Hi
Hello! How can I help you today?
Male reproductive system in adult health nursing 2 bsc nursing explain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Now I have comprehensive content. Let me compile a thorough BSc Nursing-level explanation of the male reproductive system.
Male Reproductive System — Adult Health Nursing (BSc Nursing 2nd Year)
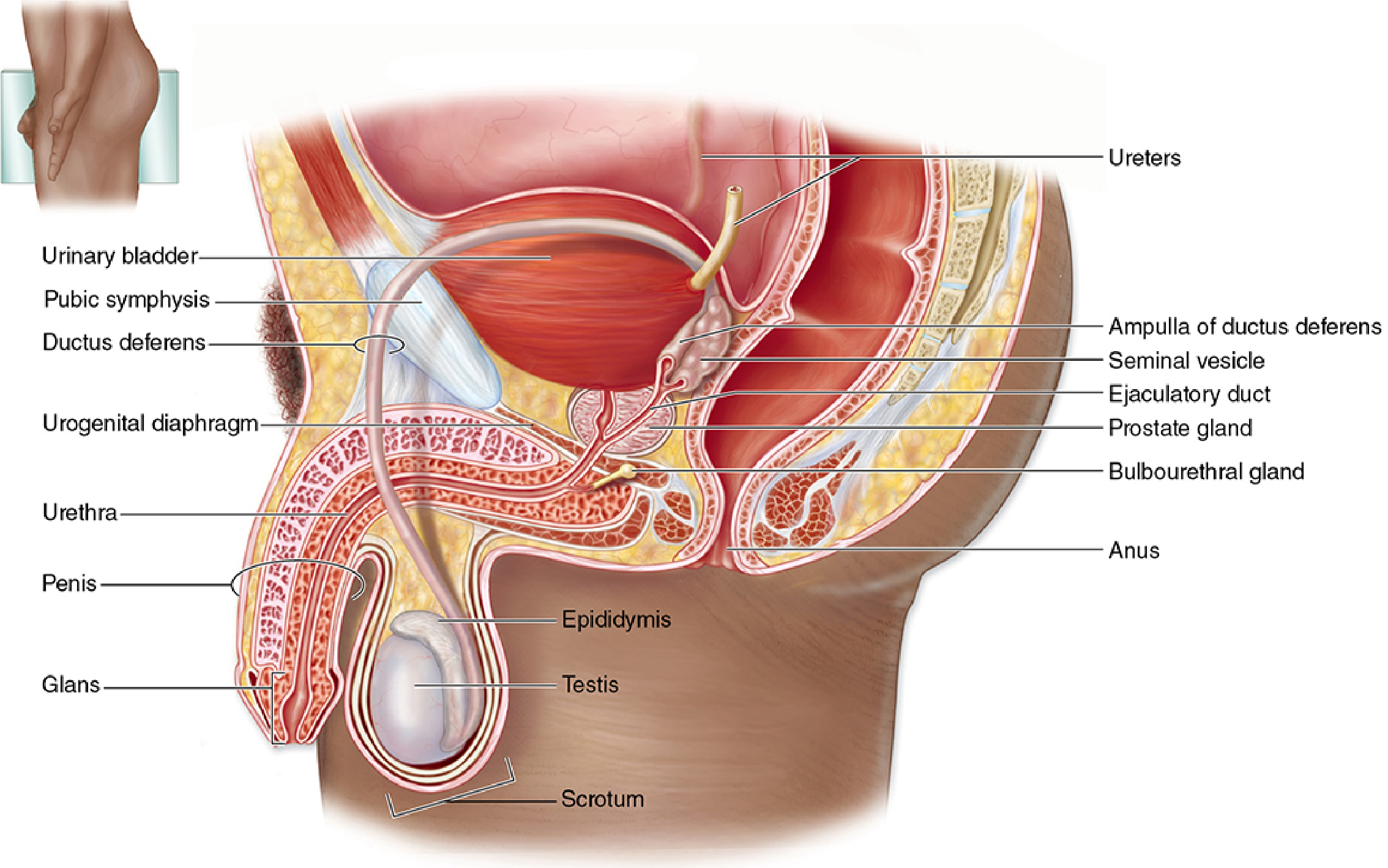
1. Overview
The male reproductive system consists of four main components:
- Testes (gonads) — produce spermatozoa and testosterone
- Genital ducts — transport spermatozoa (epididymis, vas deferens, ejaculatory ducts)
- Accessory glands — seminal vesicles, prostate, bulbourethral glands
- Penis — copulatory and excretory organ
2. Testes
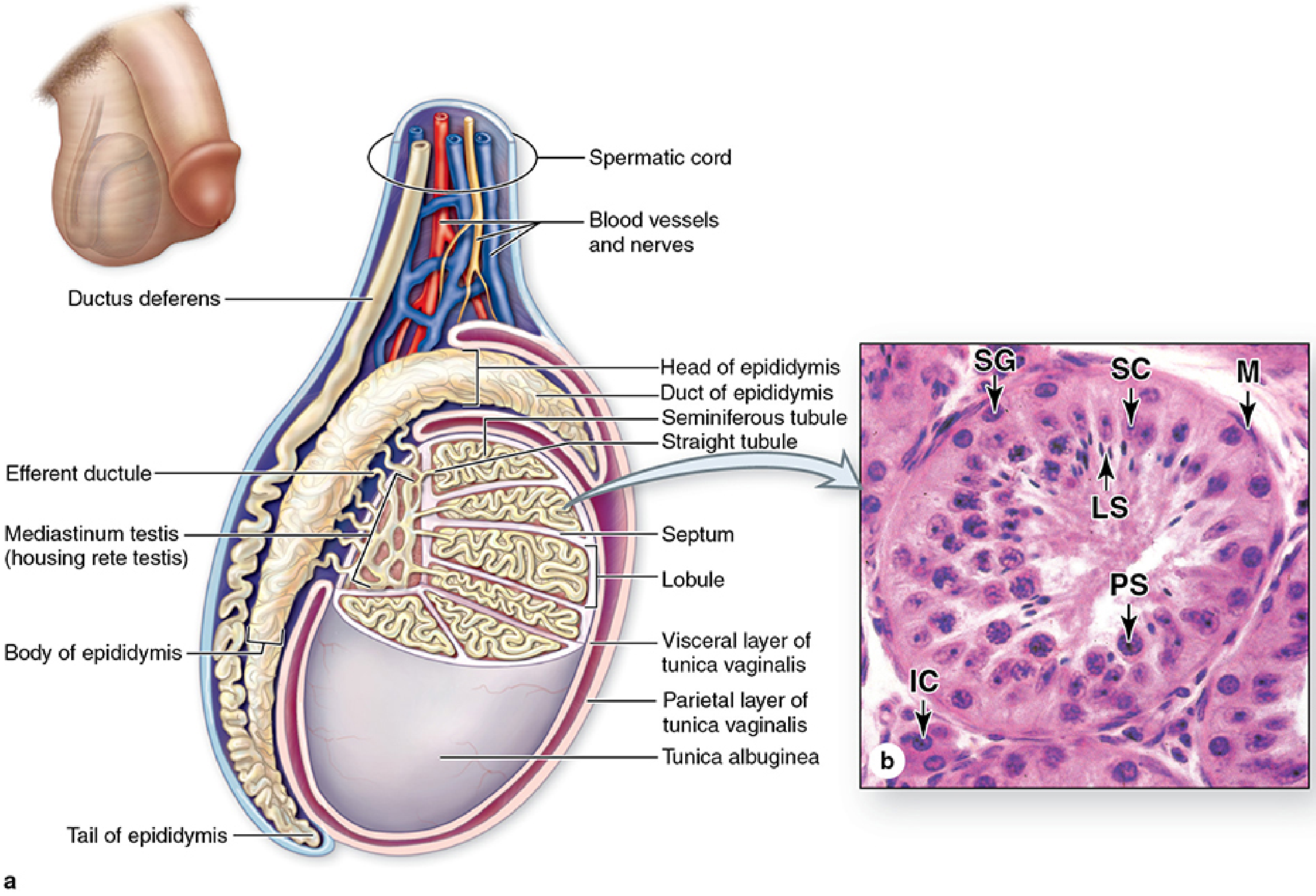
Structure
- Each testis is enclosed in a dense connective tissue capsule called the tunica albuginea, which thickens posteriorly to form the mediastinum testis
- Septa from the mediastinum divide each testis into ~250 pyramidal lobules, each containing 1–4 seminiferous tubules
- The testes descend into the scrotum during fetal life, bringing a peritoneal sac (the tunica vaginalis)
Temperature Regulation
Sperm production requires ~34°C (lower than core body temperature of 37°C). This is maintained by:
- Sweat evaporation from scrotal skin
- Pampiniform plexus — a venous network surrounding the testicular artery in the spermatic cord; acts as a countercurrent heat exchanger
- Dartos muscle (scrotum) and cremaster muscle (spermatic cord) — contract or relax to move testes closer to or away from the body
Leydig Cells (Interstitial Cells)
- Located between seminiferous tubules
- Large polygonal cells with abundant smooth endoplasmic reticulum (SER) and mitochondria
- Produce testosterone under stimulation by LH (ICSH — Interstitial Cell Stimulating Hormone) from the anterior pituitary
Clinical Conditions
| Condition | Description |
|---|---|
| Cryptorchidism | Failure of testes to descend; bilateral form causes infertility if not surgically corrected by age 2–3 years |
| Hydrocele | Accumulation of serous fluid in the tunica vaginalis; most common cause of scrotal swelling |
3. Spermatogenesis
Spermatogenesis is the process by which diploid germ cells develop into haploid spermatozoa, occurring within the seminiferous tubules.
Stages
| Stage | Cell Type | Location in Tubule | Description |
|---|---|---|---|
| Mitosis | Spermatogonia (Type A & B) | Periphery (basal) | Self-renewal and production of primary spermatocytes |
| Meiosis I | Primary → Secondary spermatocytes | Mid-zone | Reduces chromosome number by half |
| Meiosis II | Secondary spermatocytes → Spermatids | Closer to lumen | Further division to form haploid spermatids |
| Spermiogenesis | Spermatids → Spermatozoa | Lumen | Differentiation; no cell division |
Sertoli Cells
- Columnar "nurse cells" lining the seminiferous tubule
- Form the blood-testis barrier (tight junctions between adjacent Sertoli cells), protecting developing sperm from immune attack
- Secrete androgen-binding protein (ABP) to concentrate testosterone near developing sperm
- Produce inhibin B — a feedback inhibitor of FSH from the pituitary
- Phagocytose excess cytoplasm shed during spermiogenesis
Spermiogenesis (key steps)
- Golgi phase — acrosomal vesicles form; flagellum begins to develop
- Cap phase — acrosomal cap covers ~half the nucleus; nucleus condenses
- Acrosome phase — nucleus elongates; mitochondria aggregate around midpiece (ATP for flagellar motion)
- Maturation phase — excess cytoplasm shed; mature spermatozoon released into lumen
The acrosome is a lysosome-like structure at the sperm head containing hyaluronidase and acrosin — enzymes released during the acrosomal reaction to penetrate the zona pellucida of the ovum.
4. Hypothalamic-Pituitary-Gonadal (HPG) Axis
Hypothalamus
↓ GnRH (pulsatile)
Anterior Pituitary
↓ LH ↓ FSH
Leydig cells Sertoli cells
(Testosterone) (Spermatogenesis + Inhibin B)
↓ Negative feedback
Hypothalamus & Pituitary
- GnRH (decapeptide) — secreted in pulses from arcuate nucleus; stimulates pituitary gonadotrophs
- LH → stimulates Leydig cells → testosterone production
- FSH → stimulates Sertoli cells → supports spermatogenesis
- Testosterone → negative feedback on hypothalamus and pituitary
- Inhibin B → specifically inhibits FSH secretion
Actions of Testosterone
- Development of male secondary sexual characteristics (body hair, voice deepening, muscle mass)
- Activation and maintenance of spermatogenesis
- Development and maintenance of male sex accessory organs
- Anabolic effects (bone, muscle)
- Libido and behavior
5. Genital Ducts
Epididymis
- A single, tightly coiled duct (~6 m long) on the posterior surface of each testis
- Divided into head (caput), body (corpus), tail (cauda)
- Function: sperm maturation and storage (~12–20 days transit time)
- Sperm acquire motility and fertilizing capacity during epididymal transit
- Pseudostratified columnar epithelium with stereocilia (microvilli) that absorb fluid and resorb excess cytoplasm
Vas Deferens (Ductus Deferens)
- A thick-walled muscular tube that ascends in the spermatic cord
- Expands into an ampulla near the bladder before joining the seminal vesicle duct
- At ejaculation: strong peristaltic contractions propel spermatozoa toward the urethra
- Vasectomy (surgical contraception) — vas deferens is cut or ligated
Ejaculatory Ducts
- Formed by the union of the ampulla of the vas deferens and the duct of the seminal vesicle
- Pass through the prostate gland and open into the prostatic urethra
6. Accessory Glands
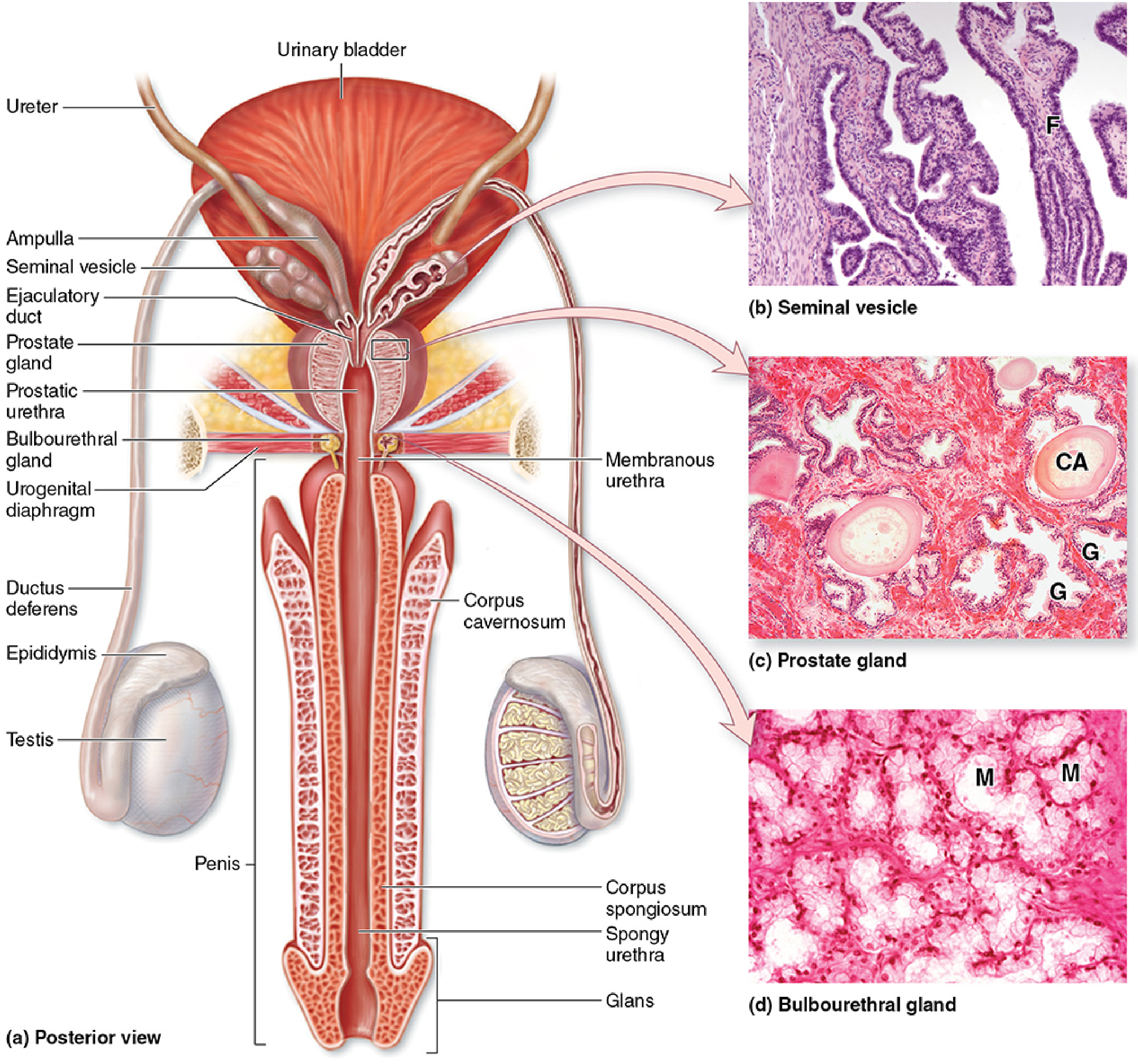
Seminal Vesicles
- Two highly tortuous tubes (~15 cm each), posterior to the bladder
- Produce ~70% of ejaculate volume (2–5 mL total)
- Secretion contains:
- Fructose — main energy source for sperm
- Prostaglandins — stimulate female reproductive tract contractions
- Fibrinogen — causes semen to coagulate after ejaculation
- Citrate, inositol, ascorbic acid
Prostate Gland
- Weight ~20 g in adult; surrounds the urethra just below the bladder
- Contains 30–50 tubuloacinar glands embedded in fibromuscular stroma
- Secretion (~25% of ejaculate) contains:
- Prostate-Specific Antigen (PSA) — serine protease that liquefies semen
- Zinc, citric acid, acid phosphatase
- Antibacterial properties
- Prostate is divided into peripheral zone (most common site of carcinoma), transitional zone (site of BPH), and central zone
- Contains corpora amylacea (calcified concretions) — increases with age
Bulbourethral Glands (Cowper's Glands)
- Paired, pea-sized mucous glands at the base of the penis
- Secrete a clear, alkaline, mucoid fluid before ejaculation
- Lubricates the urethra and neutralizes residual urinary acidity
7. Semen Composition
| Component | Source | Volume |
|---|---|---|
| Spermatozoa | Testes | <1% |
| Seminal vesicle secretion | Seminal vesicles | ~70% |
| Prostatic secretion | Prostate | ~25% |
| Bulbourethral + urethral glands | BUG + urethral glands | ~5% |
Normal semen parameters (WHO 2021):
- Volume ≥ 1.4 mL
- Sperm concentration ≥ 16 million/mL
- Total motility ≥ 42%
- Normal morphology ≥ 4%
8. Penis
- Contains two corpora cavernosa (erectile tissue) and one corpus spongiosum (surrounds the urethra)
- Glans penis — distal expansion of corpus spongiosum; covered by prepuce (foreskin) if not circumcised
- Erection: parasympathetic stimulation → NO (nitric oxide) release → smooth muscle relaxation → vasodilation → engorgement of erectile tissue
- Ejaculation: sympathetic stimulation → peristalsis of vas deferens and accessory glands; somatic nerves → rhythmic contractions of bulbospongiosus muscle
9. Common Disorders — Nursing Relevance
| Disorder | Key Features | Nursing Considerations |
|---|---|---|
| Benign Prostatic Hyperplasia (BPH) | Enlargement of transitional zone; urinary obstruction | Monitor voiding patterns, post-void residual; pre/post-op care for TURP |
| Prostate Cancer | Peripheral zone; elevated PSA | Patient education on PSA screening, biopsy care, hormone therapy side effects |
| Testicular Cancer | Most common solid tumour in men 15–35 years | Teach testicular self-examination (TSE); post-orchidectomy care |
| Epididymo-orchitis | Infection of epididymis ± testis; often STI | Administer antibiotics, scrotal support, pain management |
| Erectile Dysfunction (ED) | Vascular, neurological, hormonal, psychological | Therapeutic communication, medication education (PDE5 inhibitors) |
| Varicocele | Dilated pampiniform plexus; affects sperm quality | Pre-surgical education; fertility counseling |
10. Nursing Assessment of Male Reproductive Health
- History: urinary symptoms (frequency, hesitancy, weak stream), sexual function, STI history, fertility concerns, pain
- Physical examination: inspection and palpation of scrotum, testes (note size, symmetry, tenderness), inguinal nodes
- Investigations:
- PSA (prostate-specific antigen)
- Semen analysis
- Scrotal ultrasound — testicular masses, varicocele
- Urinalysis / urine culture
- Testosterone levels
- Health education:
- Testicular self-examination monthly
- Safe sexual practices
- Scrotal hygiene
- Prompt reporting of scrotal pain, swelling, or urinary changes
Sources:
- Medical Physiology (Boron & Boulpaep), pp. 1593–1595
- Junqueira's Basic Histology: Text and Atlas, 17e, pp. 1055–1090
This is a shared conversation. Sign in to Orris to start your own chat.