CA cervix
Reading File
Finding Sources
Searching PubMed
"cervical cancer"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"uterine cervical neoplasms"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive information to compile a thorough answer. Let me deliver the full structured response.
Carcinoma of the Cervix (CA Cervix)
1. Anatomy & the Transformation Zone
The cervix is the narrow, distal portion of the uterus (~3 cm long) projecting into the vaginal vault. It has:
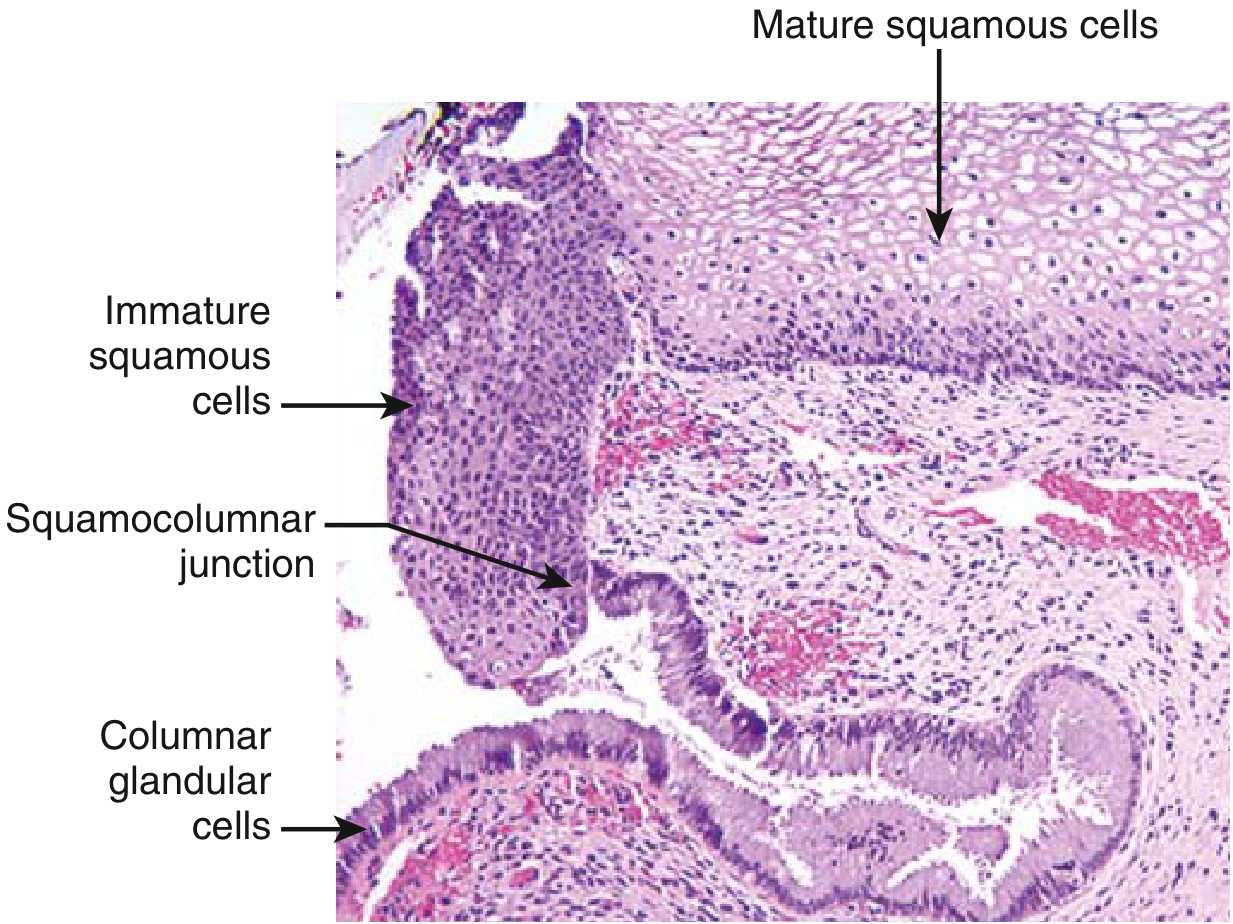
- Ectocervix - covered by stratified squamous epithelium
- Endocervix - lined by mucus-secreting columnar epithelium
- Squamocolumnar junction (SCJ) - where the two epithelia meet; its position shifts with age and hormonal status
At puberty, columnar epithelium everts onto the ectocervix. This undergoes squamous metaplasia, creating the transformation zone - the site where immature metaplastic cells are most vulnerable to HPV infection, and where virtually all cervical cancers arise.
2. Etiology & Pathogenesis
HPV is the single most important causative factor - virtually all cervical cancers are HPV-driven.
HPV Biology
- HPVs are DNA viruses classified as high-risk (oncogenic) or low-risk based on genotype
- HPV 16 and 18 account for ~70% of all CIN and cervical carcinomas
- Low-risk HPV types 6 and 11 cause genital condylomas but rarely cancer
Mechanism of Oncogenesis
Two key viral early proteins drive malignant transformation:
| Viral Protein | Target | Effect |
|---|---|---|
| E6 | p53 (tumor suppressor) | Binds and destroys p53; upregulates telomerase |
| E7 | Rb (tumor suppressor) | Binds Rb, releases E2F transcription factors, drives cell cycle progression |
- High-risk HPV integrates into the host genome - disrupting the viral gene that negatively regulates E6/E7, causing their overexpression
- Integration also increases genomic instability, allowing accumulation of additional mutations
- Most HPV infections are transient and cleared by immune response; only persistent infection leads to cancer
Risk Factors for CIN/Cervical Cancer
- Early age at first intercourse
- Multiple sexual partners (or partner with multiple partners)
- Persistent high-risk HPV infection
- Cigarette smoking (co-carcinogen)
- Immunosuppression (HIV, transplant)
- Non-participation in cervical screening
3. Precursor Lesions: SIL / CIN
HPV-related carcinogenesis begins with Squamous Intraepithelial Lesion (SIL), also termed Cervical Intraepithelial Neoplasia (CIN).
| Old Term | Bethesda System | Features |
|---|---|---|
| CIN 1 | LSIL (Low-grade SIL) | Koilocytic atypia; changes confined to lower 1/3 of epithelium; associated with transient HPV |
| CIN 2 | HSIL (High-grade SIL) | Progressive atypia in lower 2/3 |
| CIN 3 / CIS | HSIL (High-grade SIL) | Full-thickness atypia and loss of maturation |
- SIL peaks at ~30 years; invasive carcinoma peaks at ~45 years (10-15 year lag)
- Koilocytes: HPV-infected squamous cells with perinuclear cytoplasmic clearing and nuclear enlargement - hallmark of LSIL
- Management: LSIL → conservative observation; HSIL/persistent LSIL → surgical excision (cone biopsy/LEEP)
4. Invasive Carcinoma
Histological Subtypes
| Type | Frequency | Notes |
|---|---|---|
| Squamous cell carcinoma | ~80% | Most common; peaks at age 45 |
| Adenocarcinoma / Adenosquamous | ~15% | Increasing proportion (harder to detect on Pap) |
| Small cell neuroendocrine | <5% | Very poor prognosis |
All are caused by high-risk HPV.
Gross & Microscopic Morphology
- Range from microscopic stromal invasion to large exophytic tumors
- Microscopically: tongues and nests of squamous cells with desmoplastic stromal response
- Grading by degree of squamous differentiation (keratin pearl formation = well-differentiated)
- Barrel cervix: tumor encircles and distends the cervix - palpable on exam
- Parametrial extension can fix the uterus to surrounding pelvic structures

Lymph Node Metastasis Risk by Depth
| Invasion Depth | Risk of LN Metastasis |
|---|---|
| < 3 mm | < 1% |
| > 3 mm | > 10% |
5. FIGO Staging (2018)
Staging is clinical (complemented by MRI, CT, PET-CT) and uses the FIGO system:
| Stage | Description |
|---|---|
| I | Confined to the cervix |
| IA | Microscopic invasion; IA1 ≤3 mm depth, IA2 3-5 mm depth |
| IB | Clinically visible / >5 mm; IB1 (<2 cm), IB2 (2-4 cm), IB3 (≥4 cm) |
| II | Beyond cervix but not to pelvic wall or lower 1/3 vagina |
| IIA | No parametrial involvement; IIA1 (<4 cm), IIA2 (≥4 cm) |
| IIB | Parametrial involvement |
| III | Pelvic wall / lower 1/3 vagina / hydronephrosis / pelvic or para-aortic lymph nodes |
| IIIA | Lower 1/3 vagina |
| IIIB | Pelvic wall or hydronephrosis |
| IIIC | LN involvement (IIIC1 = pelvic, IIIC2 = para-aortic) |
| IV | Invades bladder/rectum mucosa (IVA) or distant metastases (IVB) |
MRI is the modality of choice for staging - it accurately delineates tumor size, parametrial invasion, and vaginal involvement.
6. Clinical Features
Invasive cervical cancer is most often diagnosed in unscreened or under-screened women.
Symptoms:
- Unexpected/postcoital vaginal bleeding (most common presenting symptom)
- Foul-smelling leukorrhea
- Dyspareunia (painful intercourse)
- Dysuria / urinary symptoms
- Pelvic or back pain (advanced disease)
- Hydronephrosis (Stage IIIB - ureter compression by pelvic mass)
Early disease may be entirely asymptomatic, detected only on Pap smear.
7. Screening & Diagnosis
| Investigation | Purpose |
|---|---|
| Pap smear (cytology) | Primary screening; detects SIL/CIN |
| HPV co-testing | Adds sensitivity; preferred in women ≥30 |
| Colposcopy | Follows abnormal Pap; acetic acid whitening identifies lesions |
| Cervical biopsy | Confirms diagnosis |
| Cone biopsy/LEEP | Definitive tissue diagnosis + treatment for HSIL |
| MRI pelvis | Local staging, parametrial invasion |
| CT chest/abdomen/pelvis | LN and distant metastases |
| PET-CT | Most sensitive for nodal/distant disease |
| Cystoscopy / sigmoidoscopy | Rule out bladder/rectal mucosal invasion (Stage IVA) |
8. Management
Early Stage (IA1 - IB1, IIA1)
- Surgery is preferred (fertility-preserving or radical)
- Stage IA1: Cone biopsy (if fertility desired) or simple hysterectomy
- Stage IA2-IB1: Radical hysterectomy (Wertheim's) + pelvic lymph node dissection
- Radical trachelectomy (cervix only) may preserve fertility in selected IA2-IB1 cases
Locally Advanced (IB2 - IVA)
- Concurrent chemoradiotherapy (CCRT) is the standard of care
- External beam radiation to pelvis + brachytherapy boost to cervix
- Cisplatin-based chemotherapy as radiosensitizer
- INTERLACE trial (Lancet 2024, PMID 39419054): Induction chemotherapy (carboplatin + paclitaxel) followed by standard CCRT showed improved outcomes in locally advanced disease
Advanced/Metastatic (IVB / Recurrent)
- Chemotherapy: Cisplatin + paclitaxel ± bevacizumab (VEGF inhibitor)
- Immunotherapy: Pembrolizumab (anti-PD-1) - approved for PD-L1+ recurrent/metastatic disease
- Palliative radiation for symptom control
Surgery - Key Points
- Blood supply: descending branch of uterine artery at 3 and 9 o'clock positions laterally
- Ureters run ~2 cm lateral to the cervix in the cardinal ligament - risk of injury in radical hysterectomy
- Innervation: parasympathetic from lumbosacral plexus (S2-S4), concentrated in the endocervical region
9. Prognosis
- Stage at diagnosis is the most important prognostic factor
- Stage I: 5-year survival ~90-95%
- Stage II: ~75%
- Stage III: ~50%
- Stage IV: ~15-20%
- Small cell neuroendocrine carcinoma has the worst prognosis regardless of stage
- Pelvic lymph node involvement significantly worsens prognosis
10. Prevention
| Measure | Details |
|---|---|
| HPV vaccination | Gardasil 9 covers HPV 16, 18 (+ 6, 11, 31, 33, 45, 52, 58); most effective when given before first sexual exposure; recommended ages 9-26 years (up to 45 in some guidelines) |
| Cervical screening | Pap smear ± HPV co-testing every 3-5 years from age 21-25 |
| Safe sex practices | Reduce HPV exposure |
Recent Evidence Update
A key 2024 RCT (INTERLACE, McCormack et al., Lancet 2024, PMID 39419054) showed that induction chemotherapy (carboplatin + paclitaxel × 6 weeks) prior to standard chemoradiotherapy improved progression-free and overall survival in locally advanced cervical cancer - a potential practice-changing addition to the standard of care. A 2025 review in Nature Reviews Clinical Oncology (Francoeur et al., PMID 39753753) further summarizes advances including immunotherapy integration and targeted agents across the cervical cancer spectrum.
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Berek & Novak's Gynecology; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.