Classify general anesthetics. Describe the pharmacology of intravenous anesthetics
Reading File
Finding Sources
Finding Sources
Searching the Web
classification general anesthetics intravenous pharmacology mechanism 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Mbbs 2nd yr refer kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Katzung (the pharmacology equivalent of KDT) and Lippincott. I have enough to write a complete, detailed MBBS 2nd year answer. Let me compile everything now.
General Anesthetics — Classification & Pharmacology of IV Agents
(Based on Katzung's Basic & Clinical Pharmacology 16e, Lippincott Illustrated Reviews: Pharmacology, Miller's Anesthesia 10e, and Barash's Clinical Anesthesia 9e — the standard references equivalent to KDT for this topic)
Note: KDT (K.D. Tripathi's Essentials of Medical Pharmacology) is not in the digital library, but all content below maps directly to KDT's Chapter on General Anaesthetics and is drawn from equivalent standard pharmacology references used in MBBS.
I. CLASSIFICATION OF GENERAL ANESTHETICS
General anesthesia produces five primary effects: unconsciousness, amnesia, analgesia, inhibition of autonomic reflexes, and skeletal muscle relaxation. No single agent produces all five ideally — hence balanced anesthesia using combinations is standard practice.
A. By Route of Administration
| Category | Agents |
|---|---|
| Inhalational (volatile liquids) | Halothane, Isoflurane, Sevoflurane, Desflurane, Enflurane |
| Inhalational (gases) | Nitrous oxide (N₂O) |
| Intravenous | Propofol, Thiopental (barbiturate), Ketamine, Etomidate, Midazolam, Dexmedetomidine |
B. By Chemical Class
Inhalational agents:
- Halogenated volatile liquids (ethers): Isoflurane, Sevoflurane, Desflurane, Enflurane
- Halogenated alkane: Halothane
- Inorganic gas: Nitrous oxide
Intravenous agents:
| Class | Drugs |
|---|---|
| Alkylphenol | Propofol |
| Barbiturates | Thiopental sodium, Methohexital |
| Phencyclidine derivative | Ketamine |
| Imidazole derivative | Etomidate |
| Benzodiazepines | Midazolam, Diazepam, Lorazepam, Remimazolam |
| α₂-adrenoceptor agonist | Dexmedetomidine |
| Opioids (adjuncts) | Fentanyl, Remifentanil, Alfentanil |
C. Stages of Anesthesia (Guedel's Classification — for ether)
- Stage I — Analgesia (conscious, responds to commands)
- Stage II — Excitement/Delirium (unconscious, irregular breathing, risk of laryngospasm)
- Stage III — Surgical anesthesia (Planes 1–4: regular breathing → apnea)
- Stage IV — Medullary depression (respiratory and cardiovascular collapse → death)
Modern IV agents pass through Stage II so rapidly it is clinically imperceptible.
II. PHARMACOLOGY OF INTRAVENOUS ANESTHETICS
Properties of the Ideal IV Anesthetic
- Rapid onset (within one arm-brain circulation time)
- Rapid metabolism to inactive metabolites
- Short context-sensitive half-time (suitable for infusion)
- Minimal cardiovascular and respiratory depression
- Hypnosis + amnesia
- No histamine release, non-teratogenic, non-carcinogenic
1. PROPOFOL (2,6-diisopropylphenol)
Mechanism of action: Enhancement of GABA_A receptor–mediated chloride ion currents → neuronal hyperpolarization → CNS depression. Formulated as a 1% lipid emulsion (soybean oil/egg phosphatide).
Pharmacokinetics:
- Onset: 40 seconds (rapid, within one arm-brain circulation)
- Duration after single bolus: 8–10 minutes (redistribution from brain to muscle)
- Highly protein-bound (97–98%), rapidly metabolized hepatically to inactive glucuronide conjugates
- Context-sensitive half-time is brief even after prolonged infusion — this is propofol's key pharmacokinetic advantage, making it ideal for TIVA (Total IV Anesthesia) maintenance
Induction dose: 1.5–2.5 mg/kg IV; Maintenance: 100–200 mcg/kg/min infusion
CNS effects:
- Dose-dependent hypnosis; no intrinsic analgesia
- ↓ Cerebral blood flow, ↓ CMRO₂, ↓ ICP, ↓ intraocular pressure
- Antiemetic effect (unique property — anti-nausea even at sub-hypnotic doses)
- Anticonvulsant
CVS effects: ↓ BP (predominantly via ↓ SVR/vasodilation); mild ↓ cardiac output
Respiratory: Dose-dependent respiratory depression; apnea on induction; ↓ tidal volume
Adverse effects:
- Pain on injection (into small veins)
- Propofol infusion syndrome (rare, with prolonged high-dose infusion): metabolic acidosis, rhabdomyolysis, cardiac failure
- No analgesic property — must be combined with an opioid
Uses: Induction and maintenance of anesthesia; procedural sedation; TIVA; ICU sedation; treatment of refractory status epilepticus
2. THIOPENTAL SODIUM (Barbiturate)
Mechanism: Acts on GABA_A receptor (binds to β subunit) → ↑ duration of Cl⁻ channel opening → CNS depression. Also acts on cortical and brainstem GABA inhibitory pathways.
Pharmacokinetics:
- Ultra-lipid-soluble → rapid onset (10–20 seconds)
- Highly alkaline (pH 10.5) — sodium salt in water; incompatible with acidic drugs (e.g., neuromuscular blockers, opioids)
- Redistribution from brain to muscle → termination of effect after single dose
- Long context-sensitive half-time (accumulates with repeated/prolonged dosing) — NOT suitable for infusion maintenance
- Slowly metabolized in liver; excreted renally
Induction dose: 3–5 mg/kg IV
CNS: Rapid, smooth loss of consciousness; ↓ ICP; cerebral protection (reduces CMRO₂); no analgesia
CVS: Moderate ↓ BP (peripheral vasodilation + mild myocardial depression); ↑ HR (reflex tachycardia)
Respiratory: ↓ respiratory drive; apnea after induction dose; laryngeal reflexes relatively preserved
Adverse effects:
- Contraindicated in acute intermittent porphyria (induces δ-ALA synthase, precipitates attack)
- Intraarterial injection → severe arterial spasm, gangrene
- Extravasation → tissue necrosis (highly alkaline)
- Laryngospasm (compared to propofol)
Uses: Induction of anesthesia; ↓ ICP in neurosurgery; cerebral protection; status epilepticus; now largely replaced by propofol
3. KETAMINE
Mechanism: Noncompetitive antagonist of NMDA (N-methyl-D-aspartate) glutamate receptors → blocks excitatory neurotransmission. Produces dissociative anesthesia — a state where the patient appears disconnected from the environment with profound analgesia yet may have open eyes and active protective reflexes.
Pharmacokinetics:
- Lipophilic → rapid onset (IV: 30–60 sec; IM: 3–4 min)
- Redistributes to peripheral tissues (similar to thiopental)
- Short context-sensitive half-time
- Metabolized hepatically to norketamine (active, ~1/3 potency)
- Can be given IV, IM, oral, rectal, epidural — versatile routes
Induction dose: 1–2 mg/kg IV or 4–6 mg/kg IM
CNS:
- Dissociative anesthesia + profound analgesia
- ↑ Cerebral blood flow, ↑ ICP → contraindicated when ICP is raised
- Psychomimetic effects (hallucinations, vivid dreams, emergence reactions) — especially in adults; reduced by pre-treatment with benzodiazepines
CVS (unique — stimulatory):
- ↑ BP, ↑ HR, ↑ cardiac output — via central sympathetic stimulation
- Beneficial in hypovolemic shock and trauma patients
- Contraindicated in hypertensive patients and those with ischemic heart disease
Respiratory:
- Minimal respiratory depression; preserves airway reflexes
- Potent bronchodilator — preferred in asthmatics and bronchospasm
- Hypersalivation → premedication with atropine/glycopyrrolate recommended; risk of laryngospasm
Uses: Induction in haemodynamically unstable/trauma patients; asthmatic patients; emergency field anesthesia; pediatric anesthesia; sub-anesthetic dose for analgesia (opioid-sparing); procedural sedation; treatment-resistant depression (esketamine)
4. ETOMIDATE
Mechanism: Imidazole derivative; acts on GABA_A receptor (specifically β₂ and β₃ subunits) → enhances inhibitory transmission.
Key feature: Hemodynamic stability — minimal effect on blood pressure and cardiac output, making it the preferred induction agent in cardiovascularly unstable patients and elderly patients.
Pharmacokinetics: Rapid onset; redistribution terminates effect; hepatic ester hydrolysis
Induction dose: 0.2–0.4 mg/kg IV
CNS: Hypnosis, no analgesia; ↓ ICP, ↓ CMRO₂; anticonvulsant (and can cause myoclonic jerks)
CVS: Minimal change in HR and BP — hemodynamically stable
Respiratory: Minimal respiratory depression
Adverse effects:
- Adrenocortical suppression — inhibits 11β-hydroxylase → ↓ cortisol and aldosterone synthesis (even after a single induction dose; clinically significant with prolonged infusion)
- Myoclonus (involuntary muscle movements) on induction
- Pain on injection
- Nausea/vomiting (higher incidence than propofol)
Uses: Induction in cardiac/haemodynamic compromise; elderly patients; rapid sequence intubation; neurosurgery (↓ ICP without ↓ BP)
5. BENZODIAZEPINES (Midazolam, Diazepam, Lorazepam)
Mechanism: Bind to BDZ site on GABA_A receptor → ↑ frequency of Cl⁻ channel opening (barbiturates increase duration) → enhanced GABA inhibition. Specific antagonist: Flumazenil.
Effects: Anxiolysis, anterograde amnesia, sedation, hypnosis, anticonvulsant, muscle relaxation
Midazolam (most commonly used IV):
- Water-soluble at acidic pH; lipid-soluble at physiological pH
- Rapid onset; shorter duration than diazepam
- Induction dose: 0.05–0.15 mg/kg IV
- Used for premedication, procedural sedation, and induction
- Metabolized by CYP3A4 → 1-hydroxymidazolam (active)
Remimazolam — newest benzodiazepine; ultra-short duration due to metabolism by plasma esterases (context-sensitive half-time independent of infusion duration)
CVS: Mild ↓ BP, mild ↓ HR
Respiratory: Mild to moderate depression; apnea risk with opioid combination
6. DEXMEDETOMIDINE
Mechanism: Highly selective α₂-adrenoceptor agonist (α₂:α₁ selectivity = 1600:1) acting on locus coeruleus → sedation, anxiolysis, analgesia, sympatholysis.
Unique property: Sedation WITHOUT significant respiratory depression (patients remain arousable and cooperative)
Effects: Sedative, analgesic, anxiolytic, sympatholytic; ↓ volatile anesthetic and opioid requirements; blunts haemodynamic responses to laryngoscopy and intubation; reduces emergence delirium (especially in children)
CVS: ↓ HR, ↓ BP (bradycardia and hypotension are main adverse effects)
Uses: ICU sedation in mechanically ventilated patients; adjunct to general anesthesia; procedural sedation; paediatric emergence delirium prevention
III. SUMMARY COMPARISON TABLE
| Drug | Class | Mechanism | Onset | CVS Effect | Resp. Depression | Special Feature |
|---|---|---|---|---|---|---|
| Propofol | Alkylphenol | GABA-A ↑ | 40 sec | ↓ BP/SVR | Moderate | Antiemetic; TIVA |
| Thiopental | Barbiturate | GABA-A ↑ | 10–20 sec | Moderate ↓BP | Moderate | C/I in porphyria |
| Ketamine | Phencyclidine | NMDA block | 30–60 sec | ↑ BP/HR | Minimal | Bronchodilator; dissociative |
| Etomidate | Imidazole | GABA-A ↑ | 15–45 sec | Minimal | Minimal | ↓ Cortisol; CVS stable |
| Midazolam | Benzodiazepine | GABA-A ↑ freq | Slow (1–5 min) | Mild ↓BP | Mild–moderate | Flumazenil reversal |
| Dexmedetomidine | α₂ agonist | α₂ receptor | Slow (infusion) | ↓ HR, ↓ BP | None significant | Arousable sedation |
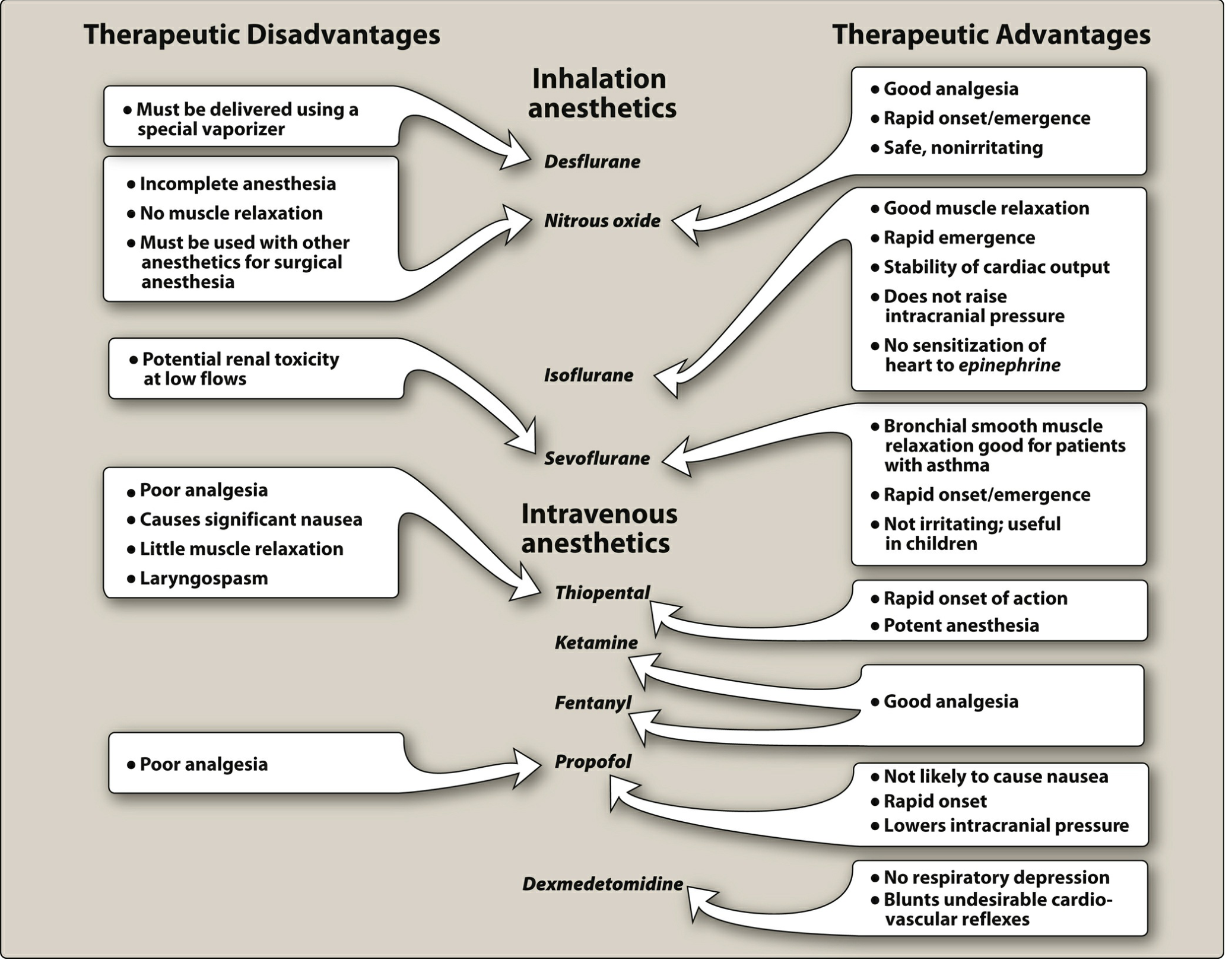
IV. DIAGRAM — Advantages & Disadvantages of Anesthetic Agents
(Lippincott Illustrated Reviews: Pharmacology)
Key Exam Points for MBBS 2nd Year
- Propofol = drug of choice for TIVA; antiemetic; short context-sensitive half-time
- Thiopental = contraindicated in porphyria; causes intraarterial spasm/gangrene if injected intraarterially
- Ketamine = NMDA antagonist → dissociative anesthesia; stimulates CVS; bronchodilator; preferred in shock/asthma; causes psychomimetic effects (prevented by benzodiazepine pre-treatment)
- Etomidate = most haemodynamically stable; inhibits adrenal 11β-hydroxylase → adrenocortical suppression
- Barbiturates vs. Benzodiazepines on GABA-A: Barbiturates ↑ duration of Cl⁻ channel opening; Benzodiazepines ↑ frequency of Cl⁻ channel opening
- Dexmedetomidine = only sedative with no significant respiratory depression; antagonist: none (atipamezole is experimental)
- Flumazenil = specific benzodiazepine antagonist; shorter duration than benzodiazepines — resedation possible
Sources: Katzung's Basic and Clinical Pharmacology 16e, Ch. 25; Lippincott Illustrated Reviews: Pharmacology, Ch. 20; Barash's Clinical Anesthesia 9e, Ch. 19; Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.