IgE
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a comprehensive overview of Immunoglobulin E (IgE) drawn from multiple authoritative textbooks:
IgE (Immunoglobulin E)
Structure
IgE is the least abundant immunoglobulin in serum, comprising only ~0.0005% of total serum immunoglobulin. Its unique structural features set it apart from other isotypes:
- Heavy chain: epsilon (ε) chain - structurally distinct from other Ig isotypes
- Molecular formula: ε₂L₂ (two epsilon heavy chains + two light chains)
- Molecular weight: ~190,000 Da (ε chain alone: ~70,000 Da)
- Extra domain: Has an additional Cε4 domain, giving it higher molecular weight than IgG
- Carbohydrate content: ~18% (more heavily glycosylated than IgG)
- Valency: Functional valency of 2 (bivalent)
- No complement fixation (classic pathway)
- No placental transfer
Table 56.2, Henry's Clinical Diagnosis and Management by Laboratory Methods
Serum Half-Life and Distribution
| Property | Value |
|---|---|
| Serum half-life | 1-5 days |
| IgG serum half-life (comparison) | ~20 days |
| Catabolic rate | >70% per day |
| Tissue-bound (mast cell) half-life | Up to several months |
The very low serum concentration reflects both avid binding to effector cells and a high catabolic rate. Once bound to mast cells, IgE persists for months.
IgE Class Switching and Production
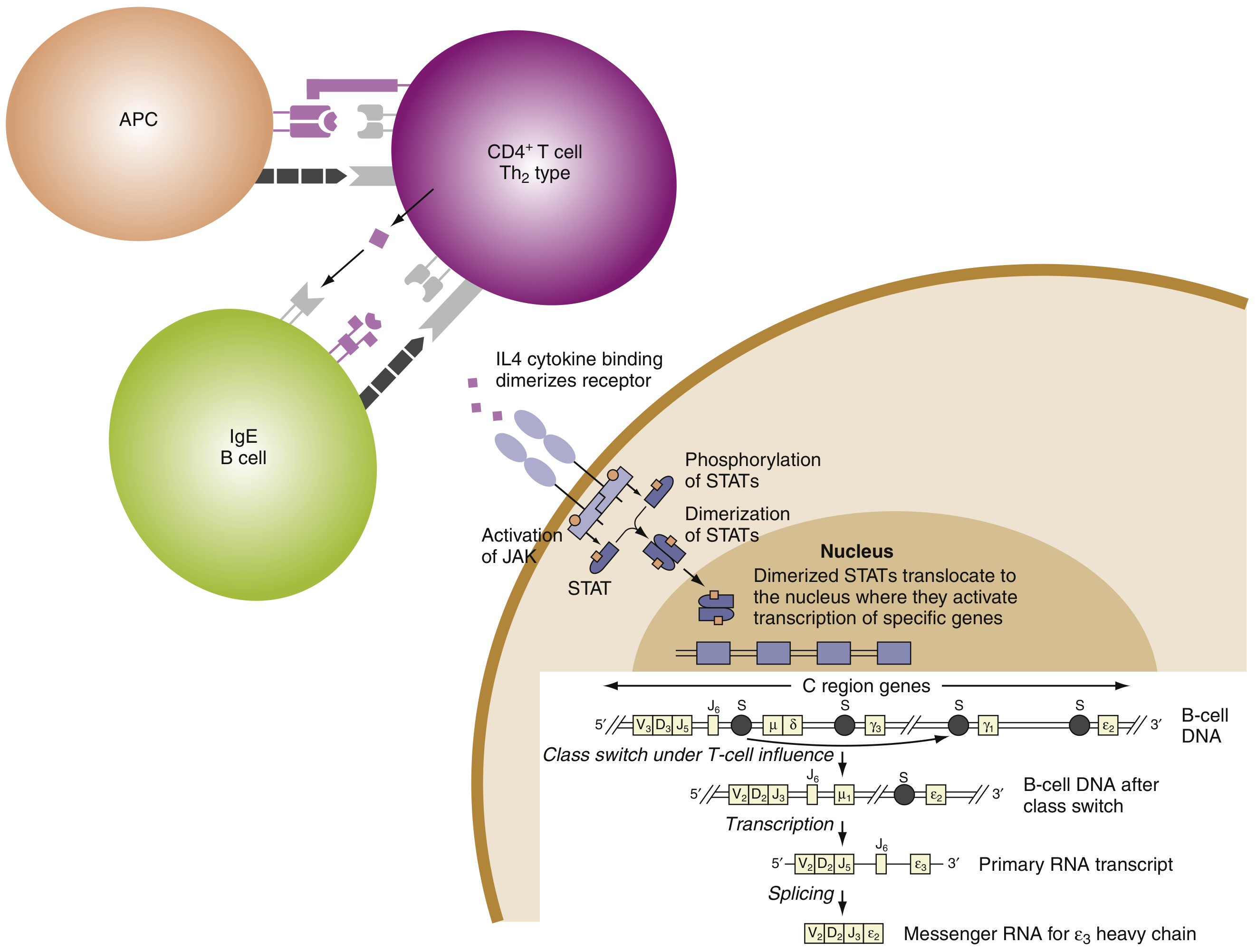
IgE production requires a two-signal B cell activation:
- IL-4 and IL-13 (from Th2/TFH cells) drive class switch recombination to the ε heavy chain via JAK-STAT6 signaling
- CD40L-CD40 interaction (T cell contact signal) provides a costimulatory signal
Key transcription factors and genes involved:
- IL-4, IL-13, IL-4Rα, STAT6 - the core molecular determinants of atopy
- GATA-3 - Th2 differentiation
- Class II HLA loci on chromosome 6p - influence sensitization to specific allergens
FcεRI - The High-Affinity IgE Receptor
IgE exerts its biological effects primarily via FcεRI (high-affinity Fc epsilon receptor I):
- Expressed on mast cells and basophils
- IgE binds to FcεRI via its Fc region (the Cε3 and Cε4 domains)
- Binding is extremely avid - this "loads" mast cells with antigen-specific IgE
- When antigen cross-links two or more FcεRI-bound IgE molecules, degranulation is triggered
There is also a low-affinity receptor FcεRII (CD23) expressed on B cells, monocytes, and eosinophils, which regulates IgE synthesis.
Mechanism of Immediate Hypersensitivity (Type I)
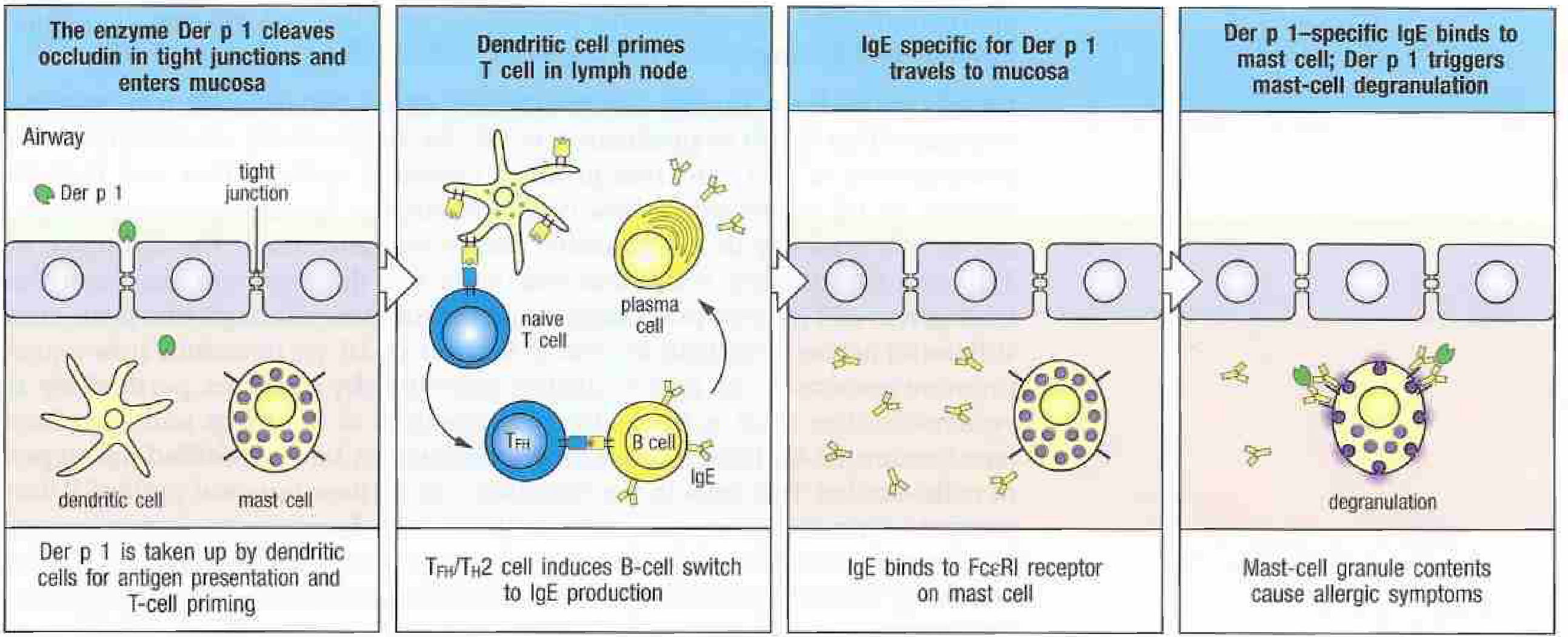
Phase 1: Sensitization
- Allergen penetrates epithelial barrier
- Dendritic cells capture allergen and traffic to lymph node
- TFH/Th2 cells are primed; IL-4 and IL-13 are produced
- B cells undergo class switch to produce allergen-specific IgE
- IgE travels to tissues and binds FcεRI on mast cells
Phase 2: Elicitation (re-exposure)
- Allergen re-enters the tissue
- Allergen cross-links mast cell-surface IgE
- Mast cell degranulation occurs within minutes
- Pre-formed mediators released: histamine, tryptase, chondroitin sulfates, TNF-α
- Newly synthesized mediators: leukotrienes (LTC4), prostaglandins (PGD2)
Janeway's Immunobiology 10e; Cellular and Molecular Immunology
Atopy and Genetic Determinants
"Atopic" individuals are genetically predisposed to produce specific IgE following allergen exposure. Key features:
- Production of high IgE depends on a propensity to generate allergen-specific TFH cells secreting IL-4 and IL-13
- Candidate genes: IL4, IL13, IL4R, STAT6 (chromosome 5q), HLA class II loci (chromosome 6p), FcεRI α chain locus (chromosome 1q23)
- Allergen characteristics that favor IgE responses: MW 5-70 kDa, stable, glycosylated, soluble, often enzymatic activity (e.g., house dust mite cysteine protease, bee venom phospholipase A2)
- Repeat exposure is required - first exposure sensitizes (IgE produced), second exposure triggers reaction
- Non-protein antigens (e.g., penicillin) can cause IgE responses by acting as haptens bound to self proteins
Mast Cell Subtypes Relevant to IgE
| Feature | MCT (mucosal) | MCTC (connective tissue) |
|---|---|---|
| Contains | Tryptase only | Tryptase + chymase |
| Location | Mucosal surfaces, near T cells | Submucosa, connective tissue |
| Allergic role | Yes - at sites of allergic inflammation | Less associated |
| Mediators | High LTC4, PGD2 | Less LTC4 |
| IL-4 content | Low | Higher |
Clinical Diseases Associated with IgE
IgE-mediated (Type I Hypersensitivity)
- Allergic rhinitis (hayfever)
- Allergic asthma
- Atopic dermatitis (eczema)
- Urticaria (hives)
- Food allergy
- Anaphylaxis - systemic, life-threatening; IgE cross-linking in vascular system
Hyper-IgE Syndrome (Job Syndrome)
Characterized by markedly elevated IgE + eczema + eosinophilia + recurrent pulmonary infections + "cold" staphylococcal skin abscesses:
- Autosomal dominant form: Heterozygous dominant-negative STAT3 mutations - impairs IL-6, IL-10, IL-17, IL-21, IL-22 signaling; reduces Th17 responses; increases IL-4/IL-13/Th9 driving IgE overproduction
- Autosomal recessive form: DOCK8 mutations - reduced T, B, NK cells; defective lymphocyte signaling similar to Wiskott-Aldrich syndrome
Cellular and Molecular Immunology
Anti-IgE Therapy
Omalizumab (anti-IgE monoclonal antibody) targets free IgE and is used in:
- Severe allergic asthma
- Chronic urticaria
- Other IgE-driven conditions
By binding free IgE, it reduces loading of mast cells and basophils, thereby blunting allergic responses.
Goodman & Gilman's Pharmacological Basis of Therapeutics
Laboratory Measurement
- Total serum IgE: Normal reference range is low (typically < 100 IU/mL in adults); elevated in atopic disease, parasitic infections, Hyper-IgE syndrome
- Specific IgE (sIgE): ImmunoCAP assay measures IgE directed against individual allergens; used in allergy diagnosis
- Nasal specific IgE: Can be detected locally even when serum IgE is normal (entopy)
Henry's Clinical Diagnosis & Management by Laboratory Methods; Cummings Otolaryngology
Sources: Janeway's Immunobiology 10e | Cellular and Molecular Immunology | Henry's Clinical Diagnosis and Management by Laboratory Methods | Goodman & Gilman's Pharmacological Basis of Therapeutics | Cummings Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.