Tuberculosis : include all aspects pathology, microbiology, pharmacology
Reading File
Finding Sources
Searching PubMed
tuberculosis treatment guidelines
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Tuberculosis - Comprehensive Review
1. MICROBIOLOGY
The Organism
Mycobacterium tuberculosis belongs to the M. tuberculosis complex (MTBC) - a group of highly related species. Members include:
- M. tuberculosis and M. africanum - obligate human pathogens, no environmental reservoir
- M. bovis (cattle), M. caprae (goats/sheep), M. pinnipedii (sea lions) - animal-adapted
M. tuberculosis is a nonmotile, non-spore-forming, facultative anaerobe that is rod-shaped, approximately 2-4 µm in length. - Goldman-Cecil Medicine, p. 3246
Key Structural Features
| Feature | Detail |
|---|---|
| Cell wall layers | Plasma membrane → peptidoglycan → arabinogalactan → outer membrane → capsule |
| Outer membrane | Contains mycolic acids (β-hydroxylated fatty acids, chains up to 90 carbons), trehalose dimycolates, phthiocerol dimycocerosate, sulfolipids |
| Growth rate | Doubles every 18-24 hours (very slow - cultures take weeks) |
| Staining | Acid-fast - retains carbol fuchsin after washing with strong acid-alcohol |
The waxy mycolic acid coat creates a formidable barrier to antibiotic entry and is central to virulence. The MTBC genome is ~4.4 × 10⁶ nucleotides, GC-rich (65.6%), with ~4000 open reading frames. - Murray & Nadel's Respiratory Medicine, p. 1174
Acid-Fast Staining
The mycolic acid-rich cell wall prevents decolorization of carbol fuchsin after acid-alcohol washing - the basis of the Ziehl-Neelsen (ZN) stain and the fluorochrome (auramine-rhodamine) stain. Organisms appear as bright red rods on ZN and fluorescent on auramine staining.
Transmission
- Airborne route via droplet nuclei (1-5 µm diameter) produced by coughing, sneezing, or speaking
- Humans are the only significant reservoir
- Small particles reach the alveoli and initiate infection
Culture & Identification
- Löwenstein-Jensen (LJ) medium - solid egg-based, takes 3-8 weeks
- BACTEC MGIT 960 - liquid broth, faster (1-3 weeks)
- GeneXpert MTB/RIF (Xpert) - rapid molecular test detecting MTB DNA and rifampicin resistance within 2 hours; WHO-endorsed first-line diagnostic
- Drug susceptibility testing (DST) - mandatory for all confirmed cases
2. PATHOLOGY
Sequence of Events in Primary TB
The natural history unfolds in two phases:
Phase 1 - First 3 weeks (before CMI):
Mycobacteria are inhaled and reach alveoli → engulfed by alveolar macrophages via mannose receptors and complement receptor CR3 → the organisms prevent phagosome-lysosome fusion (maturation arrest, lack of acidification, lack of reactive nitrogen/oxygen species) → unchecked intracellular replication → bacteremia with seeding of multiple sites. Most individuals are asymptomatic at this stage. - Robbins Basic Pathology, p. 474
Phase 2 - After 3 weeks (CMI activation):
Mycobacterial antigens reach draining lymph nodes → processed and presented to CD4+ T cells by dendritic cells and macrophages → under influence of IL-12, a Th1 response is generated → Th1 cells secrete IFN-γ.
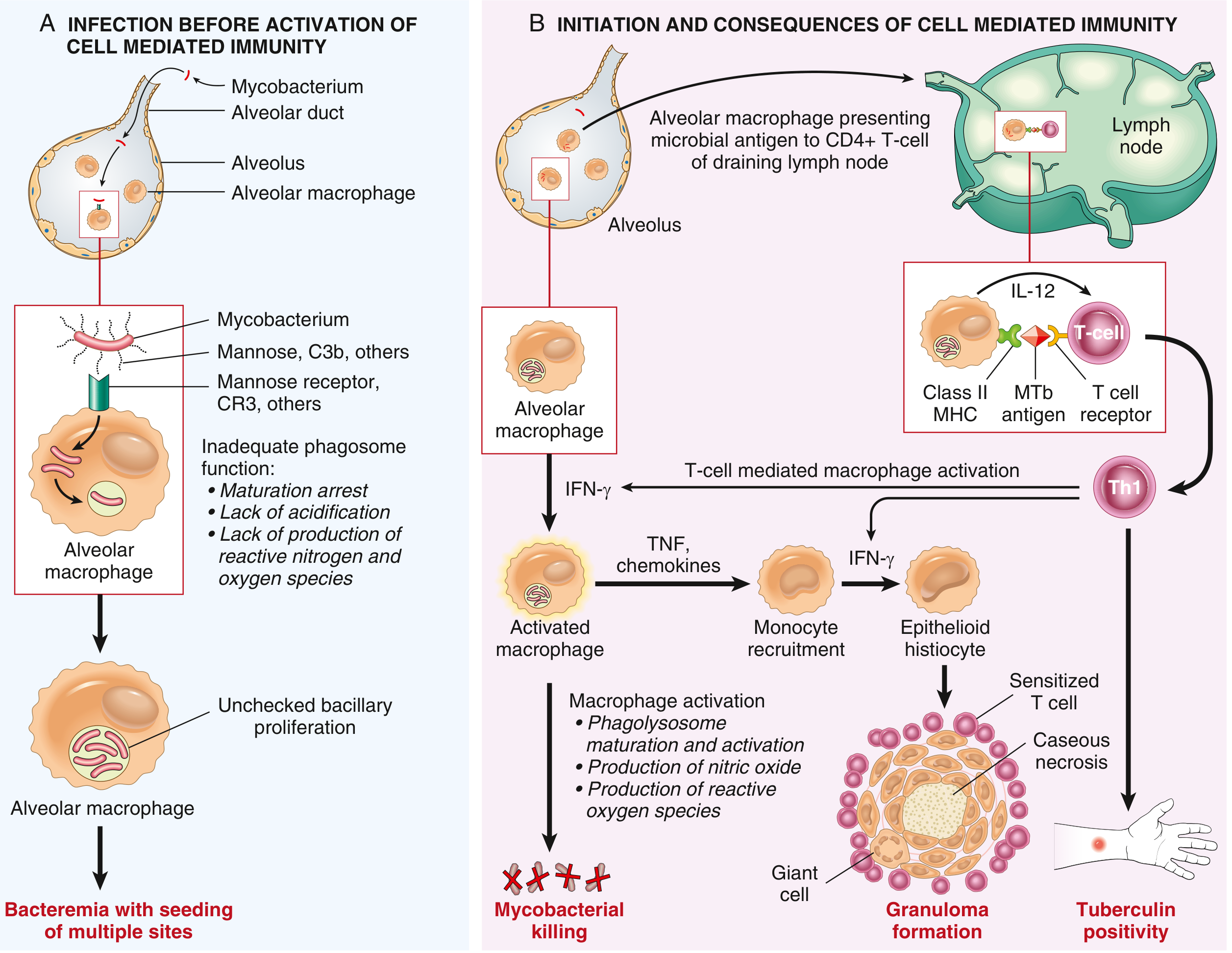
Fig: The two phases of primary TB - (A) early bacteremia before CMI, (B) IFN-γ-driven macrophage activation, granuloma formation, and tuberculin positivity. (Robbins Basic Pathology)
Granuloma Formation - The Core Pathological Lesion
IFN-γ activates macrophages, which:
- Release TNF → recruits monocytes
- Upregulate iNOS → nitric oxide → kills mycobacteria
- Release antimicrobial peptides (defensins)
- Differentiate into epithelioid histiocytes → aggregate into granulomas
- Some epithelioid cells fuse → Langhans giant cells (nuclei arranged at periphery)
Classic TB granuloma (tubercle):
- Central caseous necrosis - soft, cheese-like material (cheese = caseus in Latin)
- Surrounded by epithelioid macrophages
- Langhans giant cells at the periphery
- Rim of lymphocytes and monocytes
- Outer fibrous capsule
Histologically: "Active lesions show characteristic coalescent nodules with central caseation. Although tubercle bacilli can be demonstrated in early exudative and caseous phases, it is usually impossible to find them in the late fibrocalcific stages." - Robbins Basic Pathology, p. 475
Why caseation occurs: Unlike sarcoidosis (non-caseating), TB granulomas undergo central necrosis due to the DTH (delayed-type hypersensitivity) response against mycobacterial antigens, mediated by CD4 Th1 cells. The cell-mediated hypersensitivity is responsible for cavitation, caseation, and general toxemia. - Roitt's Essential Immunology
Ghon Complex (Primary TB)
- Ghon focus: initial subpleural parenchymal lesion, usually in the mid-lower lung zones
- Ghon complex = Ghon focus + ipsilateral hilar lymphadenopathy
- Ranke complex = calcified Ghon complex (healed primary TB)
In most immunocompetent individuals, the immune response halts infection before significant illness → latent TB infection (LTBI).
Progression Patterns
| Outcome | Mechanism |
|---|---|
| Healing | Fibrosis, calcification - "Ranke complex" |
| Reactivation TB | Latent bacilli resume growth, usually upper lobes (higher O₂) |
| Miliary TB | Hematogenous dissemination → millet-seed lesions in lungs, liver, spleen, meninges |
| Cavitation | Liquefaction of caseous material → bronchial communication → highly infectious |
| Primary progressive TB | Failure to contain in immunocompromised host |
Extrapulmonary TB
| Site | Manifestation |
|---|---|
| Lymph nodes (most common extrapulmonary) | Scrofula - painless cervical lymphadenopathy with matted nodes |
| Pleura | Pleuritis with exudative pleural effusion (lymphocyte-predominant) |
| Spine (Pott disease) | Vertebral body destruction, paravertebral "cold abscess", kyphosis |
| Meninges | TB meningitis - lymphocytic CSF, low glucose, high protein |
| Pericardium | Constrictive pericarditis |
| Genitourinary | "Sterile pyuria" - WBCs with negative routine culture |
| Adrenal | Addison disease |
| Peritoneum | Ascites, omental thickening |
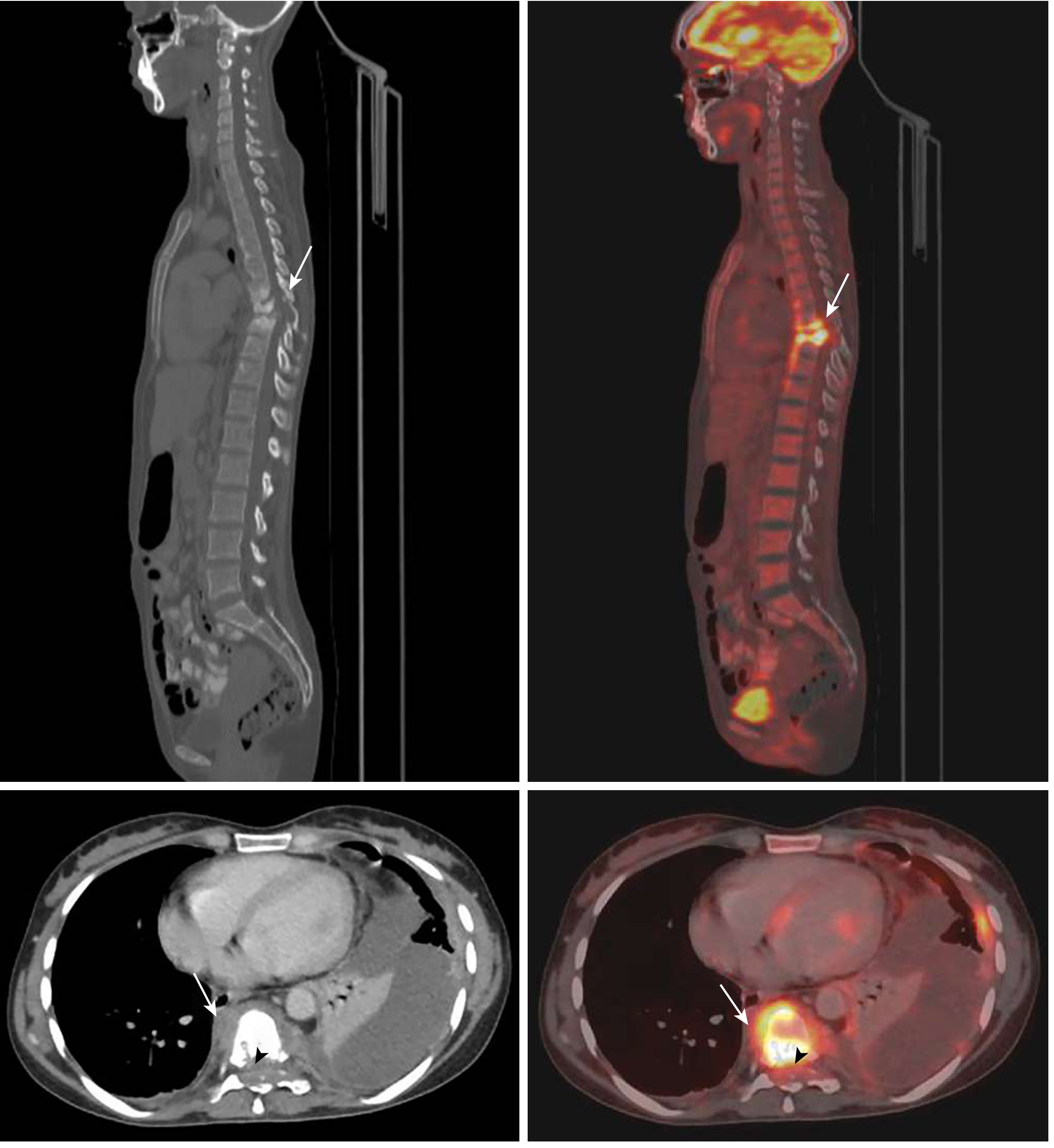
Fig: Pott disease (spinal TB) - CT and FDG-PET showing T7-T10 vertebral destruction, collapse of T8, and left paravertebral cold abscess. (Goldman-Cecil Medicine)
Latency / Dormancy / Reactivation
Latent TB infection likely represents a spectrum from complete bacterial elimination to subclinical active infection. Only 5-10% of LTBI progresses to active TB.
Risk factors for reactivation:
- HIV (strongest - 8-10% annual risk)
- TNF blockade (biologics like infliximab, adalimumab) - clear immunologic mechanism
- Diabetes mellitus
- Malnutrition, smoking, alcohol
- Age extremes, malignancy, CKD, silicosis
M. tuberculosis itself can drive reactivation via resuscitation-promoting factors (Rpfs) that act on peptidoglycan to promote growth during recovery from dormancy. Dormant bacteria may reside in adipose tissue, lymphatic endothelium, and mesenchymal stem cells. - Murray & Nadel's Respiratory Medicine, p. 1180
3. CLINICAL FEATURES
Primary TB
Usually asymptomatic or mild flu-like illness. Positive tuberculin skin test (TST) conversion after 3-8 weeks.
Active Pulmonary TB (Reactivation)
Classic "FAWN" symptoms:
- Fever (low-grade, afternoon)
- Anorexia/weight loss ("consumption")
- Wasting
- Night sweats
Respiratory: Chronic productive cough, hemoptysis (from cavitation), dyspnea. Upper lobe cavitary infiltrates on CXR are classic.
TB Meningitis
Subacute onset headache, fever, neck stiffness; CSF: lymphocytic pleocytosis, low glucose (<45 mg/dL), elevated protein, high ADA. High mortality; steroids reduce mortality. A 2026 Lancet Infectious Diseases practice guideline for TB meningitis (PMID 40840485) provides updated management recommendations.
Immunologic Manifestations
- Erythema nodosum and erythema induratum - tuberculids (hypersensitivity reactions)
- Poncet disease - reactive arthritis + erythema nodosum
- TB-IRIS (immune reconstitution inflammatory syndrome) - occurs in 5-50% of HIV patients starting ART, paradoxical worsening with fever and lymphadenitis
4. DIAGNOSIS
Tests for Latent TB Infection (LTBI)
1. Tuberculin Skin Test (TST / Mantoux)
- Intradermal injection of 5 TU PPD
- Read at 48-72 hours
- Induration (not erythema) measured:
- ≥5 mm: HIV+, immunosuppressed, close contacts, abnormal CXR
- ≥10 mm: Healthcare workers, immigrants, IV drug users, prisons
- ≥15 mm: Low-risk individuals
- False positives: BCG vaccination, NTM infection
- False negatives: Anergy (HIV, malnutrition, sarcoidosis, very severe TB)
2. Interferon-Gamma Release Assays (IGRAs)
- QuantiFERON-TB Gold, T-SPOT.TB
- Measure IFN-γ release by T cells stimulated with ESAT-6 and CFP-10 (antigens absent from BCG and most NTM)
- More specific than TST; not affected by BCG; single visit
- Preferred in BCG-vaccinated individuals - Goldman-Cecil Medicine, p. 3256
Tests for Active TB Disease
| Test | Details |
|---|---|
| Sputum smear (ZN) | Rapid, cheap; sensitivity ~50-60%; positive if ≥5000 bacilli/mL |
| Sputum culture | Gold standard; LJ medium (3-8 weeks); MGIT liquid (1-3 weeks) |
| GeneXpert MTB/RIF | Detects MTB DNA + rifampicin resistance in ~2 hours; sensitivity ~88%, specificity ~99% |
| Chest X-ray | Upper lobe cavitation (reactivation), hilar adenopathy (primary), miliary pattern |
| CT chest | Better than CXR; tree-in-bud nodularity, cavitation, consolidation |
| Bronchoscopy + BAL | For smear-negative/sputum-scarce patients |
| ADA (adenosine deaminase) | Elevated in pleural fluid, CSF, peritoneal fluid in TB |
5. PHARMACOLOGY - ANTITUBERCULOSIS DRUGS
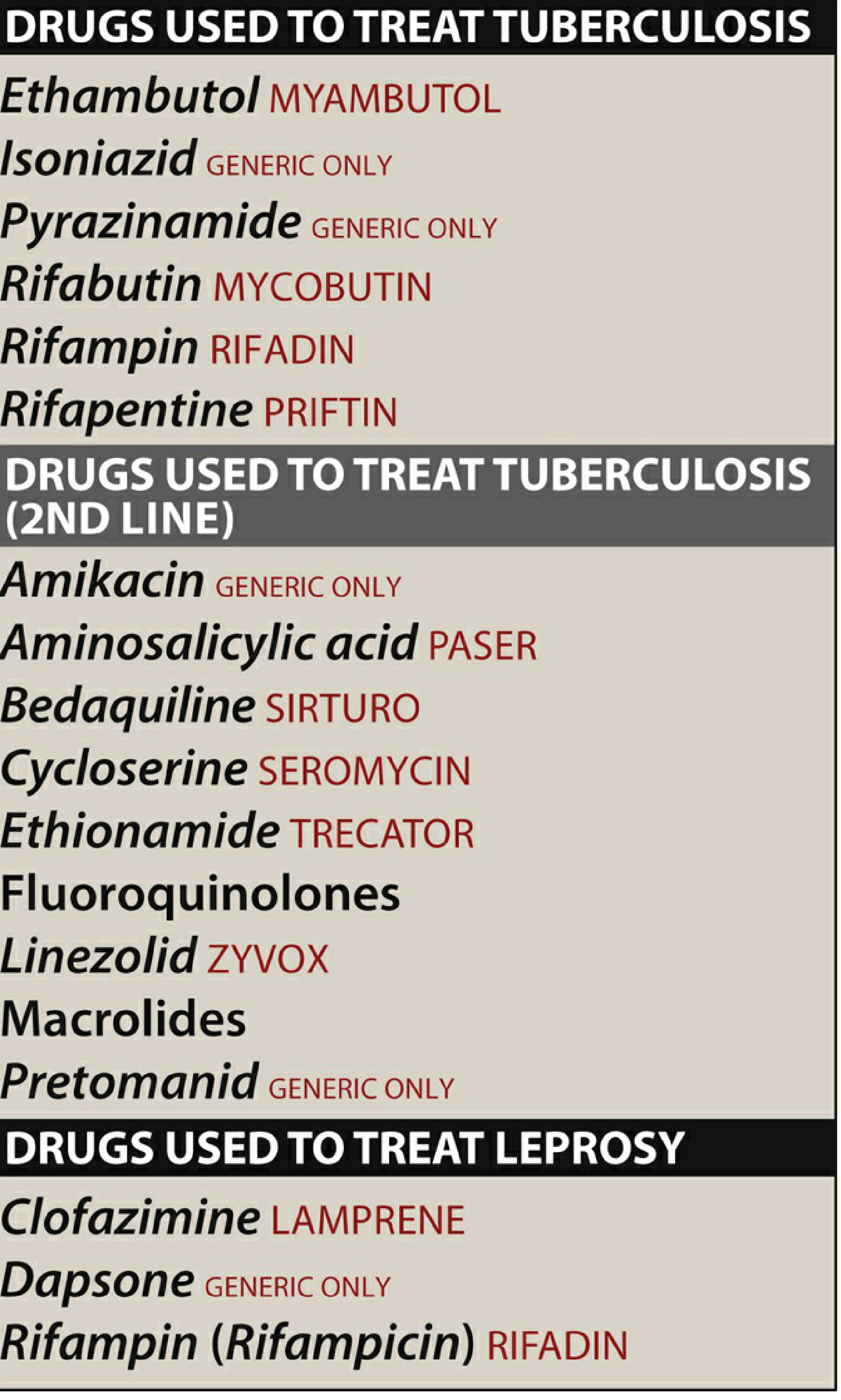
First-line TB drugs: Ethambutol, Isoniazid, Pyrazinamide, Rifampin/Rifabutin/Rifapentine. Second-line: Amikacin, Aminosalicylic acid, Bedaquiline, Cycloserine, Ethionamide, Fluoroquinolones, Linezolid, Pretomanid. (Lippincott Pharmacology)
First-Line Drugs (RIPE / HRZE)
1. Isoniazid (H / INH)
Mechanism: Prodrug activated by mycobacterial catalase-peroxidase KatG → inhibits InhA (acyl carrier protein reductase) and KasA (β-ketoacyl-ACP synthase) → blocks mycolic acid synthesis → disrupts cell wall.
Activity: Bactericidal for actively dividing organisms (intracellular and extracellular); bacteriostatic against slowly dividing organisms. Specific for M. tuberculosis (M. kansasii may be susceptible at higher concentrations).
Pharmacokinetics:
- Well absorbed orally; impaired by food (especially high-fat meals)
- Distributes to all body fluids, cells, caseous material; CSF = serum levels (excellent CNS penetration)
- Metabolized by N-acetyltransferase 2 (NAT2) - genetically polymorphic:
- Fast acetylators: half-life ~90 min
- Slow acetylators: half-life ~3-4 hours (bimodal distribution)
- Excreted renally (mainly as metabolites)
Adverse effects:
- Hepatotoxicity - most serious; fatal if unrecognized; risk increases with age >35, alcohol use, co-administration with rifampin
- Peripheral neuropathy - due to pyridoxine (Vitamin B6) deficiency via competitive inhibition of B6-dependent enzymes; prevented by pyridoxine 25-50 mg/day supplementation
- Drug-induced lupus (slow acetylators)
- CNS effects (seizures, psychosis) - rare
Resistance: Mutations in KatG (prevents prodrug activation) or overexpression/mutation of InhA. Cross-resistance with ethionamide possible. - Lippincott Pharmacology, p. 1055
2. Rifampin (R) / Rifampicin
Mechanism: Binds to the β-subunit of mycobacterial DNA-dependent RNA polymerase → blocks RNA transcription → bactericidal.
Activity: Bactericidal for both intracellular and extracellular mycobacteria; active against M. tuberculosis, M. kansasii, and other NTM; also active against M. leprae, Staphylococcus, H. influenzae, Neisseria.
Pharmacokinetics:
- Well absorbed orally; food impairs absorption
- Hepatic metabolism; bile excretion (enterohepatic circulation)
- Potent CYP450 inducer (CYP3A4, 2C9, 2C19) - major drug interactions
- CSF penetration adequate (especially with inflammation)
- Turns urine, sweat, tears orange-red (harmless but important to counsel patients)
Adverse effects:
- Hepatotoxicity (especially with isoniazid)
- Drug interactions (CYP inducer): reduces levels of oral contraceptives, warfarin, protease inhibitors, methadone, azoles
- Flu-like syndrome (intermittent dosing)
- Thrombocytopenia, hemolytic anemia (rare)
- Rifabutin: less CYP induction - preferred with HIV antiretrovirals
- Rifapentine: long half-life; used for once-weekly LTBI regimens
Resistance: Mutations in the rpoB gene (encodes RNA polymerase β-subunit). Rifampicin resistance is a surrogate for MDR-TB detection by GeneXpert. - Lippincott Pharmacology, p. 5592
3. Pyrazinamide (Z / PZA)
Mechanism: Prodrug converted by pyrazinamidase (PncA) in mycobacteria → pyrazinoic acid → disrupts membrane potential; inhibits fatty acid synthase I; active in acidic pH (within macrophage phagolysosomes). Active primarily against M. tuberculosis only. Allows treatment shortening from 9 to 6 months. - Harrison's Internal Medicine 22e, p. 391
Activity: Bactericidal against intracellular, slowly dividing bacteria in acidic environments (macrophages, necrotic tissue). Critical for sterilizing effect in short-course therapy.
Pharmacokinetics: Well absorbed; good CNS penetration; hepatic metabolism; renal excretion
Adverse effects:
- Hepatotoxicity - most serious; dose-dependent; monitor LFTs
- Hyperuricemia - inhibits tubular secretion of urate → gout (treat with allopurinol or probenecid; withhold if symptomatic gout)
- Arthralgias
- Photosensitivity, rash
Resistance: Mutations in pncA gene
4. Ethambutol (E / EMB)
Mechanism: Inhibits arabinosyl transferases (EmbB) → blocks arabinogalactan synthesis (a key cell wall polysaccharide) → impairs mycobacterial cell wall integrity. Bacteriostatic.
Activity: Active against M. tuberculosis, M. avium, and some other mycobacteria.
Adverse effects:
- Retrobulbar optic neuritis - most important; dose-dependent; presents as decreased visual acuity, red-green color blindness; usually reversible on stopping the drug. Baseline and monthly visual testing required.
- Hyperuricemia
Use: Primarily to prevent emergence of resistance to the other three drugs; dropped once susceptibility confirmed.
Standard Treatment Regimens
Drug-Susceptible TB:
| Phase | Duration | Drugs | Mnemonic |
|---|---|---|---|
| Intensive phase | 2 months | HRZE (Isoniazid + Rifampin + Pyrazinamide + Ethambutol) | "2 HRZE" |
| Continuation phase | 4 months | HR (Isoniazid + Rifampin) | "4 HR" |
| Total | 6 months |
Extensions: Cavitary disease + positive culture at 2 months → extend to 9 months. CNS TB → 12 months.
LTBI Treatment Options:
- 3HP: Weekly isoniazid + rifapentine × 12 doses (3 months) - preferred
- 4R: Daily rifampin × 4 months
- 3HR: Daily isoniazid + rifampin × 3 months
- 6H/9H: Daily isoniazid × 6 or 9 months (traditional)
Second-Line Drugs
| Drug | Class | Key Mechanism / Use |
|---|---|---|
| Fluoroquinolones (levofloxacin, moxifloxacin) | Group A | Inhibit DNA gyrase; bactericidal; backbone of MDR regimens |
| Bedaquiline | Diarylquinoline | Inhibits mycobacterial ATP synthase (subunit c); novel; bactericidal |
| Pretomanid | Nitroimidazole | Inhibits mycolic acid synthesis + generates reactive nitrogen species; activates in anaerobic conditions |
| Linezolid | Oxazolidinone | Inhibits 50S ribosome (23S rRNA); bactericidal; bone marrow suppression |
| Clofazimine | Riminophenazine | Disrupts membrane; anti-inflammatory; repurposed from leprosy |
| Cycloserine | Analog of D-alanine | Inhibits cell wall synthesis (D-Ala-D-Ala ligase); CNS toxicity |
| Ethionamide | Thioamide | Inhibits InhA (same target as INH); hepatotoxic; cross-resistance with INH |
| Amikacin/Kanamycin | Aminoglycosides | Inhibit 30S ribosome; injectable; nephrotoxic, ototoxic |
| Para-aminosalicylic acid (PAS) | - | Inhibits folate synthesis in mycobacteria; GI intolerant |
Drug-Resistant TB (DR-TB)
Definitions:
- MDR-TB: Resistant to both isoniazid AND rifampin
- Pre-XDR-TB (WHO 2021): MDR-TB + resistant to any fluoroquinolone
- XDR-TB: MDR-TB + fluoroquinolone resistance + at least one Group A drug (bedaquiline or linezolid)
WHO 2022 preferred regimen for MDR-TB - BPaLM:
Bedaquiline + Pretomanid + Linezolid + Moxifloxacin (BPaLM) × 6 months
- TB PRACTECAL trial showed BPaLM noninferior to 9-20 month standard care, with fewer serious adverse events
- Previous Nix-TB trial showed BPaL (without moxifloxacin) achieved favorable outcomes in 89% of highly drug-resistant cases - Harrison's Internal Medicine 22e, p. 322-323
⚠️ Recent Evidence Note: A 2026 Lancet Infectious Diseases guideline on TB meningitis (PMID 40840485) updates management recommendations for CNS TB. A 2024 meta-analysis on TB-diabetes comorbidity (PMID 38346381) highlights the treatment challenges in this growing comorbid population.
6. SPECIAL SITUATIONS
HIV-TB Coinfection
- Start ART within 2 weeks of TB treatment (unless TB meningitis - delay to 8 weeks to reduce IRIS risk)
- Use rifabutin instead of rifampin (less CYP induction with protease inhibitors)
- Watch for TB-IRIS: paradoxical worsening in 5-50% starting ART; treat with corticosteroids
- Steroids (dexamethasone) recommended for all TB meningitis to reduce mortality
TB in Pregnancy
- Treat with HRZE (ethambutol avoided in some guidelines; pyrazinamide safety debated but WHO recommends its use)
- Streptomycin contraindicated (ototoxicity to fetus)
- Pyridoxine supplementation essential
Drug Monitoring
| Drug | Monitor |
|---|---|
| Isoniazid | LFTs (baseline + if symptomatic), peripheral neuropathy symptoms |
| Rifampin | LFTs, drug interactions review |
| Pyrazinamide | LFTs, uric acid, joint symptoms |
| Ethambutol | Visual acuity + red-green color discrimination (monthly) |
| Bedaquiline | QTc interval (ECG) |
7. PREVENTION
- BCG vaccine: Live attenuated M. bovis; given at birth in TB-endemic countries; protects against miliary TB and TB meningitis in children (~80%); less effective against adult pulmonary TB; standard intradermal dose
- BCG revaccination: Recent trial showed ~45% efficacy in preventing sustained LTBI in adolescents
- M72/AS01E vaccine: Adjuvanted protein subunit vaccine; Phase 2b trial showed ~50% efficacy in IGRA-positive adults against active TB disease - Murray & Nadel's Respiratory Medicine, p. 1181
- Infection control: Negative-pressure isolation rooms, N95 respirators, UV germicidal irradiation
- Contact tracing and treatment of LTBI in close contacts
Quick Reference Summary
TB DRUG MNEMONICS
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
First-line: RIPE / HRZE
H = Isoniazid → Mycolic acid (KatG prodrug → InhA/KasA)
R = Rifampin → RNA polymerase (rpoB)
Z = Pyrazinamide → Membrane potential / FAS-I (acidic env)
E = Ethambutol → Arabinogalactan (EmbB)
Toxicities (Classic Board Targets):
INH → Peripheral neuropathy (give B6!), hepatitis
RIF → Orange urine, CYP inducer, hepatitis
PZA → Hyperuricemia, hepatitis
EMB → Optic neuritis (red-green color blindness)
MDR-TB preferred: BPaLM × 6 months (WHO 2022)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Sources: Robbins & Kumar Basic Pathology, Murray & Nadel's Textbook of Respiratory Medicine (2-vol), Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22e, Lippincott Illustrated Reviews: Pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.