Internal medicine: hypertension detailed exam oriented what to understand and apply in practice
Reading File
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "guideline"[pt]
Reading File
Finding Sources
Reading Article
PMID: 40811516
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive, exam-oriented response. Let me compile it.
Hypertension - Internal Medicine: Exam-Oriented Master Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Lippincott Illustrated Reviews Pharmacology, Frameworks for Internal Medicine, Brenner & Rector's The Kidney, 2025 AHA/ACC Guideline (PMID: 40811516), 2024 ESC Guidelines (PMID: 39210715)
1. PATHOPHYSIOLOGY - The Core Equation
BP = Cardiac Output × Peripheral Vascular Resistance
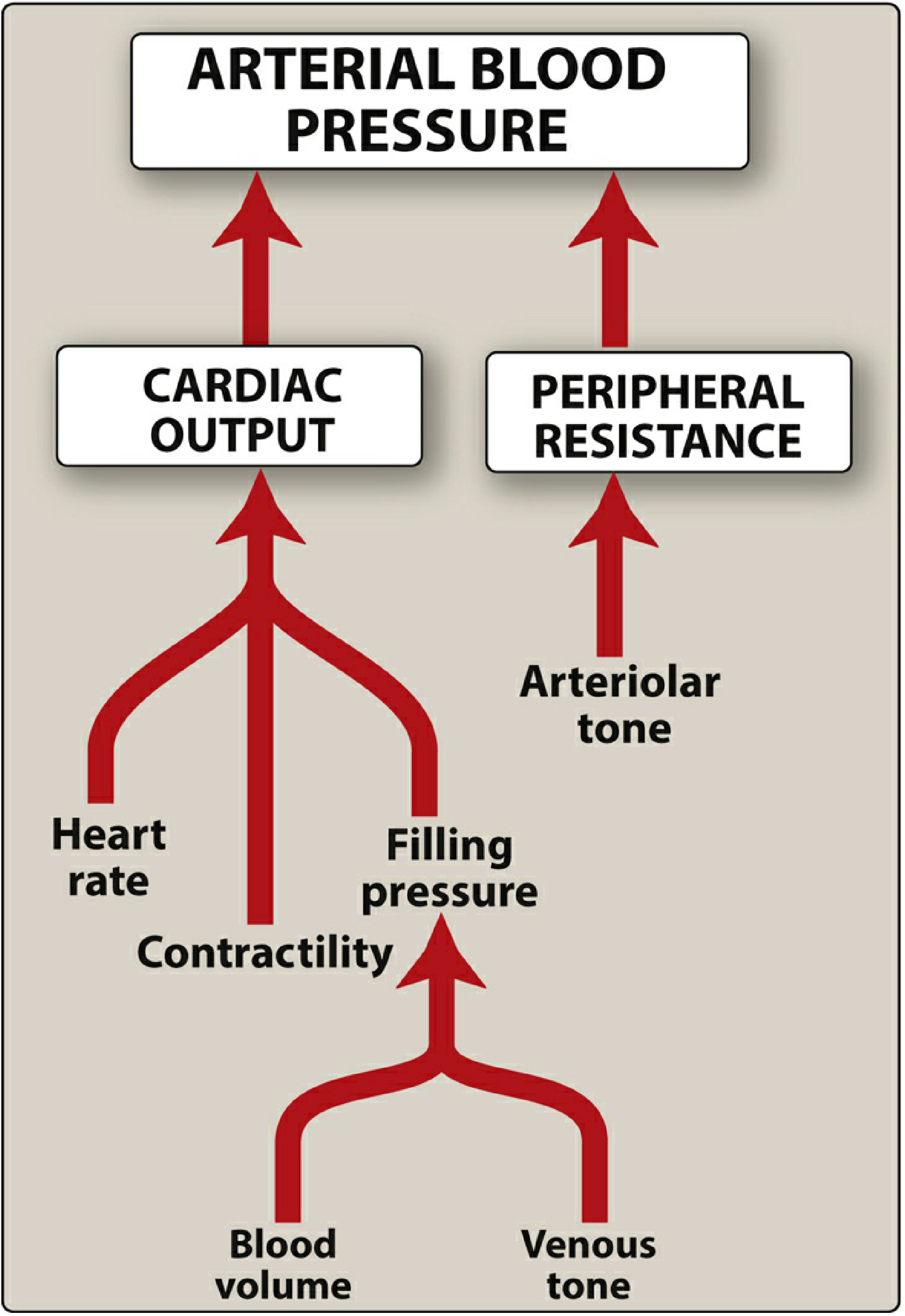
Two overlapping regulatory systems control CO and PVR:
- Sympathetic nervous system - baroreflexes, catecholamines
- Renin-Angiotensin-Aldosterone System (RAAS) - long-term sodium/volume control
The kidney plays a dominant role in long-term BP regulation via the pressure-natriuresis mechanism. When renal perfusion is impaired (renal artery stenosis, nephron loss), BP rises to maintain GFR - this is the core concept behind renovascular hypertension.
Key downstream mechanisms:
- Salt sensitivity: patchy increases in preglomerular resistance impair natriuresis → salt-sensitive HTN
- Endothelin-1 (ET-1): potent vasoconstrictor, mediates salt-sensitive HTN
- Nitric oxide (NO) deficiency: impairs renal pressure natriuresis, promotes oxidative stress
- Atrial natriuretic peptide (ANP): released by atrial stretch, promotes natriuresis - a counter-regulatory hormone
2. CLASSIFICATION (ACC/AHA - Applied in the US, 2025)
| BP Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Elevated | 120-129 | and | < 80 |
| Stage 1 HTN | 130-139 | or | 80-89 |
| Stage 2 HTN | ≥ 140 | or | ≥ 90 |
- Harrison's 22E (2025), Table 288-1; Lippincott Pharmacology, Fig 8.2
Exam pearls on classification:
- When SBP and DBP fall in different categories, use the higher one
- Always average ≥2 readings at ≥2 separate visits before diagnosing
- The 2024 ESC uses slightly different thresholds (Grade 1: 140-159/90-99; Grade 2: ≥160/≥100) - know which system your exam uses
3. BP MEASUREMENT - Accuracy is Testable
- Clinically validated oscillometric device preferred (eliminates observer bias)
- SBP is overestimated by ~7 mmHg on average in routine clinical practice, leading to 15-20% overestimation of HTN prevalence
- Patient must be seated, arm at heart level, 5 min of rest, bladder emptied, no caffeine/tobacco 30 min before
- Two readings per visit, averaged
White-Coat HTN vs Masked HTN
- White-coat HTN: elevated in office, normal out of office - use ambulatory BP monitoring (ABPM) to confirm
- Masked HTN: normal in office, elevated outside - also confirmed by ABPM; associated with cardiovascular risk similar to true HTN
- 24-hour ABPM is the gold standard for both
Nondipping BP
- Normally BP dips 10-20% during sleep
- Non-dippers (< 10% nocturnal fall) have higher cardiovascular risk - important clinical concept
4. ETIOLOGY
Primary (Essential) HTN - > 90% of cases
- No single identifiable cause; polygenic, environmental
- Risk factors: family history, age, Black race (higher incidence and severity), obesity, high sodium intake, physical inactivity, alcohol, diabetes, stressful lifestyle, low education/income
Secondary HTN - when to suspect it
Suspect secondary HTN in ANY of these scenarios:
- Treatment-resistant HTN (uncontrolled on ≥3 drugs including a diuretic at max doses)
- Abrupt worsening of previously controlled HTN
- Disproportionate target organ damage for the BP level
- Unprovoked hypokalemia, proteinuria, or LVH on ECG/echo
5. SECONDARY HYPERTENSION - Causes, Clues, Tests
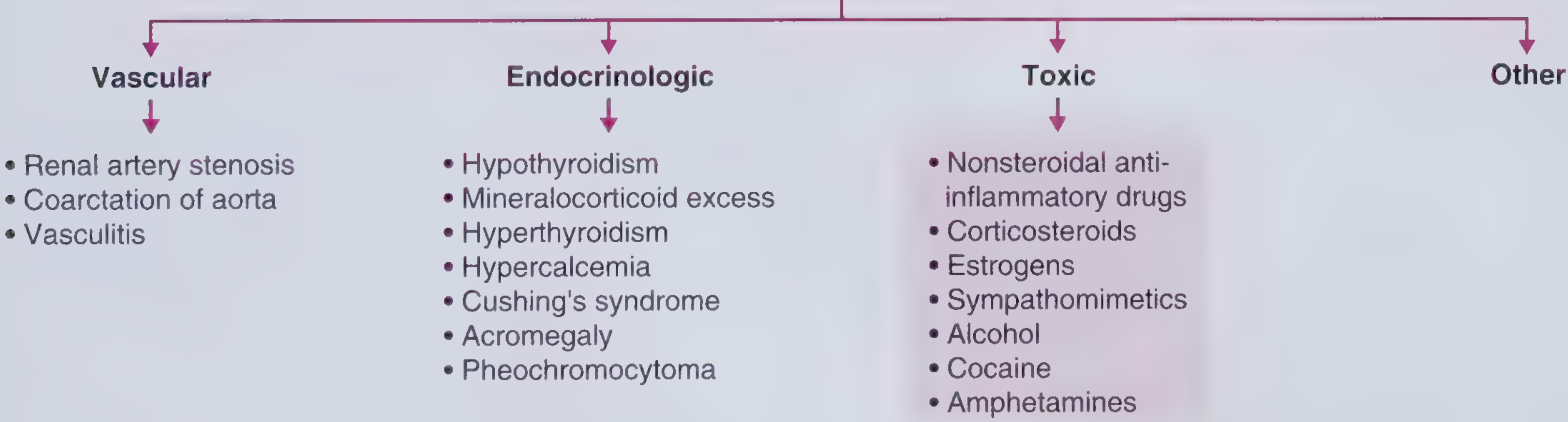
Vascular
| Cause | Clinical Clue | Test | Treatment |
|---|---|---|---|
| Renal artery stenosis | Abdominal bruit (especially diastolic); acute ↑ Cr after ACE-I/ARB; young woman (FMD) vs. older man (atherosclerosis) | Duplex US (initial); renal angiography (gold standard) | Revascularization (stent/surgery); ACE-I/ARB cautiously if bilateral |
| Coarctation of aorta | BP discordance upper vs. lower extremities; bounding carotid pulses; S4; rib notching on CXR; young person | Echocardiogram, CT/MRI aorta | Surgery or catheter-based repair |
| Vasculitis (PAN, Takayasu, GCA) | Multi-system features; elevated ESR/CRP | Angiography, biopsy | Immunosuppression |
FMD vs atherosclerosis in renal artery stenosis: FMD = most common in children/young adults (especially women), "string of beads" on angiography. Atherosclerosis = older adults, proximal renal artery lesion.
Endocrinologic
| Cause | Key Feature | Screening Test | Confirmatory Test |
|---|---|---|---|
| Primary aldosteronism (most common endocrine cause) | Hypokalemia (50% normokalemic!), resistant HTN, adrenal incidentaloma | Plasma aldosterone-to-renin ratio (ARR) | Adrenal vein sampling; CT adrenal |
| Pheochromocytoma | Episodic HTN, headache, diaphoresis, palpitations ("5 Hs": HTN, headache, hyperhidrosis, hyperglycemia, hypermetabolism); spells | Plasma free metanephrines (most sensitive) | 24-hr urine catecholamines; CT/MRI abdomen |
| Cushing's syndrome | Truncal obesity, striae, buffalo hump, moon facies, hyperglycemia | 24-hr urine cortisol; 1 mg overnight dexamethasone suppression test | Low-dose DST, CRH stimulation |
| Hypothyroidism | Bradycardia, weight gain, cold intolerance, dry skin | TSH | Free T4 |
| Hyperthyroidism | Primarily elevated pulse pressure/systolic HTN; tachycardia | TSH | Free T4/T3 |
| Acromegaly | Enlarged hands/feet, jaw, macroglossia | IGF-1 | Oral glucose tolerance test (GH) |
| Hyperparathyroidism/hypercalcemia | Nephrolithiasis, bone disease, fatigue | Serum calcium, PTH |
Renal Parenchymal
- Most common overall cause of secondary HTN
- CKD (HTN in majority of patients), acute glomerulonephritis, scleroderma renal crisis
- Mechanism: sodium and volume retention + RAAS activation
Obstructive Sleep Apnea (OSA)
- Probably the most common identifiable cause of secondary HTN per Harrison's
- Present in > 30% of US adults with HTN; hypertension present in most OSA patients
- Mechanism: intermittent hypoxia → sympathetic activation; severity of OSA correlates directly with BP and antihypertensive resistance
- Diagnosis: polysomnography; ABPM useful to assess for non-dipping pattern
- Treatment: CPAP - shown to improve associated HTN
Toxic/Drug-Induced
| Agent | Mechanism | Management |
|---|---|---|
| NSAIDs | Prostaglandin inhibition → sodium retention; +5 mmHg mean | Stop if possible; diuretics if not |
| Glucocorticoids | Mineralocorticoid receptor activation → Na/water retention | Salt restriction + diuretics |
| Oral contraceptives (estrogens) | 2-3x higher risk; especially with smoking, Black race, obesity | Stop or switch; low-dose diuretics |
| Sympathomimetics (methylphenidate, ephedrine, pseudoephedrine, oxymetazoline) | α-adrenergic vasoconstriction | Avoid beta-blockers alone (unopposed alpha) |
| Cocaine/amphetamines | Blocks NE reuptake → sympathetic surge | Avoid beta-blockers (unopposed alpha → crisis); use phentolamine or benzodiazepines |
| Chronic alcohol (> 2 drinks/day) | Dose-dependent; HTN also occurs in withdrawal 2-3 days after last drink | Reduce/abstain |
Critical exam point: Avoid beta-blockers in cocaine/sympathomimetic-induced HTN - unopposed alpha-adrenergic vasoconstriction worsens hypertensive crisis.
Neurologic
- Increased ICP (Cushing's response: HTN + bradycardia + irregular respirations)
- Quadriplegia, dysautonomia, Guillain-Barré syndrome
6. EVALUATION - Initial Workup
History
- Duration, severity, prior readings
- Symptoms of end-organ damage: headache, chest pain, dyspnea, vision changes, neurologic symptoms
- Medications (OCP, NSAIDs, decongestants, stimulants, steroids)
- Family history of HTN, cardiovascular disease, renal disease, pheochromocytoma (MEN2)
- Lifestyle: diet, sodium, alcohol, tobacco, physical activity
- Review for symptoms of secondary causes: spells (pheo), snoring/apnea (OSA), weight changes
Physical Exam - High-yield findings
- BP in both arms (> 10-15 mmHg difference → subclavian stenosis, coarctation)
- BP in legs (coarctation: lower extremity BP < upper extremity BP; normally lower limb > upper limb by ~10-20 mmHg)
- Fundoscopy: Keith-Wagener-Barker classification (arteriolar narrowing, AV nicking, cotton-wool spots, papilledema)
- Carotid bruits; abdominal bruits (renal artery stenosis)
- Thyroid enlargement
- Cushingoid features
- Signs of LVH: displaced PMI, S4
- Peripheral pulses: radio-femoral delay (coarctation)
Lab Testing - Routine Initial
- Basic metabolic panel (creatinine, BUN, electrolytes - K+)
- Urinalysis + urine albumin-to-creatinine ratio
- Fasting lipid panel, fasting glucose, HbA1c
- ECG (LVH, arrhythmia)
- CBC (polycythemia)
Add if secondary HTN suspected: thyroid function tests, aldosterone/renin ratio, plasma metanephrines, urine cortisol, renal Doppler US
7. TARGET ORGAN DAMAGE - What HTN Does to the Body
| Organ | Damage |
|---|---|
| Heart | LVH, diastolic dysfunction, HF with preserved EF (HFpEF), accelerated coronary artery disease, AF |
| Brain | Ischemic stroke, hemorrhagic stroke (especially hypertensive), lacunar infarcts, vascular dementia |
| Kidney | Hypertensive nephrosclerosis, proteinuria, CKD progression |
| Eyes | Hypertensive retinopathy (AV nicking, arteriovenous crossing changes, cotton-wool spots, flame hemorrhages, papilledema in emergency) |
| Peripheral arteries | PAD (HTN confers 2.5x risk in men, 3.9x in women) |
| Aorta | Dissection, aneurysm |
8. TREATMENT
A. Lifestyle Modifications (Non-pharmacologic) - Expected BP Reductions
| Intervention | Expected SBP Reduction |
|---|---|
| DASH diet | ~5 mmHg (with HTN); 2-3 mmHg (without HTN) |
| Sodium restriction (< 2300 mg/day) | ~5 mmHg (with HTN); 2-3 mmHg (without HTN) |
| Weight loss | ~1 mmHg per kg lost |
| Aerobic exercise (150 min/week) | ~5 mmHg; ~7 mmHg when combined with resistance training |
| Alcohol reduction | Dose-dependent benefit |
| Potassium supplementation | ~3 mmHg; greater effect in Black patients and high-sodium consumers |
Harrison's 22E (2025), derived from Table 288-2 / lifestyle intervention table
B. Pharmacologic Treatment
Drug Classes and Mechanisms
| Class | Mechanism | Key Agents | Compelling Indications |
|---|---|---|---|
| ACE inhibitors | Block conversion Ang I → Ang II; ↓ aldosterone | Lisinopril, ramipril, enalapril | CKD/proteinuria, HFrEF, post-MI, diabetes, high CVD risk |
| ARBs | Block AT1 receptor | Losartan, valsartan, olmesartan | Same as ACE-I; use if ACE-I cough intolerable |
| Thiazide/thiazide-like diuretics | Block NCC in DCT; ↓ sodium and volume | Hydrochlorothiazide, chlorthalidone (preferred), indapamide | First-line; especially Black patients; isolated systolic HTN elderly |
| Dihydropyridine CCBs | Block L-type calcium channels in vascular smooth muscle → vasodilation | Amlodipine, nifedipine | Elderly, isolated systolic HTN, Black patients, angina, Raynaud's |
| Non-dihydropyridine CCBs | Block cardiac and vascular calcium channels → rate + vasodilation | Diltiazem, verapamil | Atrial fibrillation rate control, angina; avoid in HFrEF |
| Beta-blockers | Block β1 (heart) → ↓ HR, CO; block β2 (kidney) → ↓ renin | Metoprolol succinate, carvedilol, bisoprolol | HFrEF, post-MI, angina, rate control; NOT first-line for uncomplicated HTN |
| Aldosterone antagonists | Block mineralocorticoid receptor | Spironolactone, eplerenone | Resistant HTN, HFrEF, primary aldosteronism |
| Alpha-1 blockers | Block peripheral α1 → vasodilation | Doxazosin, prazosin | BPH with HTN; NOT first-line |
| Central alpha-2 agonists | ↓ central sympathetic outflow | Clonidine, methyldopa | Methyldopa: first-line in pregnancy |
| Direct vasodilators | Relax arteriolar smooth muscle | Hydralazine, minoxidil | Reserved for resistant cases; hydralazine used in pregnancy |
Hydralazine adverse effects: Headache, tachycardia, palpitations, nausea, angina precipitation, drug-induced lupus (reversible on discontinuation)
Minoxidil adverse effect: Hypertrichosis (topically used for male-pattern baldness)
Compelling Indications Guide
| Comorbidity | Preferred Drug Class | Avoid |
|---|---|---|
| CKD with proteinuria | ACE-I or ARB | Dual ACE-I + ARB (hyperkalemia, AKI) |
| HFrEF | ACE-I/ARB (or ARNI), beta-blocker, aldosterone antagonist, SGLT2-i | Non-DHP CCBs (verapamil/diltiazem) |
| Post-MI | Beta-blocker, ACE-I, aldosterone antagonist | |
| Diabetes | ACE-I or ARB | |
| Black patients | Thiazide + CCB (RAAS less effective as monotherapy) | ACE-I/ARB monotherapy (less BP-lowering efficacy) |
| Atrial fibrillation (rate control) | Beta-blocker, non-DHP CCB | |
| Pregnancy | Methyldopa (first-line), hydralazine, labetalol | ACE-I, ARBs (teratogenic), spironolactone |
| Benign prostatic hyperplasia | Alpha-1 blocker (added benefit) | |
| Bilateral renal artery stenosis | Avoid ACE-I/ARB (↑ Cr, hyperkalemia) | ACE-I/ARB |
| Cocaine-induced HTN | Benzodiazepines, phentolamine | Beta-blockers (unopposed alpha → crisis) |
| Sympathomimetic-induced HTN | Alpha-blocker (phentolamine) | Beta-blockers alone |
BP Treatment Targets (2025 AHA/ACC)
- Most adults with confirmed HTN: < 130/80 mmHg
- High-risk patients (established CVD, CKD, DM): < 130/80 mmHg
- Note: 2025 AHA/ACC guideline reaffirms the 130/80 target introduced in 2017; the 2024 ESC uses < 130/80 in most, with < 140/90 acceptable in elderly frail patients
9. RESISTANT AND REFRACTORY HYPERTENSION
- Resistant HTN: BP uncontrolled despite ≥3 antihypertensive medications at optimal doses, including a diuretic - OR - requiring ≥4 medications to be controlled
- Pseudoresistance: Medication non-adherence (most common!), white-coat effect, improper BP measurement technique, suboptimal doses
- Refractory HTN: Uncontrolled on ≥5 agents including a mineralocorticoid antagonist
Workup for resistant HTN:
- Confirm adherence and proper BP measurement
- Eliminate offending substances (NSAIDs, OCP, decongestants, alcohol)
- Screen for secondary causes: primary aldosteronism (most common secondary cause in resistant HTN), OSA, renal artery stenosis, pheo
Fourth-line agent for resistant HTN: Spironolactone or eplerenone (mineralocorticoid antagonist) - most evidence for add-on benefit
10. HYPERTENSIVE CRISES
Hypertensive Emergency
- Definition: Severe BP elevation (usually SBP > 180 or DBP > 120 mmHg) WITH evidence of acute target organ damage
- Target organ damage: stroke/hemorrhage, aortic dissection, acute MI, acute decompensated HF (pulmonary edema), hypertensive encephalopathy, retinal hemorrhages/papilledema, acute kidney injury, eclampsia
Management principles:
- IV medications; ICU monitoring
- Goal: Reduce MAP by no more than 25% in the first hour, then toward 160/100 over 2-6 hours (exception: aortic dissection - must reduce rapidly to SBP < 120 in minutes)
- Avoid rapid BP drop - can precipitate ischemic stroke, MI, renal failure (autoregulation is set higher in chronic HTN)
IV agents for hypertensive emergency:
| Agent | Mechanism | Best For | Notes |
|---|---|---|---|
| Labetalol | Combined α + β blockade | Most emergencies, aortic dissection, pregnancy | Avoid in HF, bronchospasm |
| Nicardipine | Dihydropyridine CCB | Stroke, perioperative HTN, most emergencies | Titratable infusion |
| Clevidipine | Ultra-short-acting DHP CCB | Perioperative | Very rapid onset/offset |
| Nitroprusside | NO donor → venous + arterial dilation | Hypertensive encephalopathy, HF | Risk of cyanide toxicity (prolonged use); avoid in renal failure |
| Nitroglycerin | NO donor → predominantly venodilation | Acute coronary syndrome, HF with pulmonary edema | |
| Esmolol | Ultra-short-acting β1-blocker | Aortic dissection (combine with vasodilator), perioperative | |
| Phentolamine | Alpha-blocker | Pheochromocytoma, cocaine/MAOI/tyramine crisis | |
| Fenoldopam | Dopamine D1 agonist → renal vasodilation | Renal impairment (increases renal blood flow) | |
| Hydralazine | Direct vasodilator | Eclampsia/severe hypertension in pregnancy | Unpredictable; associated with reflex tachycardia |
Lippincott Illustrated Reviews Pharmacology, Section XV
Hypertensive Urgency
- Severe BP elevation WITHOUT acute target organ damage
- Oral medications; outpatient management acceptable; gradual reduction over 24-48 hours
11. SPECIAL POPULATIONS
Pregnancy
| Condition | Definition | Treatment |
|---|---|---|
| Gestational HTN | New BP ≥ 140/90 after 20 weeks; no proteinuria | Methyldopa, labetalol, nifedipine |
| Pre-eclampsia | HTN + proteinuria (or end-organ signs) after 20 weeks | MgSO4 (seizure prophylaxis); antihypertensives; delivery (definitive) |
| Eclampsia | Pre-eclampsia + seizures | MgSO4, delivery |
- Methyldopa = first-line in pregnancy
- ACE inhibitors and ARBs are absolutely contraindicated (fetotoxic)
- Hydralazine: IV use in acute severe HTN in pregnancy
Elderly
- Isolated systolic HTN (ISH) is dominant form (stiff arteries)
- Treatment reduces stroke and cardiovascular events even in very old patients (> 80 years)
- Preferred: thiazides, DHP-CCBs
- Start low, go slow; beware orthostatic hypotension and falls
Chronic Kidney Disease
- ACE-I or ARBs are preferred (reduce proteinuria, slow progression)
- Target BP < 130/80 mmHg
- Diuretic choice: thiazides lose efficacy when eGFR < 30; use loop diuretics (furosemide) at low eGFR
Black Patients
- Higher incidence, earlier onset, more severe, more end-organ damage
- Thiazides + DHP-CCBs work better as initial therapy
- RAAS monotherapy less effective than in White patients (lower renin states)
- Add ACE-I/ARB when diabetes or CKD is also present
12. KEY EXAM VIGNETTE PATTERNS
| Clinical Scenario | Diagnosis/Answer |
|---|---|
| Young woman, HTN, abdominal bruit | Renal artery stenosis (FMD) |
| HTN worsens after starting lisinopril, Cr rises | Bilateral renal artery stenosis - stop ACE-I |
| Upper > lower extremity BP, S4, rib notching on CXR | Coarctation of aorta |
| Hypokalemia + HTN + high aldosterone, low renin | Primary aldosteronism |
| Episodic HTN, headache, sweating, palpitations | Pheochromocytoma (check plasma metanephrines) |
| HTN + Cushingoid features | Cushing's syndrome |
| Resistant HTN + snoring, obesity | OSA (CPAP improves BP) |
| HTN + cocaine intoxication | NO beta-blockers; use benzos ± phentolamine |
| Pregnant patient, BP 160/105, seizures | Eclampsia - MgSO4 + labetalol/hydralazine + delivery |
| BP 200/120, papilledema, acute kidney injury | Hypertensive emergency - IV labetalol or nicardipine |
| BP 190/110 in ER, no end-organ damage | Hypertensive urgency - oral meds, discharge + follow-up |
| 4 meds + diuretic, still > 140/90 | Resistant HTN - add spironolactone |
| HTN patient taking NSAIDs for joint pain | NSAID-induced HTN (+5 mmHg) - substitute acetaminophen |
13. CURRENT GUIDELINES ALERT
2025 AHA/ACC Guideline (PMID: 40811516) - Published October 2025 in Hypertension and Circulation. This replaces the 2017 guideline and is described as a "living document." It reaffirms the Stage 1/2 classification with thresholds of 130/80 and 140/90 mmHg and the treatment target of < 130/80 for most adults with confirmed HTN.
2024 ESC Guidelines (PMID: 39210715) - Uses a different classification (Grade 1: 140-159/90-99; Grade 2: 160-179/100-109; Grade 3: ≥ 180/110). European guidelines distinguish "elevated BP" from "hypertension" at 140/90 rather than 130/80. Know which system your exam tests.
Summary Mental Model
HTN = ↑CO and/or ↑PVR
↓
90%+ Primary (Essential)
↓
Remaining ~10%: Secondary - always ask:
- Resistant? Abrupt onset? Young? Lab clues?
↓
Evaluate: Renal (most common overall), OSA (most common identifiable),
Primary aldosteronism (most common endocrine),
Pheochromocytoma (most dangerous), Renovascular
↓
Treat: Lifestyle first → Drug choice by comorbidity
ACE-I/ARB = CKD/DM/HF
Thiazide + CCB = Black patients, elderly
Emergency: IV meds, MAP -25% in 1h (except dissection)
Pregnancy: Methyldopa, labetalol, hydralazine; NEVER ACE-I/ARB
- Lippincott Illustrated Reviews Pharmacology, Sections II, III, XIV, XV
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 288 (Table 288-1, Table 288-3, lifestyle intervention table)
- Frameworks for Internal Medicine, Chapter 39 (Secondary Hypertension)
- Brenner & Rector's The Kidney (RAAS, renal mechanisms)
- 2025 AHA/ACC Guideline (PMID: 40811516) | 2024 ESC Guidelines (PMID: 39210715)
Mcqs
Here are 25 high-yield MCQs on hypertension, covering everything from the guide above. Each question is followed by the answer and a focused explanation.
Hypertension - 25 Exam MCQs
Q1. A 28-year-old woman presents with hypertension. On exam, her BP is 168/98 mmHg in both arms but 110/70 mmHg in both legs. She has bounding carotid pulses and an S4 gallop. Chest X-ray shows rib notching. What is the most likely diagnosis?
- A) Renal artery stenosis
- B) Primary aldosteronism
- C) Coarctation of the aorta
- D) Takayasu arteritis
- E) Pheochromocytoma
Answer
C - Coarctation of the aorta
The classic triad: upper extremity hypertension with lower extremity hypotension, rib notching (collateral intercostal vessels), and an S4 from LVH. The discordant BP between upper and lower extremities is pathognomonic. An S4 reflects impaired LV compliance from chronic pressure overload.
Q2. A 52-year-old man with hypertension on three medications (amlodipine 10 mg, lisinopril 40 mg, chlorthalidone 25 mg) has a BP of 152/94 mmHg. He snores heavily, his wife reports witnessed apneas, and his BMI is 37 kg/m². What is the single most likely cause of his resistant hypertension?
- A) Primary aldosteronism
- B) Renal artery stenosis
- C) Obstructive sleep apnea
- D) Pheochromocytoma
- E) Cushing's syndrome
Answer
C - Obstructive sleep apnea
OSA is probably the most common identifiable cause of resistant hypertension per Harrison's 22E. Over 30% of US adults with hypertension have OSA. The mechanism is intermittent hypoxia driving sympathetic activation. Severity of OSA directly correlates with BP level and resistance to antihypertensive therapy. CPAP is the most effective treatment and has been shown to improve associated hypertension.
Q3. A 45-year-old woman is found to have hypertension with a serum potassium of 2.9 mEq/L despite not taking diuretics. Her plasma aldosterone-to-renin ratio is markedly elevated. What is the next best step?
- A) Start spironolactone immediately
- B) 24-hour urine cortisol
- C) CT scan of the adrenal glands + adrenal vein sampling
- D) Renal artery Doppler ultrasound
- E) Plasma metanephrines
Answer
C - CT adrenal + adrenal vein sampling
This is primary aldosteronism. After a positive aldosterone-to-renin ratio (ARR) screen, the next steps are adrenal CT (to identify adenoma vs. bilateral hyperplasia) followed by adrenal vein sampling, which is the gold standard for lateralization. Spironolactone can be started empirically but you must lateralize first if surgery is being considered. Adrenal vein sampling differentiates unilateral adenoma (surgical cure with adrenalectomy) from bilateral adrenal hyperplasia (treated medically with aldosterone antagonists).
Q4. A 34-year-old man presents to the ED with BP 210/118 mmHg, severe headache, diaphoresis, and palpitations. He reports episodic "spells" of these symptoms over the past 3 months. Urine drug screen is negative. What is the most appropriate initial diagnostic test?
- A) 24-hour urine catecholamines
- B) Plasma free metanephrines
- C) Aldosterone-to-renin ratio
- D) CT abdomen without contrast
- E) Renal Doppler ultrasound
Answer
B - Plasma free metanephrines
This is the classic pheochromocytoma presentation ("5 Hs": hypertension, headache, hyperhidrosis, hyperglycemia, hypermetabolism). Plasma free metanephrines are the most sensitive test and are preferred for initial screening. 24-hour urine catecholamines and metanephrines are also used but are slightly less sensitive. CT/MRI abdomen follows a positive biochemical test - never image first, since incidental adrenal masses are common and can mislead.
Q5. A patient is taking oral contraceptive pills and develops hypertension. Her BP normalizes after stopping the OCP. Which of the following was the most likely mechanism?
- A) Renin suppression and reduced angiotensin II
- B) Increased aldosterone secretion from adrenal cortex
- C) Estrogen-induced increase in angiotensinogen production
- D) Direct sympathomimetic effect of synthetic progestins
- E) Prostaglandin inhibition leading to sodium retention
Answer
C - Estrogen-induced increase in angiotensinogen
Estrogen stimulates hepatic synthesis of angiotensinogen (renin substrate), leading to increased Ang II and aldosterone levels, causing sodium retention and hypertension. This is 2-3x more common in OCP users. Risk factors include smoking, Black race, obesity, and diabetes. If OCP cannot be stopped, low-dose diuretics are generally effective.
Q6. A 67-year-old man on three antihypertensive medications presents with BP 186/112 mmHg. He has no headache, no visual changes, no chest pain, and no neurologic symptoms. Fundoscopy is normal. Creatinine is at his baseline. What is the most appropriate management?
- A) Admit to ICU, start IV labetalol
- B) Admit to ICU, start IV nitroprusside
- C) Give oral clonidine in the ED and discharge
- D) Intensify oral antihypertensive regimen and arrange close follow-up
- E) Immediate IV nicardipine drip
Answer
D - Intensify oral medications and arrange close follow-up
This is hypertensive urgency - severely elevated BP without acute target organ damage. There is no evidence that rapid reduction in hypertensive urgency improves outcomes. IV medications are not indicated. Overly aggressive reduction risks ischemic stroke, MI, and renal injury (autoregulation is set at higher pressures in chronic hypertension). Outpatient titration of oral medications with follow-up in 1-7 days is appropriate.
Q7. You start lisinopril in a 58-year-old woman with hypertension. Two weeks later, her creatinine rises from 0.9 to 1.8 mg/dL and her BP is lower. What is the most likely explanation?
- A) ACE inhibitor-induced interstitial nephritis
- B) Bilateral renal artery stenosis
- C) Unilateral renal artery stenosis with solitary kidney
- D) Hyperkalemia causing renal tubular dysfunction
- E) Rhabdomyolysis from drug interaction
Answer
B - Bilateral renal artery stenosis
A rise in creatinine after starting an ACE-I or ARB is a classic clue to bilateral renal artery stenosis (or stenosis of an artery to a solitary kidney). When both renal arteries are stenosed, glomerular filtration is maintained by Ang II-dependent efferent arteriolar constriction. Blocking this with ACE-I/ARB drops efferent resistance, precipitously reducing GFR. Stop the ACE-I immediately. Unilateral RAS without a solitary kidney usually does not cause a significant creatinine rise because the contralateral kidney compensates.
Q8. A 62-year-old man with hypertension and gout presents for medication management. Which antihypertensive is most likely to worsen his gout?
- A) Amlodipine
- B) Lisinopril
- C) Hydrochlorothiazide
- D) Losartan
- E) Carvedilol
Answer
C - Hydrochlorothiazide
Thiazide diuretics increase serum uric acid by competing with uric acid for secretion at the proximal tubule, reducing renal uric acid excretion. This worsens hyperuricemia and can precipitate gouty attacks. Of note, losartan (ARB) is actually uricosuric - it has a unique property among antihypertensives of lowering serum uric acid, making it the preferred RAAS agent in hypertensive patients with gout.
Q9. A 38-year-old woman with hypertension is brought to the ED after a cocaine binge. Her BP is 195/115 mmHg and she is anxious and tachycardic. Which medication is contraindicated?
- A) Lorazepam
- B) Phentolamine
- C) Metoprolol
- D) Nicardipine
- E) Nitroprusside
Answer
C - Metoprolol
Beta-blockers are contraindicated in cocaine-induced hypertension. Cocaine blocks norepinephrine reuptake, flooding the synapse with NE that stimulates both alpha and beta receptors. Blocking beta receptors leaves alpha-adrenergic vasoconstriction unopposed, worsening hypertension and potentially causing coronary vasospasm. First-line management is benzodiazepines (treat the central sympathomimetic state) ± phentolamine (alpha-blocker) for refractory hypertension. The same principle applies to other sympathomimetics (amphetamines, ephedrine, pseudoephedrine).
Q10. A 30-year-old woman is 24 weeks pregnant and develops a BP of 150/96 mmHg with 2+ proteinuria. There is no prior history of hypertension. What is the first-line antihypertensive for long-term outpatient management?
- A) Lisinopril
- B) Amlodipine
- C) Methyldopa
- D) Losartan
- E) Spironolactone
Answer
C - Methyldopa
Methyldopa (a central alpha-2 agonist) is the first-line antihypertensive in pregnancy-associated hypertension (gestational HTN or pre-eclampsia). It has the longest safety record in pregnancy. ACE inhibitors and ARBs are absolutely contraindicated (fetotoxic - associated with renal agenesis, oligohydramnios, skull ossification defects). Spironolactone is also contraindicated (anti-androgenic effects on fetus). Labetalol and nifedipine are acceptable alternatives. For acute severe HTN in pregnancy, IV labetalol or IV hydralazine are used.
Q11. A 71-year-old man with hypertension, HFrEF (EF 30%), and atrial fibrillation is being started on antihypertensives. Which drug class is absolutely contraindicated in this patient?
- A) ACE inhibitors
- B) Beta-blockers
- C) Thiazide diuretics
- D) Non-dihydropyridine CCBs (verapamil, diltiazem)
- E) Aldosterone antagonists
Answer
D - Non-dihydropyridine CCBs
Verapamil and diltiazem are contraindicated in HFrEF. They are negative inotropes and can precipitate acute decompensation in patients with reduced systolic function. Dihydropyridine CCBs (amlodipine, felodipine) are acceptable in HFrEF. For this patient with HFrEF + AF, the appropriate agents are ACE-I/ARB, carvedilol or bisoprolol (rate control + HF benefit), loop diuretics, and aldosterone antagonists.
Q12. A patient with hypertension, Type 2 diabetes, and a urine albumin-to-creatinine ratio of 450 mg/g (macroalbuminuria) asks which antihypertensive will best protect his kidneys. What is the most appropriate first-line agent?
- A) Amlodipine
- B) Lisinopril
- C) Hydrochlorothiazide
- D) Metoprolol
- E) Doxazosin
Answer
B - Lisinopril (ACE inhibitor)
ACE inhibitors and ARBs are the preferred first-line agents in diabetic nephropathy and CKD with proteinuria. They reduce intraglomerular pressure by dilating the efferent arteriole (Ang II normally constricts efferent), thereby reducing proteinuria and slowing GFR decline independent of their BP-lowering effect. Do not combine ACE-I + ARB (no added benefit; increases risk of hyperkalemia and AKI per ONTARGET trial).
Q13. According to ACC/AHA classification, which BP reading correctly defines Stage 1 hypertension?
- A) SBP 120-129 and DBP < 80
- B) SBP 130-139 or DBP 80-89
- C) SBP ≥ 140 or DBP ≥ 90
- D) SBP 140-159 or DBP 90-99
- E) SBP ≥ 160 or DBP ≥ 100
Answer
B - SBP 130-139 or DBP 80-89
ACC/AHA classification (used in the US, 2017 and reaffirmed in 2025):
- Normal: < 120 and < 80
- Elevated: 120-129 and < 80
- Stage 1 HTN: 130-139 or 80-89
- Stage 2 HTN: ≥ 140 or ≥ 90
Option D (140-159/90-99) is Grade 1 HTN per the 2024 European ESC classification - different thresholds for the same "Stage 1" concept. Know which system the question uses.
Q14. A 55-year-old man with hypertension on three drugs has a BP of 158/100. Review shows he only takes his medications on clinic days. His home BP log shows readings of 135-140/85-88. What is this phenomenon called?
- A) Masked hypertension
- B) White-coat hypertension
- C) Pseudoresistance due to non-adherence
- D) Resistant hypertension
- E) Labile hypertension
Answer
C - Pseudoresistance due to non-adherence
Non-adherence is the most common cause of apparent resistant hypertension. When medication is taken only on clinic days, office BP is temporarily controlled but home monitoring reveals true uncontrolled HTN. This is pseudoresistance. True resistant HTN requires demonstrated adherence. White-coat HTN is elevated in-office/normal out-of-office in a patient who IS taking medications consistently. Masked HTN is normal in office, elevated outside.
Q15. A patient develops hypertension, truncal obesity, purple abdominal striae, proximal muscle weakness, hyperglycemia, and easy bruising. Which of the following is the most appropriate initial screening test?
- A) 24-hour aldosterone/renin ratio
- B) Plasma free metanephrines
- C) 1 mg overnight dexamethasone suppression test
- D) IGF-1 level
- E) Morning ACTH level
Answer
C - 1 mg overnight dexamethasone suppression test
This is classic Cushing's syndrome. The triad of central obesity, striae, and proximal myopathy with hypertension and hyperglycemia should immediately raise suspicion. Three screening tests are accepted: 1 mg overnight DST (most convenient outpatient test), 24-hour urine free cortisol, or late-night salivary cortisol. ACTH level comes after establishing hypercortisolism (to differentiate ACTH-dependent from ACTH-independent causes). Mechanism of HTN: glucocorticoid activity at mineralocorticoid receptors → sodium and fluid retention.
Q16. A hypertensive patient on hydralazine develops arthralgia, a malar rash, and a positive ANA. Serum complement is low. What is the most appropriate action?
- A) Start hydroxychloroquine for SLE
- B) Increase the hydralazine dose with added steroids
- C) Discontinue hydralazine; switch antihypertensive
- D) Add methotrexate
- E) Perform renal biopsy
Answer
C - Discontinue hydralazine
Hydralazine can cause a drug-induced lupus-like syndrome at high doses, manifesting with arthralgia, malar rash, positive ANA, and low complement. Unlike true SLE, renal involvement is rare and the syndrome resolves upon discontinuation of the drug. This is reversible. Key teaching point: drug-induced lupus also occurs with procainamide, isoniazid, and minocycline. No need for long-term immunosuppression.
Q17. A 48-year-old woman with hypertension takes ibuprofen 800 mg TID for chronic low back pain. Her BP has risen from 128/82 to 144/94 mmHg since starting the NSAID. What is the expected magnitude of BP increase with NSAID use?
- A) 1-2 mmHg
- B) ~5 mmHg
- C) ~10 mmHg
- D) ~15 mmHg
- E) No significant effect
Answer
B - ~5 mmHg
NSAIDs cause a relatively modest average increase in mean BP of 5 mmHg, but can be more pronounced in patients with pre-existing hypertension on antihypertensive medications. The mechanism is prostaglandin inhibition → reduced renal vasodilation, sodium retention, and blunting of antihypertensive drug effects (particularly ACE-I and diuretics). The solution is to substitute acetaminophen or consider topical NSAIDs if possible.
Q18. A 60-year-old Black man with hypertension is started on lisinopril 10 mg daily. At 4-week follow-up, his BP is 158/96 mmHg, unchanged. What is the best next step according to evidence-based guidelines?
- A) Double the lisinopril dose to 20 mg
- B) Add hydrochlorothiazide 12.5 mg
- C) Switch to amlodipine monotherapy
- D) Add amlodipine; consider thiazide as well
- E) Switch to a beta-blocker
Answer
D - Add amlodipine; consider thiazide
In Black patients, ACE inhibitor monotherapy is less effective than in White patients due to lower-renin, volume-dependent HTN patterns. The evidence-based preferred regimen for Black patients is thiazide diuretic + dihydropyridine CCB (the ALLHAT trial demonstrated superiority of chlorthalidone and amlodipine over lisinopril as first-line in this population). Adding amlodipine (and/or chlorthalidone) is the preferred approach. ACE-I/ARBs are still used when there is a compelling indication (DM, CKD, HF) but as monotherapy they provide less BP lowering in this population.
Q19. A patient in the ICU has a BP of 220/130 mmHg with acute pulmonary edema and ST depressions on ECG. Which IV medication is most appropriate?
- A) Hydralazine IV bolus
- B) Labetalol bolus only
- C) IV nitroglycerin infusion
- D) IV nitroprusside infusion
- E) Oral nifedipine
Answer
C - IV nitroglycerin infusion
For hypertensive emergency with concomitant acute coronary syndrome + pulmonary edema, IV nitroglycerin is the agent of choice. It acts as a NO donor with predominantly venodilatory effects (reducing preload), relieves pulmonary congestion, and dilates coronary arteries. Nitroprusside is a NO donor with more arterial dilation and is better for pure hypertensive encephalopathy; it has risk of coronary steal in ACS. Oral nifedipine is never appropriate in emergencies (rapid, uncontrolled drops). Hydralazine causes reflex tachycardia, worsening ischemia.
Q20. A patient with hypertension undergoes ABPM. During the day, average BP is 148/92. During sleep, average BP is 145/90 mmHg (a fall of only 2%). How does this pattern affect cardiovascular risk?
- A) Normal sleep pattern; no added risk
- B) Non-dipper pattern; associated with increased cardiovascular risk
- C) Reverse dipper; BP paradoxically rises at night
- D) White-coat effect during monitoring
- E) No clinical significance if daytime BP is controlled
Answer
B - Non-dipper; increased cardiovascular risk
Normally, BP falls 10-20% during sleep (the "dipping" pattern). A fall of < 10% defines a non-dipper, which is associated with higher rates of stroke, myocardial infarction, LVH, and renal damage independent of the absolute BP level. A reverse dipper (nocturnal BP actually higher than daytime) carries the highest risk. ABPM is the only way to identify this pattern. OSA, CKD, and autonomic dysfunction are common causes of non-dipping.
Q21. A 40-year-old woman with hypertension and a BMI of 42 has a BP of 162/102 mmHg despite maximum doses of amlodipine and lisinopril. She is adherent to medication. What is the most evidence-based fourth agent to add?
- A) Doxazosin
- B) Clonidine
- C) Spironolactone
- D) Hydralazine
- E) Minoxidil
Answer
C - Spironolactone
Spironolactone (a mineralocorticoid antagonist) has the strongest evidence as add-on therapy for resistant hypertension. The PATHWAY-2 trial demonstrated spironolactone was significantly superior to doxazosin and bisoprolol as the fourth drug in resistant HTN. The rationale is that occult primary aldosteronism or excess aldosterone effect is common in resistant HTN. Before adding, confirm adherence and rule out secondary causes, particularly primary aldosteronism. Monitor potassium carefully.
Q22. A 25-year-old man with hypertension and no family history is found to have an abdominal bruit on exam. Renal Doppler shows turbulent flow in the right renal artery. Angiography reveals a "string of beads" pattern. What is the most likely etiology?
- A) Atherosclerotic renal artery stenosis
- B) Fibromuscular dysplasia
- C) Polyarteritis nodosa
- D) Renal cell carcinoma compressing the artery
- E) Takayasu arteritis
Answer
B - Fibromuscular dysplasia (FMD)
The "string of beads" pattern on angiography is pathognomonic for FMD, which affects the medial layer of arteries. FMD is the most common cause of renal artery stenosis in young women and children. In contrast, atherosclerosis is the dominant cause in older adults and produces proximal, ostial lesions. FMD also occurs in carotid and vertebral arteries (can cause dissection or stroke in young patients). Treatment options include percutaneous transluminal angioplasty (preferred over stenting in FMD) or ACE-I/ARB.
Q23. A hypertensive patient presents with BP 195/125 mmHg, altered mental status, severe headache, and papilledema. CT head shows no hemorrhage or infarct. What is the immediate BP target for the first hour of treatment?
- A) Normalize BP to < 120/80 within 1 hour
- B) Reduce SBP to < 120 within minutes
- C) Reduce MAP by no more than 25% within the first hour
- D) Reduce SBP to 140 mmHg within 30 minutes
- E) No reduction until cause identified
Answer
C - Reduce MAP by no more than 25% in the first hour
For most hypertensive emergencies, the target is a MAP reduction of ≤ 25% in the first 1 hour, then toward 160/100 over 2-6 hours, then gradual normalization over 24-48 hours. Rapid BP reduction in patients with chronic hypertension is dangerous because cerebral, coronary, and renal autoregulation is reset to higher pressures - too rapid a drop causes ischemia. The one major exception is aortic dissection, where SBP must be rapidly reduced to < 120 mmHg within minutes using IV esmolol + vasodilator.
Q24. A 55-year-old man with newly diagnosed hypertension has a BP of 144/88 mmHg. His 10-year ASCVD risk is 6%. He has no DM, CKD, or other comorbidities. What is the most appropriate initial management per current guidelines?
- A) Start two antihypertensive drugs immediately
- B) Start one antihypertensive drug (ACE-I or ARB preferred)
- C) Lifestyle modifications alone for 3-6 months; reassess
- D) Immediate referral to nephrology
- E) 24-hour ambulatory BP monitoring before any treatment
Answer
C - Lifestyle modifications alone for 3-6 months
For Stage 1 HTN (130-139/80-89) in patients with low ASCVD risk (< 10%) and no compelling indications, current ACC/AHA guidelines recommend a trial of lifestyle modifications (DASH diet, sodium restriction, weight loss, exercise, alcohol reduction) for 3-6 months before initiating pharmacotherapy. Drug therapy is indicated at Stage 1 if ASCVD risk ≥ 10%, or if the patient has diabetes, CKD, established CVD, or Stage 2 HTN (≥ 140/90). BP of 144/88 = Stage 2 would warrant medication, but 130-139/80-89 at low risk = lifestyle first.
(Note: This patient's BP of 144/88 technically crosses into Stage 2 on the systolic - in practice, Stage 2 warrants medication initiation. The principle of lifestyle-first at Stage 1 low-risk is the key testable point.)
Q25. A 33-year-old woman with pheochromocytoma is scheduled for adrenalectomy. She is started on phenoxybenzamine (alpha-blocker) preoperatively. A week later, she develops tachycardia of 110 bpm. What should be added next?
- A) Increase the phenoxybenzamine dose
- B) Add a beta-blocker (propranolol)
- C) Add verapamil
- D) Add labetalol as sole agent first
- E) Nothing; tachycardia is expected and benign
Answer
B - Add a beta-blocker AFTER alpha-blockade is established
The critical rule in pheochromocytoma preoperative preparation: always establish alpha-blockade first, then add beta-blockade if needed for tachycardia. If a beta-blocker is given first (or alone), it blocks the vasodilatory beta-2 receptors in peripheral vessels, leaving alpha-mediated vasoconstriction unopposed - precipitating a hypertensive crisis. Once adequate alpha-blockade is in place (typically 7-14 days), a beta-blocker can be safely added to control the reflex tachycardia. Phenoxybenzamine is the preferred preoperative alpha-blocker (irreversible, long-acting).
Quick Score Key
| Q# | Answer | Topic Tested |
|---|---|---|
| 1 | C | Coarctation of aorta |
| 2 | C | OSA as cause of resistant HTN |
| 3 | C | Primary aldosteronism workup |
| 4 | B | Pheochromocytoma diagnosis |
| 5 | C | OCP-induced HTN mechanism |
| 6 | D | HTN urgency vs. emergency management |
| 7 | B | Bilateral RAS + ACE-I |
| 8 | C | Thiazide + gout; losartan is uricosuric |
| 9 | C | Cocaine - no beta-blockers |
| 10 | C | Methyldopa in pregnancy |
| 11 | D | Non-DHP CCBs contraindicated in HFrEF |
| 12 | B | ACE-I in diabetic nephropathy |
| 13 | B | ACC/AHA classification |
| 14 | C | Pseudoresistance - non-adherence |
| 15 | C | Cushing's syndrome screening |
| 16 | C | Hydralazine-induced lupus |
| 17 | B | NSAID effect on BP |
| 18 | D | Black patients - thiazide + CCB preferred |
| 19 | C | HTN emergency + ACS - nitroglycerin |
| 20 | B | Non-dipping pattern |
| 21 | C | Spironolactone for resistant HTN |
| 22 | B | FMD - string of beads |
| 23 | C | MAP reduction target in emergency |
| 24 | C | Lifestyle first at Stage 1 low risk |
| 25 | B | Pheo preop - alpha before beta |
Hi
Hi! How can I help you today?
Internal medicine: cardiovascular hypertension super detailed exam oriented notes made easy
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Hypertension internal medicine simplified made easy as per priyanka sachdev
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.