Classify General Anesthetics. Discuss the advantages and disadvantages of Halothane as a general anesthetic
Reading File
Finding Sources
Finding Sources
Searching the Web
halothane general anesthetic advantages disadvantages pharmacology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full response:
Classification of General Anesthetics
General anesthetics are broadly divided based on the route of administration:
I. Inhalational (Inhaled) Anesthetics
These are further subdivided into gaseous and volatile agents:
A. Gaseous Anesthetics
Drugs that exist as a gas at room temperature (high vapor pressure, low boiling point):
- Nitrous oxide (N₂O) — the most widely used; incomplete anesthetic alone (MAC >100%)
- Xenon — rarely used clinically due to cost
B. Volatile Anesthetics
Drugs that are liquids at room temperature but vaporize for delivery via precision vaporizers:
| Agent | Chemical Class | MAC (%) | Key Feature |
|---|---|---|---|
| Halothane | Halogenated alkane | 0.75 | Bronchodilator; hepatotoxic; historical |
| Isoflurane | Halogenated ether | 1.15 | Coronary vasodilator; widely used |
| Desflurane | Halogenated ether | 6.0 | Fastest emergence; airway irritant |
| Sevoflurane | Halogenated ether | 2.0 | Smooth induction; preferred in pediatrics |
| Enflurane | Halogenated ether | 1.68 | Rarely used; seizurogenic at high doses |
| Methoxyflurane | Halogenated ether | 0.16 | Analgesic use; nephrotoxic at anesthetic doses |
The rank order for hepatic metabolism is: halothane > enflurane > sevoflurane > isoflurane > desflurane > nitrous oxide. — Katzung's Basic and Clinical Pharmacology, 16th Ed.
II. Intravenous (IV) Anesthetics
A. Barbiturates
- Thiopental sodium (ultra-short acting)
- Methohexital
B. Non-Barbiturate Sedative-Hypnotics
- Propofol — most widely used IV induction agent; antiemetic properties
- Etomidate — hemodynamically stable; adrenal suppression risk
C. Dissociative Anesthetics
- Ketamine — produces "dissociative anesthesia"; bronchodilator; raises BP and ICP; analgesia maintained
D. Benzodiazepines
- Midazolam, diazepam — sedation, amnesia, anxiolysis; used as adjuncts
E. Alpha-2 Agonists
- Dexmedetomidine — sedation without respiratory depression
F. Opioids (as adjuncts)
- Fentanyl, remifentanil, morphine — component of balanced anesthesia
III. Classification by Stage of Anesthesia (Guedel's Stages)
| Stage | Description |
|---|---|
| I | Analgesia — conscious, reduced pain perception |
| II | Excitement/delirium — loss of consciousness; risk of vomiting/laryngospasm |
| III | Surgical anesthesia — planes 1–4; loss of reflexes; suitable for surgery |
| IV | Medullary depression — circulatory/respiratory failure; fatal if untreated |
Halothane as a General Anesthetic
Chemical structure: Halothane (2-bromo-2-chloro-1,1,1-trifluoroethane) is a halogenated alkane.
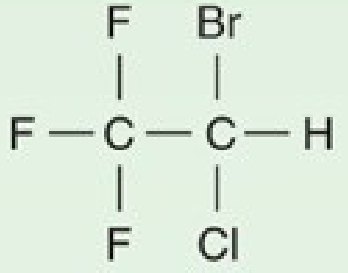
MAC: 0.75% | Blood:gas partition coefficient: 2.4 (relatively soluble → slower induction/recovery)
Halothane is stored in amber bottles with thymol as a preservative because it is light-sensitive. It is non-flammable and non-explosive in oxygen or air mixtures.
Advantages of Halothane
1. Potent Bronchodilator
Halothane is one of the most effective bronchodilators among anesthetic agents. It relaxes bronchial smooth muscle by inhibiting intracellular calcium mobilization and is not inhibited by β-adrenergic blockers. This makes it historically valuable in patients with asthma or bronchospasm. It is non-pungent (does not irritate airways), unlike isoflurane and desflurane, making it suitable for smooth mask induction. — Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
2. Smooth, Non-Pungent Induction
Halothane's lack of airway irritancy allows inhalational induction without coughing, breath-holding, or laryngospasm — a major advantage for pediatric patients or patients who refuse IV access.
3. Potent Anesthetic
With a low MAC of 0.75%, halothane achieves surgical anesthesia at relatively low inhaled concentrations. It produces good CNS depression, reducing cerebral metabolic oxygen requirements.
4. Muscle Relaxation
Halothane produces direct skeletal muscle relaxation and potentiates nondepolarizing neuromuscular blocking agents, reducing the dose requirements of NMBAs. — Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
5. Low Cost and Wide Availability
Halothane has low manufacturing cost and remains widely used in developing countries where newer agents (sevoflurane, desflurane) are unaffordable or unavailable. — Goodman & Gilman's Pharmacological Basis of Therapeutics
6. Uterine Relaxation
Like other halogenated anesthetics, it causes potent uterine muscle relaxation in a concentration-dependent manner — useful for intrauterine fetal manipulation or retained placenta extraction.
7. Cardiac Benefits (Limited)
Adequate myocardial perfusion is usually maintained as both oxygen demand and coronary flow decrease proportionally. Halothane is a coronary vasodilator, and it does not typically cause "coronary steal" as has been debated with isoflurane.
Disadvantages of Halothane
1. Halothane Hepatitis (Most Serious)
Halothane undergoes extensive hepatic metabolism (~20–40% of inhaled dose) via CYP2E1, producing trifluoroacetic acid. Under hypoxic conditions, reductive metabolism yields hepatotoxic intermediates that covalently bind to liver macromolecules.
- Mild form: Transient elevation of liver transaminases — occurs in up to 20% of patients
- Fulminant halothane hepatitis: Occurs in approximately 1 in 10,000 patients; carries a 50% fatality rate
- Characterized by: fever, anorexia, nausea, vomiting, jaundice, eosinophilia, rash — appearing several days post-exposure
- The immune mechanism involves trifluoroacetylated liver proteins acting as neoantigens, triggering an antibody response
- Risk factors: multiple halothane exposures at short intervals, middle-aged obese women, familial predisposition
- Contraindicated in patients with unexplained liver dysfunction after previous halothane exposure
— Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.; Katzung, 16th Ed.
2. Cardiovascular Depression
- Causes a dose-dependent decrease in arterial BP primarily through direct myocardial depression (reduced cardiac output), unlike isoflurane/desflurane which cause vasodilation
- 2.0 MAC → ~50% decrease in blood pressure and cardiac output
- Increases right atrial pressure (reflecting reduced contractility)
- Blunts baroreceptor reflexes → no compensatory tachycardia
- Can cause sinoatrial node slowing → junctional rhythm or bradycardia
- In infants: decreases cardiac output by both reduced heart rate and depressed contractility
3. Sensitization of the Heart to Catecholamines
Halothane sensitizes the myocardium to arrhythmogenic effects of epinephrine. Doses of epinephrine above 1.5 mcg/kg should be avoided. This limits its use when:
- Exogenous epinephrine is injected (e.g., in local anesthetic solutions)
- The patient has a pheochromocytoma
4. Raised Intracranial Pressure
By dilating cerebral vessels, halothane lowers cerebrovascular resistance and increases cerebral blood volume and CBF. This raises ICP. Crucially, hyperventilation must be established before halothane administration (unlike isoflurane, which can be started first). Contraindicated in patients with intracranial mass lesions unless combined with hyperventilation.
5. Respiratory Depression
- Causes rapid, shallow breathing; increased rate does not compensate for decreased tidal volume → elevated PaCO₂
- Severely depresses hypoxic drive even at sub-anesthetic concentrations (0.1 MAC)
- Depresses mucociliary clearance → promotes postoperative atelectasis and pneumonia
6. Malignant Hyperthermia (MH)
Halothane is a triggering agent for malignant hyperthermia in susceptible individuals. Absolutely contraindicated in patients with known or suspected MH susceptibility.
7. Slower Induction and Recovery
Blood:gas partition coefficient of 2.4 (vs. 0.42 for desflurane, 0.65 for sevoflurane) means slower equilibration → longer induction and recovery times.
8. Renal Effects
Reduces renal blood flow, GFR, and urinary output — partly due to reduced cardiac output. The filtration fraction is increased (efferent arteriolar tone preserved).
9. Obsolescence in Developed Countries
Due to its hepatotoxicity profile and the availability of safer agents with more favorable pharmacokinetics (sevoflurane, desflurane), halothane is no longer marketed in the United States and most developed nations. — Goodman & Gilman's
Summary Table: Halothane Advantages vs. Disadvantages
| Advantages | Disadvantages |
|---|---|
| Potent bronchodilator | Halothane hepatitis (1:10,000; 50% mortality) |
| Non-pungent → smooth inhalational induction | Profound myocardial depression |
| Low MAC (0.75%) — potent | Sensitizes heart to epinephrine → arrhythmias |
| Skeletal muscle relaxation | Increases ICP (must pre-hyperventilate) |
| Low cost; available in developing countries | Triggers malignant hyperthermia |
| Uterine relaxation | Severe respiratory depression; ↓ hypoxic drive |
| — | Slow induction/recovery (high blood solubility) |
| — | Depresses mucociliary clearance |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition (Morgan & Mikhail)
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Miller's Anesthesia, 10th Edition
This is a shared conversation. Sign in to Orris to start your own chat.