Addison disease
Reading File
Finding Sources
Searching PubMed
"Addison disease" OR "primary adrenal insufficiency"
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information to provide a detailed, well-illustrated answer on Addison disease. Let me compile it.
Addison Disease (Primary Adrenocortical Insufficiency)
Definition
Addison disease is primary adrenocortical insufficiency caused by destruction or dysfunction of the adrenal cortex, resulting in deficiency of all three classes of adrenocortical hormones: glucocorticoids (cortisol), mineralocorticoids (aldosterone), and adrenal androgens (DHEA, androstenedione).
- Costanzo Physiology 7th Ed., p. 440
- Tietz Textbook of Laboratory Medicine 7th Ed.
Epidemiology
- Affects approximately 1 in 10,000 individuals in developed countries
- Autoimmune adrenalitis most common cause in adults (developed world); tuberculosis is the most common cause worldwide
- Most common presentation between ages 30-50 years
- In children, >80% of cases are genetic in origin
Etiology & Causes
| Category | Examples |
|---|---|
| Autoimmune | Autoimmune adrenalitis (most common in developed world); often part of APS type 2 |
| Infectious | Tuberculosis (most common worldwide), histoplasmosis, CMV, Meningococcal sepsis (Waterhouse-Friderichsen syndrome) |
| Neoplastic | Bilateral adrenal metastases (lung, breast, melanoma), lymphoma |
| Vascular | Bilateral adrenal hemorrhage (Waterhouse-Friderichsen syndrome, anticoagulants, heparin-induced thrombocytopenia) |
| Infiltrative | Amyloidosis, hemochromatosis, sarcoidosis |
| Genetic | CAH (21-hydroxylase deficiency), adrenoleukodystrophy (X-linked - important in young boys) |
| Drugs | Ketoconazole, fluconazole, etomidate, rifampicin, certain anticancer agents |
Autoimmune polyendocrine syndromes (APS):
- APS type 2 (~70% of autoimmune Addison cases) - autosomal dominant, HLA-DRB1 mutation on chromosome 6p21.32; also associated with type 1 diabetes, autoimmune thyroiditis, celiac disease
- APS type 1 (~10%) - autosomal recessive AIRE gene mutation (chromosome 21q22.3); triad of candidiasis, hypoparathyroidism, Addison disease
Note: In young boys with Addison disease, always consider adrenoleukodystrophy (ABCD1 gene mutation) - hyperpigmentation may precede neurological signs by years; check very-long-chain fatty acid levels.
Pathophysiology
Destruction of all zones of the adrenal cortex leads to:
- Glucocorticoid (cortisol) deficiency → hypoglycemia, anorexia, weight loss, nausea, vomiting, weakness, fatigue
- Mineralocorticoid (aldosterone) deficiency → hyponatremia, hyperkalemia, metabolic acidosis, hypotension (reduced ECF volume), high renin levels
- Adrenal androgen deficiency → in women: decreased pubic and axillary hair, reduced libido
- Compensatory ACTH elevation (due to loss of cortisol negative feedback on the pituitary) → ACTH contains the α-MSH fragment → hyperpigmentation
Clinical Features
Chronic Symptoms
- Fatigue, weakness, malaise
- Anorexia, weight loss, nausea, vomiting, diarrhea
- Hypotension (orthostatic or frank)
- Salt craving
- Psychosis, depression, cognitive symptoms
- In women: loss of axillary and pubic hair, decreased libido
Hallmark Sign - Hyperpigmentation

- Diffuse hyperpigmentation, most prominent in sun-exposed areas, pressure points (elbows, knees), nail beds, nipples, areolae, and recent scars
- Palmar crease darkening, darkening of mucous membranes, nevi, and hair
- Multifocal oral melanoacanthoma may occur
- Eruptive onset of multiple new nevi can be an early sign
- Occasionally absent ("white Addison disease")
- Key distinction from secondary adrenal insufficiency: hyperpigmentation does NOT occur in secondary (pituitary/hypothalamic) causes because ACTH levels are low or normal, not elevated
Cardiovascular Findings (Braunwald's Heart Disease)
- Low diastolic BP (<60 mmHg) with orthostatic changes
- ECG: low-amplitude P waves and peaked T waves (from hyperkalemia)
- Reduced LV end-systolic and end-diastolic dimensions
- Can progress to cardiovascular collapse
Laboratory Findings
| Test | Finding in Addison Disease |
|---|---|
| Serum cortisol (AM) | Low (<5 µg/dL = abnormal) |
| Plasma ACTH | Elevated (primary) vs. low/normal (secondary) |
| Serum sodium | Low (hyponatremia) |
| Serum potassium | High (hyperkalemia) |
| Blood glucose | Low (hypoglycemia) |
| Serum calcium | High (hypercalcemia) |
| Acid-base | Metabolic acidosis |
| Plasma renin | Elevated |
| Aldosterone | Low |
Diagnosis
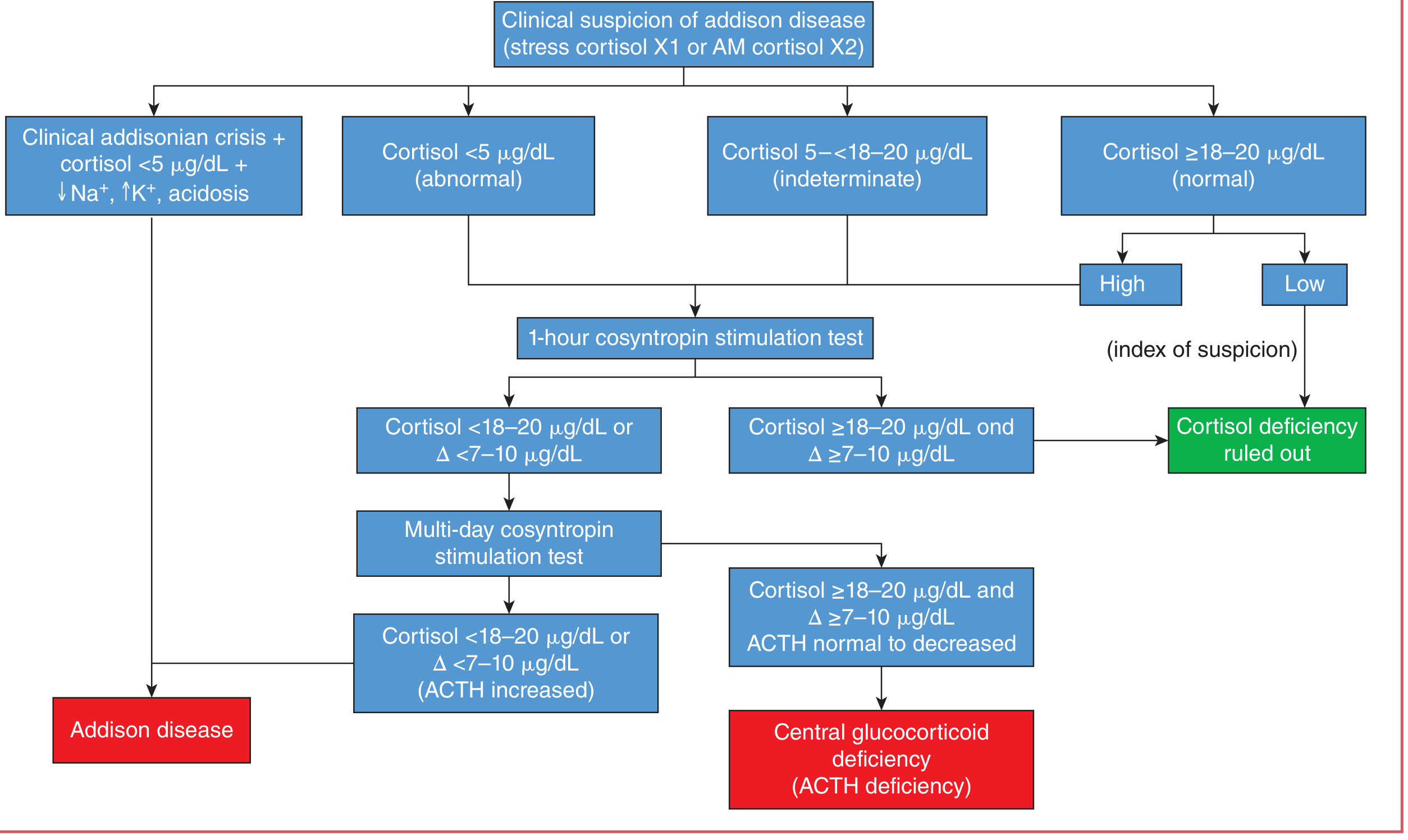
Step-by-step approach:
- Obtain morning plasma cortisol (and ACTH simultaneously)
- Cortisol <5 µg/dL = abnormal → proceed to confirmation
- Cortisol 5-18 µg/dL = indeterminate → cosyntropin (ACTH) stimulation test
- Cosyntropin 250 µg IV; measure cortisol at 30 and 60 min
- Normal response: cortisol rises to ≥18-20 µg/dL (some sources use 550 nmol/L) with delta ≥7-10 µg/dL
- Abnormal response + elevated ACTH = Addison disease (primary)
- Abnormal response + normal/decreased ACTH = central (secondary) glucocorticoid deficiency
- If clinical Addisonian crisis is already present (cortisol <5 µg/dL + hyponatremia + hyperkalemia + acidosis) - diagnosis is established clinically; begin treatment immediately
- CT adrenal glands to exclude infiltration, hemorrhage, or infection
Addisonian Crisis (Acute Adrenal Insufficiency)
A life-threatening emergency triggered by physiologic stress (infection, trauma, surgery) in a patient with undiagnosed or undertreated adrenal insufficiency, or abrupt withdrawal of chronic steroids.
Presentation: Circulatory collapse, severe hypotension, fever, abdominal pain, vomiting, extreme weakness, altered consciousness
Management (Braunwald's Heart Disease):
- Hydrocortisone 100 mg IV bolus immediately
- Then 100 mg IV every 8-12 hours for first 24 hours
- Taper over 72-96 hours as patient stabilizes
- Large volumes of normal saline + 5% dextrose to address volume deficit and hypoglycemia
- Identify and treat precipitating cause (infection, ischemia, intra-abdominal emergency)
Long-Term Treatment
| Hormone Replaced | Drug | Dose |
|---|---|---|
| Glucocorticoid | Hydrocortisone | 15-20 mg/day in 2 divided doses (larger AM dose to mimic diurnal rhythm) |
| Prednisone | 5 mg/day once or twice daily | |
| Mineralocorticoid | Fludrocortisone | 0.05-0.2 mg/day orally |
- Dual-release hydrocortisone preparations can better mimic the cortisol circadian rhythm
- Sick day rules: patients must double (or triple) their glucocorticoid dose during illness, injury, or surgery
- Patients should carry a steroid emergency card and injectable hydrocortisone for emergencies
- Secondary (pituitary) adrenal insufficiency does not require mineralocorticoid replacement (aldosterone production relatively preserved)
Secondary vs. Primary Adrenal Insufficiency - Key Differences
| Feature | Primary (Addison) | Secondary (Pituitary/Hypothalamic) |
|---|---|---|
| ACTH | High | Low or normal |
| Hyperpigmentation | Yes | No |
| Mineralocorticoid deficiency | Yes | No (aldosterone preserved) |
| Electrolyte disturbance | Hyponatremia + hyperkalemia | Usually hyponatremia only |
| Cause | Adrenal gland destruction | Pituitary/hypothalamic disease, long-term steroid use |
Recent Evidence (2024-2026)
Two recent systematic reviews and meta-analyses are worth noting:
- A 2024 meta-analysis (PMID 39277840) found increased rates of adverse pregnancy and fetal outcomes in women with primary adrenal insufficiency - relevant for counseling reproductive-age women
- A 2025 meta-analysis (PMID 40966723) confirmed increased all-cause mortality in primary adrenal insufficiency compared to the general population, underscoring the importance of optimal replacement and education
Sources: Costanzo Physiology 7th Ed. | Tietz Textbook of Laboratory Medicine 7th Ed. | Andrews' Diseases of the Skin | Braunwald's Heart Disease | Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.