I have all the information I need. Now let me compose a comprehensive answer covering leiomyoma, leiomyosarcoma (myometrial tumors), and the cervical stump.
Myometrial Tumours
The myometrium gives rise to two major smooth muscle tumours: the benign leiomyoma and the malignant leiomyosarcoma.
1. LEIOMYOMA (Fibroid / Uterine Fibroid)
Definition
A leiomyoma is a benign smooth muscle neoplasm of the myometrium. It is one of the most common tumours in women and is often called a "fibroid" (though it contains very little fibrous tissue).
Etiology & Pathogenesis
| Factor | Detail |
|---|
| Hormonal | Estrogen and progesterone stimulate growth; tumours shrink after menopause |
| Genetic | Rearrangements of chromosomes 6 and 12 |
| Molecular | MED12 mutations in up to 70% of cases (MED12 regulates RNA polymerase II-mediated transcription) |
| Race | More common in African-Caribbean women |
| Hereditary | Germline loss-of-function mutations in the fumarate hydratase (FH) gene cause an autosomal syndrome of multiple cutaneous + uterine leiomyomas + renal cell carcinoma |
- Robbins & Kumar Basic Pathology, Uterine Leiomyoma section
- Bailey and Love's Short Practice of Surgery 28th Ed, p.1609
Pathology - Classification by Location
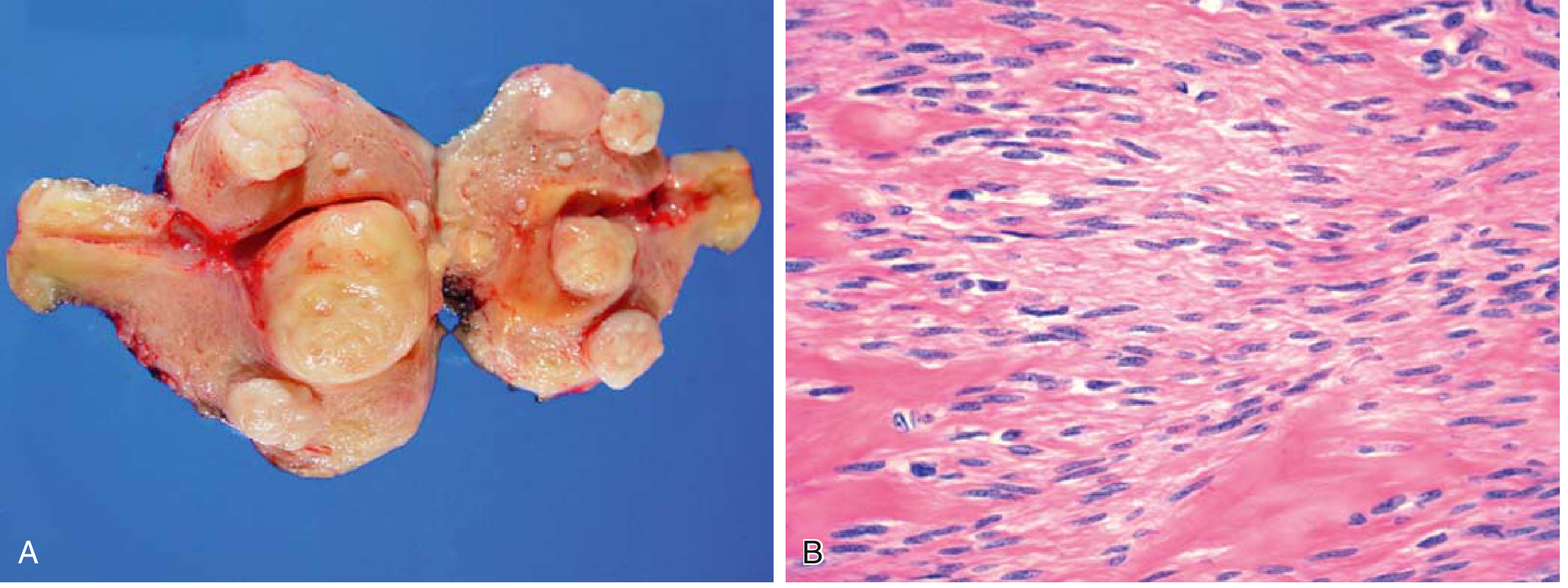
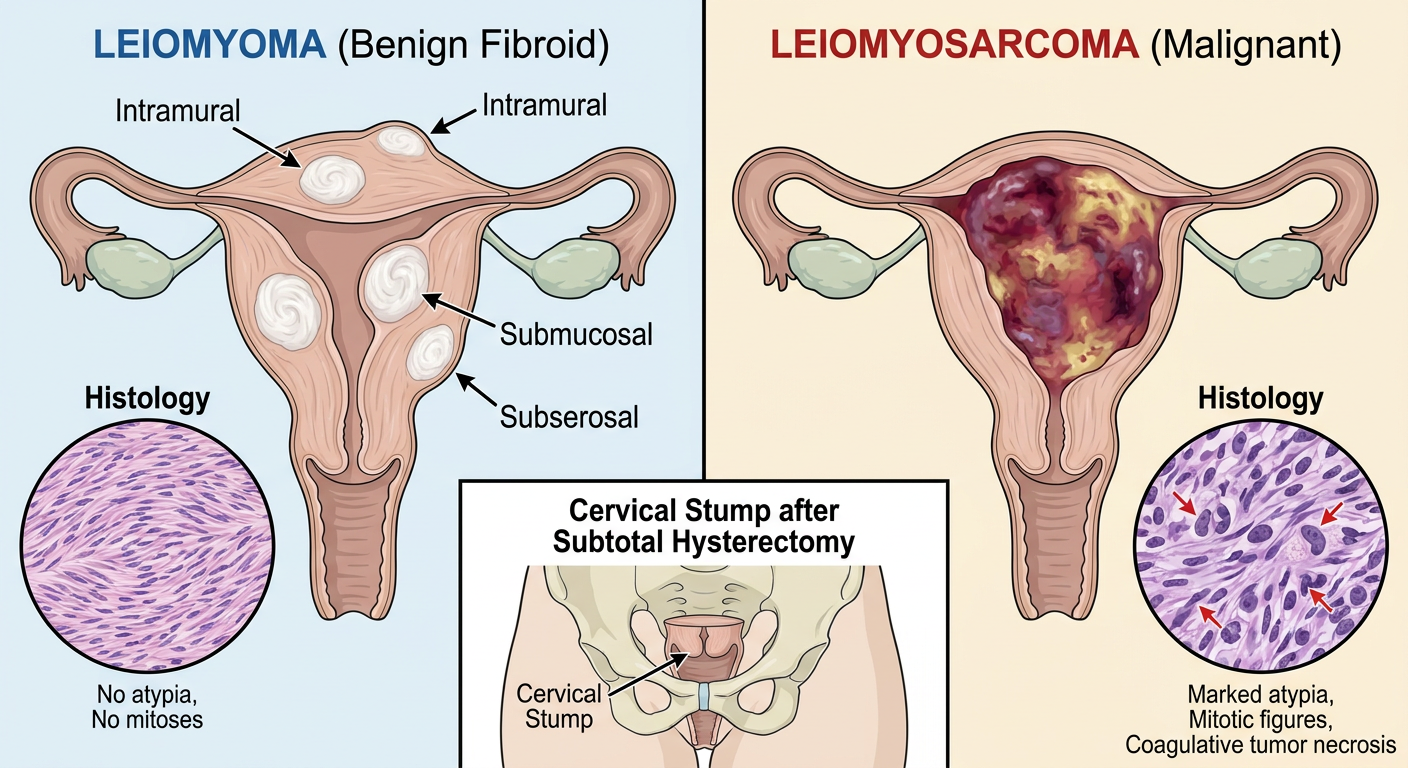
Leiomyomas are typically sharply circumscribed, firm, gray-white masses with a whorled cut surface. They may be single or, more commonly, multiple.
| Type | Location | Features |
|---|
| Intramural | Embedded in myometrium | Most common; pressure symptoms, may distort cavity |
| Submucosal | Beneath endometrium | Heavy periods, infertility, recurrent pregnancy loss; if pedunculated may extrude through cervical os |
| Subserosal | Below serosa | Pressure symptoms; pedunculated forms can mimic ovarian mass ("parasitic leiomyomas" when they attach to other organs and develop independent blood supply) |
| Cervical / Broad ligament | Rare sites | Rare locations |
Histology: Bundles of smooth muscle cells resembling normal myometrium, with minimal atypia and extremely rare mitotic figures. Foci of fibrosis, calcification, and degenerative softening ("degeneration") may be present.
Degenerations of Leiomyoma
| Type | Mechanism |
|---|
| Hyaline | Most common; collagen replaces smooth muscle |
| Cystic | Liquefaction of hyaline areas |
| Calcific | Dystrophic calcification (seen in postmenopausal women; "womb stones") |
| Red (Carneous) | Venous thrombosis → infarction; seen in pregnancy - presents with acute pain |
| Fatty (Lipomatous) | Rare |
| Myxoid | Myxoid change |
| Sarcomatous | Malignant transformation to leiomyosarcoma - extremely rare (<1%) |
Clinical Features
- Menorrhagia (most common symptom), with or without metrorrhagia
- Pelvic pressure / pain, urinary frequency/retention, constipation
- Infertility, recurrent pregnancy loss (submucosal type)
- Acute pain from torsion of pedunculated fibroid or red degeneration in pregnancy
- Many are asymptomatic - discovered incidentally
Investigations
- Pelvic ultrasound - first line, high sensitivity and specificity
- MRI - if USS inconclusive or declined; gold standard for mapping
- LDH and its isozymes - help differentiate leiomyosarcoma from degenerated leiomyoma
- Hysteroscopy - for submucosal fibroids
Treatment
| Category | Options |
|---|
| Conservative | Watchful waiting if asymptomatic |
| Medical | Tranexamic acid, NSAIDs; GnRH agonists to shrink before surgery |
| Hormonal | Progesterone-releasing IUS, combined oral contraceptive |
| Surgical (uterus-sparing) | Myomectomy (open, laparoscopic, hysteroscopic) |
| Surgical (definitive) | Hysterectomy (total or subtotal) |
| Interventional | Uterine artery embolisation |
2. LEIOMYOSARCOMA
Definition
A malignant smooth muscle tumour arising from the myometrium (or endometrial stromal precursor cells). It is distinct from leiomyoma and does not arise from it in the vast majority of cases.
Epidemiology & Pathogenesis
- Uncommon - accounts for 10-20% of soft tissue sarcomas overall
- More common in postmenopausal women (contrast to leiomyoma which occurs before menopause)
- Almost always solitary (contrast to leiomyoma which is often multiple)
- Complex, highly variable karyotypes with chromosomal deletions; defects in genomic stability
- MED12 mutations present in ~30% (vs 70% in leiomyoma)
- Robbins & Kumar Basic Pathology, Leiomyosarcoma section
Pathology
| Feature | Description |
|---|
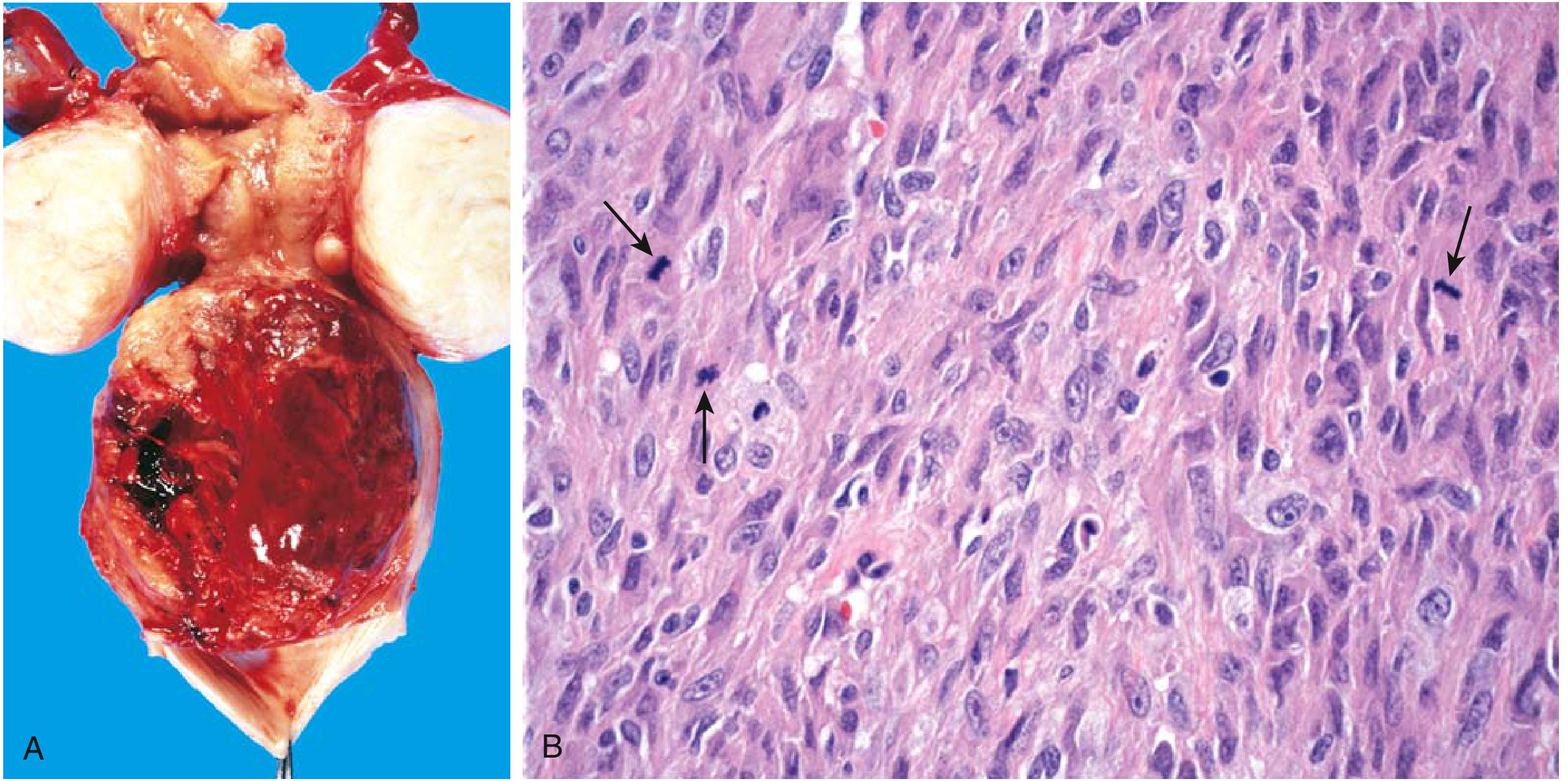
| Gross | Soft, hemorrhagic, necrotic mass; typically solitary |
| Histology | Ranges from tumours resembling leiomyoma to wildly anaplastic neoplasms |
Diagnostic Triad (all three must be assessed):
- Tumor coagulative necrosis
- Cytologic atypia
- Mitotic activity (increased mitotic rate)
Note: Increased mitotic activity alone can be seen in benign smooth muscle tumours (especially in young women), so all three features together are needed to diagnose malignancy.
Immunohistochemistry: Smooth muscle proteins (smooth muscle actin, desmin, h-caldesmon) confirm smooth muscle differentiation.
Spread & Prognosis
- Local recurrence is common following surgery
-
50% eventually metastasize, primarily to the lungs
- Poor prognosis; retroperitoneal/deep tumours are particularly difficult to control
Leiomyoma vs Leiomyosarcoma - Key Differences
| Feature | Leiomyoma | Leiomyosarcoma |
|---|
| Nature | Benign | Malignant |
| Number | Multiple | Solitary |
| Age | Premenopausal | Postmenopausal |
| Gross | Firm, whorled, white | Soft, hemorrhagic, necrotic |
| Necrosis | Absent | Present (coagulative) |
| Atypia | Minimal | Marked |
| Mitoses | Very rare | Frequent |
| MED12 mutation | ~70% | ~30% |
| Transformation from leiomyoma | Extremely rare (<1%) | Mostly de novo |
THE CERVICAL STUMP
What is a Cervical Stump?
A cervical stump is the remnant cervix left behind after a subtotal (supracervical) hysterectomy - an operation in which only the uterine body (corpus) is removed while the cervix is intentionally left in place.
"A supracervical or 'subtotal' hysterectomy is the removal of the uterine corpus while leaving the cervix in situ."
- Sabiston Textbook of Surgery
Why is a Subtotal Hysterectomy Performed (Creating a Stump)?
- Technically easier and faster, especially in cases with dense adhesions or severe endometriosis where total hysterectomy is hazardous
- Historically popular; sometimes driven by patient preference (belief in preserved pelvic floor support and sexual function)
- May be performed laparoscopically via morcellation (cutting the uterine body into pieces for removal through small ports)
Surgical Procedure
- Steps identical to total hysterectomy up to the point of uterine artery ligation at the level of the internal cervical os
- The uterine body is then amputated from the cervix using scissors, electrocautery, or ultrasonic energy
- The remaining endocervix and cervical stump are cauterised
- The stump is closed with figure-of-eight sutures for hemostasis
Important Considerations After Leaving a Cervical Stump
| Issue | Detail |
|---|
| Cervical cancer screening | Must continue per guidelines (Pap smears / HPV testing) because the transformation zone of the cervix is still present |
| Contraindication | Subtotal hysterectomy is contraindicated if there is malignant or premalignant disease of the uterus or cervix |
| Cancer of the Cervical Stump | Cervical carcinoma can develop in the stump just as in an intact cervix |
Cancer of the Cervical Stump
This is a cervical carcinoma arising in the residual cervix after a prior subtotal hysterectomy. It is managed similarly to regular cervical carcinoma but with important differences:
- Radical trachelectomy (surgical removal of the stump) is preferred over pelvic irradiation in many cases, because intestinal adhesions to the residual cervix increase the risk of bowel complications from radiation
- Laparoscopic and robotic radical trachelectomy approaches have been reported
- "Cut-through" scenarios - e.g. if endometrial cancer is later discovered in the subtotal hysterectomy specimen, robotic radical trachelectomy of the remaining cervix may be required
- Berek & Novak's Gynecology, Cancer of the Cervical Stump
- Sabiston Textbook of Surgery, Supracervical Hysterectomy
Summary Table: Cervical Stump
| Aspect | Detail |
|---|
| Definition | Residual cervix after subtotal hysterectomy |
| Synonym | Supracervical / subtotal hysterectomy remnant |
| Screening required | Yes - Pap smear continues |
| Risk | Cancer of the cervical stump |
| Management of stump cancer | Radical trachelectomy (surgical) preferred over radiotherapy due to adhesion risk |
| Contraindication to leaving stump | Pre-existing cervical/uterine malignancy or premalignancy |
Morcellation and the Stump
During laparoscopic subtotal hysterectomy, the uterine body is removed by morcellation (breaking it into small pieces). A recognized risk is parasitic spread of tissue - if an occult leiomyosarcoma was present, morcellation can disseminate malignant cells throughout the peritoneal cavity. This is why the FDA has issued warnings about power morcellation, particularly in postmenopausal women where leiomyosarcoma risk is higher.
- Bailey and Love's Short Practice of Surgery 28th Ed, Morcellation section