - heart, GI tract, bone; regulates cardiac function, heart rate, intestinal motility, bone metabolism, and growth
Thyroid hormone receptors are most abundant in pituitary, liver, kidney, heart, skeletal muscle, lung, and intestine. The spleen and testes have very few receptors. The affinity of TR for T3 is about 10 times greater than for T4, reflecting T3's greater biological potency.
Part 4: Hypothalamic-Pituitary-Thyroid (HPT) Axis and Regulation
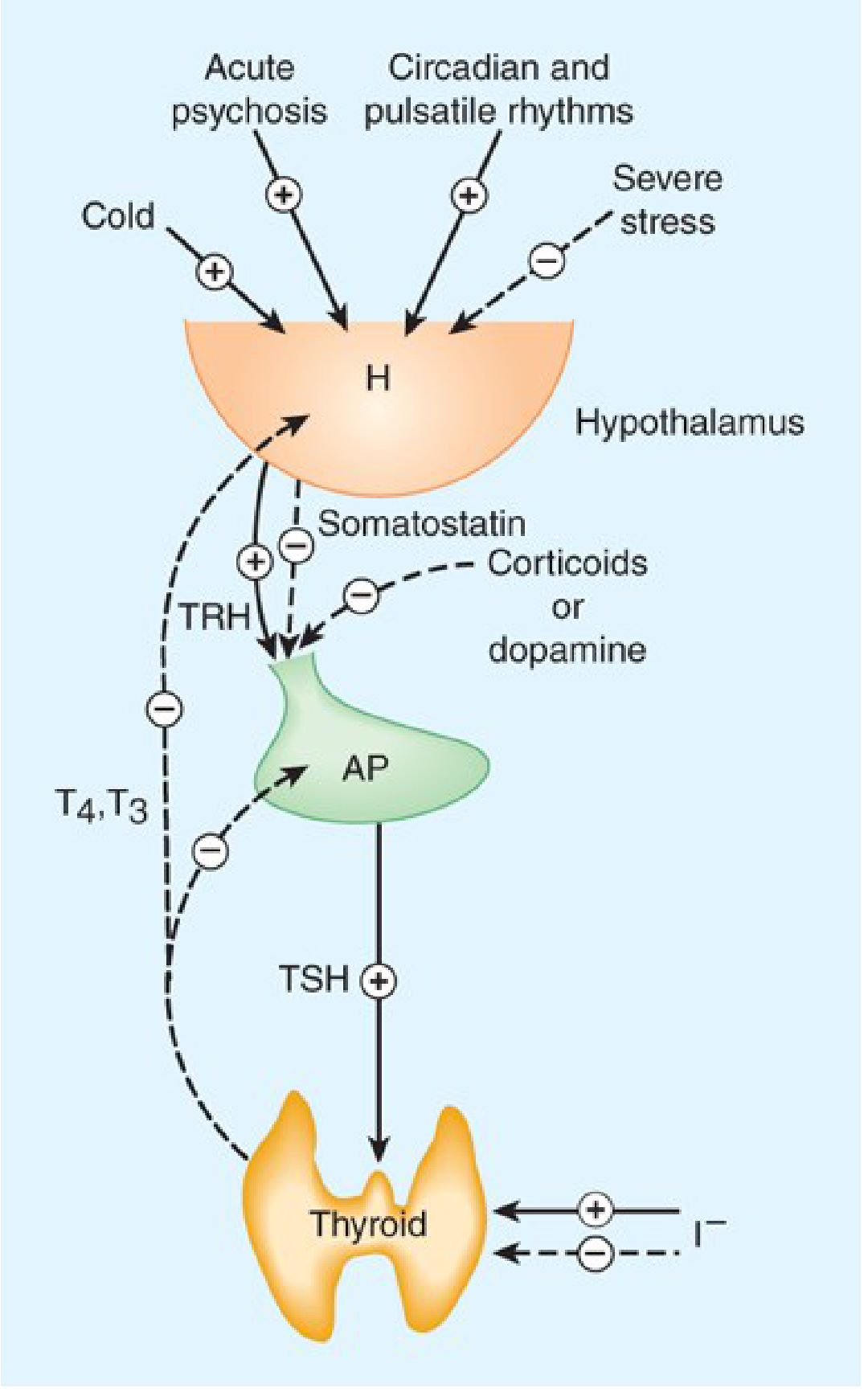
- TRH (tripeptide, from hypothalamic paraventricular nucleus) → stimulates anterior pituitary thyrotropes → TSH release
- TSH binds TSHR on follicular cells → increases iodide uptake, hormone synthesis, and secretion
- T3/T4 feed back negatively at both hypothalamus (inhibit TRH) and pituitary (inhibit TSH synthesis/release)
- TSH levels rise when thyroid hormones are low and are suppressed when high → TSH is the most sensitive screening test for thyroid dysfunction
Modifiers of the HPT axis:
- Cold exposure → stimulates TRH (activates axis)
- Acute psychosis → activates axis
- Severe stress, somatostatin, dopamine, corticoids → inhibit TSH secretion
- Large doses of iodide → inhibit T3/T4 production (Wolff-Chaikoff block)
Part 5: Physiological Actions by System
1. Metabolic / Calorigenic Effects
- Thyroid hormone is the primary driver of basal metabolic rate (BMR)
- Binds mitochondrial receptors → increases ATP production, O2 consumption, and glucose oxidation → releases heat (calorigenic effect)
- Stimulates lipid and carbohydrate metabolism
- Increases Na+/K+-ATPase activity in virtually all cells
2. Cardiovascular System
- Increases cardiac contractility (positive inotropy) and heart rate (positive chronotropy) via TRα1
- Decreases peripheral vascular resistance → increases cardiac output and widens pulse pressure
- Increases sensitivity to catecholamines (upregulates β-adrenergic receptors)
3. Growth and Development
- Fetal/neonatal brain development is the most critical effect - deficiency causes cretinism (irreversible intellectual disability, deafness, spasticity)
- Critical for skeletal maturation and epiphyseal development
- Synergizes with growth hormone (GH) for linear growth
- Promotes myelination of the CNS
4. Nervous System
- Maintains normal reflexes and mental function
- Increases sensitivity of CNS to adrenergic stimulation
5. Gastrointestinal Tract
- Increases GI motility (via TRα1)
- Stimulates appetite
6. Bone
- Regulates bone metabolism via TRα1
- Excess thyroid hormone causes increased bone turnover and osteoporosis
7. Reproductive System
- Normal reproductive function is highly dependent on thyroid hormone
- Both hypothyroidism and hyperthyroidism impair fertility
8. Calcitonin (from parafollicular C cells)
- Decreases serum calcium by:
- Inhibiting osteoclast activity / stimulating osteoblasts
- Decreasing gut calcium absorption
- Increasing urinary calcium excretion
- Release triggered by elevated serum calcium
- Clinically used to treat hypercalcemia and Paget's disease
- Note: calcitonin deficiency does not cause clinically significant hypercalcemia (unlike PTH deficiency), so its physiologic role in humans is minor
Part 6: Applied Physiology
Comparison of Thyrotoxicosis vs. Hypothyroidism
| System | Thyrotoxicosis (Excess) | Hypothyroidism (Deficiency) |
|---|---|---|
| Skin | Warm, moist, sweating, heat intolerance; fine thin hair; Plummer's nails | Pale, cool, puffy, yellowish; dry/brittle hair and nails |
| Eyes/Face | Lid retraction, exophthalmos, periorbital edema (Graves) | Drooping lids, loss of lateral eyebrows, puffy face, macroglossia, hoarseness |
| CVS | Tachycardia, high output, arrhythmias, increased pulse pressure, angina | Bradycardia, low output, prolonged PR, low voltage ECG, pericardial effusion |
| Respiratory | Dyspnea, decreased vital capacity | Pleural effusions, hypoventilation, CO2 retention, sleep apnea |
| GI | Increased motility, diarrhea, weight loss despite increased appetite | Constipation, weight gain |
| CNS/Neuromuscular | Anxiety, tremor, hyperreflexia, insomnia | Slow mentation, fatigue, depression, delayed tendon reflexes |
| Metabolic | Elevated BMR, heat intolerance, weight loss | Decreased BMR, cold intolerance, weight gain |
| Bone | Osteoporosis, hypercalcemia | Normal or elevated TSH-driven bone effects |
| Reproductive | Menstrual irregularity, infertility, gynecomastia | Menorrhagia, infertility, decreased libido |
(Katzung's Basic and Clinical Pharmacology, 16th Ed.)
Clinically Important Applied Points
| Scenario | Applied Physiology |
|---|---|
| Cretinism | Congenital hypothyroidism (1 in 3500 births) from thyroid agenesis, dyshormonogenesis, or maternal iodine deficiency. Irreversible brain damage if untreated within weeks of birth. Neonatal TSH screening is life-saving. |
| Myxedema coma | Extreme hypothyroidism with hypothermia, bradycardia, hypoventilation, and altered consciousness. Treat with IV T3/T4 + hydrocortisone (adrenal insufficiency may coexist) |
| Thyroid storm | Life-threatening hyperthyroidism with fever, tachyarrhythmia, CNS dysfunction. Treat with PTU (blocks synthesis and peripheral T4→T3 conversion), beta-blockers (control adrenergic symptoms), Lugol's iodine (Wolff-Chaikoff block), and glucocorticoids |
| Pregnancy | Maternal T4 requirement rises ~30-50% in first trimester (hCG has weak TSH-like activity). Maternal T4 crosses placenta before fetal thyroid function starts (12 weeks). Untreated hypothyroidism causes fetal neurodevelopmental defects. |
| Graves' disease | TSH-receptor stimulating antibodies (TSI/TSH-R Ab[stim]) continuously stimulate the gland, bypassing normal negative feedback. Orbital fibrocytes also express TSH receptors, causing ophthalmopathy. |
| Subclinical hypothyroidism | T4/T3 within normal range but TSH elevated, reflecting that the individual's genetic set point is not being met. Treat if TSH >10 mIU/L or if symptomatic. |
| Sick euthyroid syndrome | Severe illness causes decreased T3 (less peripheral T4→T3 conversion) and elevated rT3. TSH may be low or normal. Do not treat - it is a protective adaptation. |
| Wolff-Chaikoff effect | Large iodide loads transiently block organification. Used clinically before thyroid surgery and in thyroid storm. Most euthyroid individuals "escape" this block after 1-2 weeks; those with Hashimoto thyroiditis may not escape, resulting in hypothyroidism. |
| Pendred syndrome | Biallelic SLC26A4 mutations cause sensorineural deafness + goiter (defective pendrin prevents cochlear and thyroid iodide transport) |
Sources: Goldman-Cecil Medicine (p. 2428-2435) | Sabiston Textbook of Surgery (p. 1490) | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Harrison's Principles of Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.