diagnosis and management of drug induced hepatitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"drug-induced liver injury" diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Drug-Induced Liver Injury (DILI) / Drug-Induced Hepatitis
Drug-induced liver injury (DILI) is the most common cause of acute liver failure in the Western world. It accounts for approximately 10% of cases of severe acute hepatitis at tertiary centers. Despite this importance, it remains a diagnosis of exclusion, as no single test can definitively confirm it in most cases.
1. Classification and Mechanisms
Three mechanistic categories are recognized (Goldman-Cecil Medicine, p. 1587):
A. Direct / Intrinsic Hepatotoxicity
- Caused by the parent drug or, more commonly, a toxic reactive metabolite
- Dose-dependent - virtually every user will develop toxicity at a high enough dose
- Short latency (hours to days)
- Prototype: Acetaminophen (paracetamol)
B. Idiosyncratic Hepatotoxicity
Two subtypes exist (Harrison's, Table 351-1):
| Feature | Immunoallergic Reaction | Metabolic Idiosyncrasy |
|---|---|---|
| Frequency | <1 per 10,000 exposed | 1-50 per 10,000 exposed |
| Gender | Women predominate (often ≥2:1) | Variable |
| Latency | Fairly constant, 2-10 weeks | More variable, 2-24 weeks, occasionally >1 year |
| Dose relationship | None | Usually none |
| Mechanism | Immune/allergic | Drug metabolism anomaly |
| Recurrence on rechallenge | Prompt | Variable |
| Examples | Nitrofurantoin, halothane | Isoniazid, valproate |
Idiosyncratic DILI generally reflects an adaptive immune (cytotoxic T-cell) attack on the liver, triggered when drug-related neoantigen-protein adducts are presented on hepatocyte surfaces. HLA haplotypes and cytokine polymorphisms determine individual susceptibility.
C. Indirect Toxicity (Goldman-Cecil, p. 1587)
- Liver injury is a side effect of the drug's intended actions
- Examples: immunosuppressants that reactivate viral hepatitis (HBV, HCV); immune checkpoint inhibitors (pembrolizumab, nivolumab) that trigger T-cell-mediated hepatitis
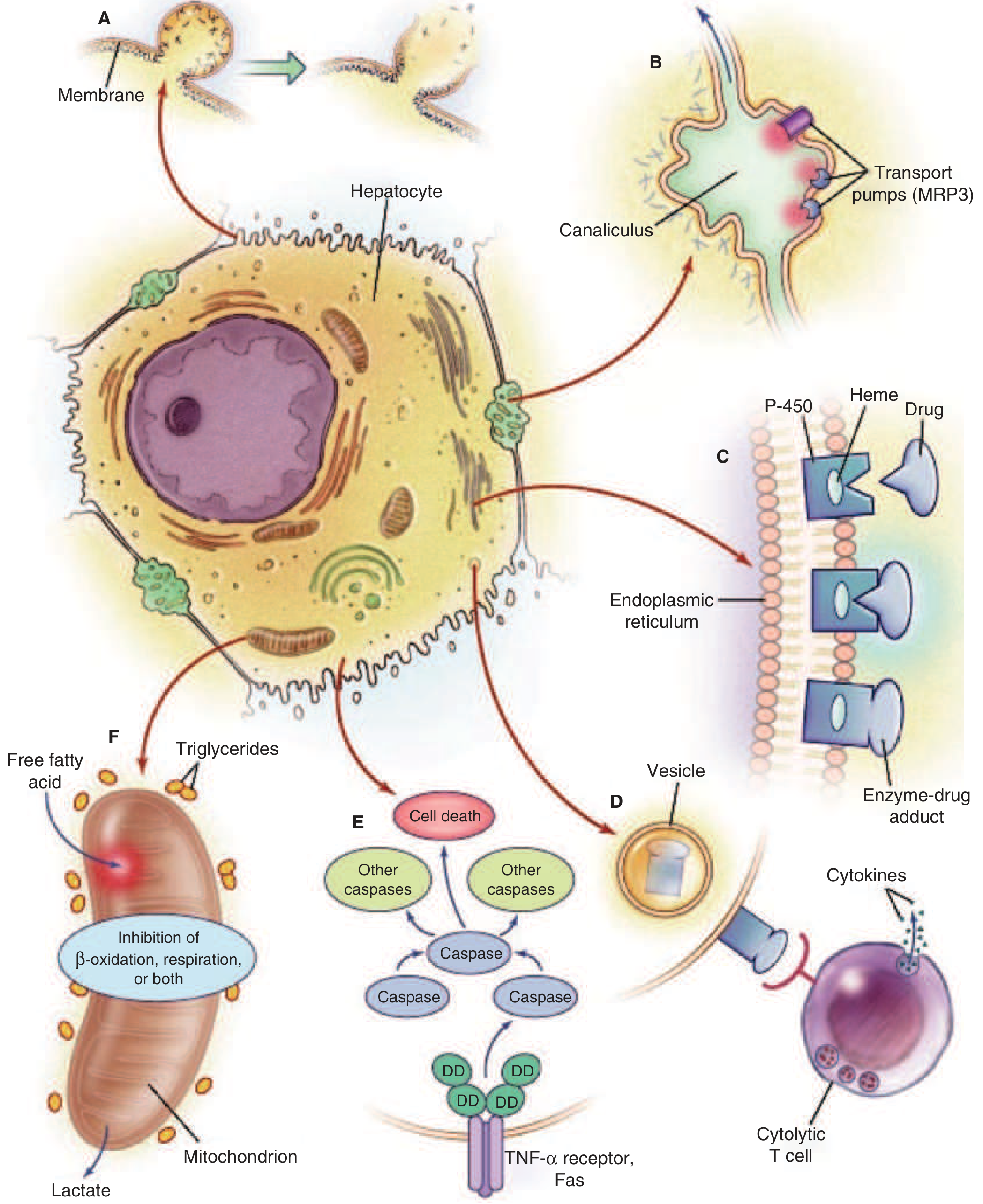
2. Pathophysiology
Key mechanisms (Harrison's Fig. 351-1):
| Mechanism | Effect |
|---|---|
| Disruption of intracellular calcium homeostasis | Actin fibril disassembly → cell membrane rupture |
| Disruption of bile canalicular transport pumps (MRP3) | Bile acid accumulation → secondary hepatocyte injury, cholestasis |
| Cytochrome P450 - drug covalent binding (adducts) | Nonfunctioning enzyme, neoantigen formation |
| Immune attack via CTLs / cytokines | Cytolytic T-lymphocyte destruction of hepatocytes |
| TNF-α / Fas activation | Apoptotic cascade via caspases |
| Mitochondrial inhibition | Impaired β-oxidation + respiratory chain → lactic acidosis, microvesicular steatosis |
Most drug hepatotoxicity results from a phase I toxic metabolite (e.g., NAPQI from acetaminophen via CYP2E1). Phase II reactions (glucuronidation, sulfation) and glutathione conjugation are normally protective. Glutathione depletion (fasting, malnutrition, alcoholism) significantly lowers the toxicity threshold.
3. Clinical Presentations
Hepatocellular Pattern
- Resembles acute viral hepatitis: jaundice, nausea, RUQ pain, malaise
- Elevated ALT/AST (can exceed 10,000 IU/L in acetaminophen toxicity)
- Acetaminophen: characteristic very high aminotransferases with disproportionately low bilirubin - a biochemical signature of hyperacute injury
Cholestatic Pattern
- Pruritus, jaundice, elevated alkaline phosphatase
- Examples: estrogens, anabolic steroids, amoxicillin-clavulanate, chlorpromazine
Mixed Pattern
- Combination of both
Pattern Classification - The R-Value (Goldman-Cecil, p. 1588):
- R = (ALT ÷ ULN) ÷ (ALP ÷ ULN)
- R ≥ 5: hepatocellular
- R ≤ 2: cholestatic
- 2 < R < 5: mixed
Granulomatous Hepatitis
Distinct subtype - caused by: allopurinol, diltiazem, hydralazine, quinidine, sulfonamides, phenytoin (Sleisenger & Fordtran, p. 1674)
Chronic Hepatitis
Some drugs cause a chronic hepatitis picture (>3-6 months) resembling autoimmune hepatitis: nitrofurantoin, methyldopa, minocycline, diclofenac
Acute Liver Failure (ALF)
- Most severe outcome - encephalopathy + coagulopathy
- DILI is the most common identifiable cause of ALF in Western countries
4. Diagnosis
International Consensus Criteria (Goldman-Cecil, Table 136-1)
DILI is defined by any one of the following peak serum values (assuming previously healthy liver):
- ALT ≥ 5× ULN
- ALP ≥ 2× ULN (in absence of bone pathology)
- ALT ≥ 3× ULN AND total bilirubin ≥ 2× ULN (in absence of hemolysis/Gilbert's)
Hy's Law
A powerful predictor of severe outcome. A drug causing hepatocellular injury (ALT > 3× ULN) plus jaundice (bilirubin > 2× ULN) plus no other cause found = ~10% mortality risk from ALF. This combination is used in drug development as a regulatory safety signal.
Causality Assessment
Because there is no confirmatory biomarker, causality is assessed by:
- Detailed medication history: all prescription drugs, OTC medications, herbal/dietary supplements (including duration, dose, and timeline)
- Temporal relationship: onset of liver abnormalities after drug exposure and resolution after stopping (dechallenge)
- Rechallenge (generally avoided for safety): recurrence of injury confirms causality
- Exclusion of alternative diagnoses: viral hepatitis A/B/C/E, autoimmune hepatitis, ischemic hepatitis, biliary obstruction, Wilson disease
- RUCAM (Roussel Uclaf Causality Assessment Method): the most widely used structured scoring tool
Features Supporting Diagnosis
- Fever, rash, eosinophilia (suggest immunoallergic mechanism)
- Known association between the implicated drug and hepatotoxicity
- Time from exposure to onset fitting known patterns for that drug
- Improvement in liver tests within weeks of drug cessation (for hepatocellular DILI; cholestatic DILI may normalize more slowly)
Key Investigations
- LFTs (ALT, AST, ALP, GGT, bilirubin, albumin, PT/INR)
- Full blood count (eosinophilia)
- Viral serology: HBsAg, anti-HBc, anti-HAV IgM, anti-HCV, anti-HEV IgM
- Autoimmune markers: ANA, ASMA, LKM-1, IgG
- Abdominal ultrasound (exclude biliary obstruction, chronic liver disease)
- Liver biopsy: not routinely required but useful when diagnosis is uncertain, when autoimmune hepatitis cannot be excluded, or when DILI severity/histology will guide management
5. Important Causative Drugs
| Category | Examples |
|---|---|
| Analgesics | Acetaminophen, NSAIDs (diclofenac, sulindac) |
| Antibiotics | Isoniazid, rifampicin, amoxicillin-clavulanate, nitrofurantoin, flucloxacillin, tetracyclines |
| Antifungals | Ketoconazole, fluconazole |
| Anticonvulsants | Valproate, phenytoin, carbamazepine |
| Cardiovascular | Amiodarone, hydralazine, methyldopa, statins |
| Immunosuppressants | Methotrexate, azathioprine |
| Psychiatric | Chlorpromazine, haloperidol |
| Hormones | Anabolic steroids, oral contraceptives (cholestasis) |
| Herbal supplements | Kava, pyrrolizidine alkaloids (Comfrey), Green tea extract |
| Anti-TB drugs | Isoniazid, pyrazinamide, rifampicin |
| Checkpoint inhibitors | Nivolumab, pembrolizumab (indirect, immune-mediated) |
6. Management
A. Acetaminophen Hepatotoxicity (Direct Toxin)
- N-acetylcysteine (NAC) is the specific antidote - effective if given within 12 hours of ingestion, but still used even after injury has evolved
- NAC replenishes glutathione stores and prevents further NAPQI-mediated hepatocyte damage
- Activated charcoal if presentation within 1-2 hours of ingestion
- Serum acetaminophen levels: levels >300 μg/L at 4 hours post-ingestion predict severe damage; levels <150 μg/L suggest injury is highly unlikely
- Monitor PT/INR, creatinine, glucose, acid-base status
- Contact liver transplant center early if ALF develops
B. Idiosyncratic DILI - General Principles
- Stop the offending drug immediately - this is the cornerstone of management
- Supportive care: adequate nutrition, avoidance of further hepatotoxins, alcohol abstinence
- Monitor LFTs until normalization (may take weeks to months for cholestatic DILI)
- Do not rechallenge in most cases - risk of more severe recurrence
C. Specific Situations
Corticosteroids:
- May be considered for immunoallergic DILI (especially if features of autoimmune hepatitis overlap), but evidence is limited and they are not routinely recommended
- Often used for checkpoint inhibitor-mediated hepatitis (Grade 2-4)
Checkpoint inhibitor hepatitis:
- Grade 1 (ALT <3× ULN): continue immunotherapy with monitoring
- Grade 2 (ALT 3-5× ULN): hold immunotherapy, consider corticosteroids (prednisolone 0.5-1 mg/kg/day)
- Grade 3-4 (ALT >5× ULN): permanently discontinue; high-dose IV methylprednisolone 1-2 mg/kg/day; add mycophenolate mofetil if refractory
Isoniazid hepatitis:
- If clinical hepatitis develops (symptomatic or ALT >3× ULN), stop all anti-TB drugs
- Re-introduce one at a time after recovery, with monitoring
Valproate hepatotoxicity:
- Idiosyncratic, most severe in children under 2 years on polypharmacy
- Stop valproate; carnitine supplementation may be beneficial
D. Acute Liver Failure
- Transfer to a liver transplant center
- King's College Criteria or MELD score guide transplant listing
- Liver transplantation remains the definitive treatment for irreversible ALF from DILI
7. Prognosis
- Most cases resolve within weeks to months after drug withdrawal
- Hy's Law cases carry ~10% mortality without liver transplantation
- Cholestatic DILI generally has a better prognosis than hepatocellular DILI, but can persist for months ("prolonged cholestasis" or "vanishing bile duct syndrome" with some drugs, e.g., chlorpromazine, amoxicillin-clavulanate)
- Progression to chronic liver disease or cirrhosis is uncommon but possible
Recent Evidence (PubMed 2024-2026)
- A 2024 Chinese practice guideline (PMID 40198161) for primary care settings and a 2024 anti-TB drug DILI guideline (PMID 39497389) have been published, reflecting ongoing standardization of diagnostic criteria and management protocols.
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025), Ch. 351
- Goldman-Cecil Medicine, Ch. 136
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 88
- Morgan & Mikhail's Clinical Anesthesiology, 7th ed.
Nutrition and weightlifting advice in this case
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
nutrition advice recovery drug-induced hepatitis liver injury diet exercise
Finding Sources
Finding Sources
Reading Web Page
https://easl.eu/wp-content/uploads/2019/04/EASL-CPG-Drug-ind…
Finding Sources
Finding Sources
Searching PubMed
"drug-induced liver injury" AND "dietary supplement" AND bodybuilding
Reading File
Finding Sources
I now have enough material to compose a thorough, well-organized answer. Let me compile it.
Nutrition and Weightlifting in Drug-Induced Hepatitis
This covers two angles: what to eat and how to exercise during recovery, and what supplements/drugs to avoid to prevent DILI in the first place for someone who lifts weights.
PART 1: Recovery - Nutrition During DILI
General Principles
The injured liver has reduced capacity for protein synthesis, glycogen storage, fat metabolism, and detoxification. Nutritional support accelerates hepatocyte regeneration and prevents further damage.
Energy Intake
- Avoid fasting - even short fasting worsens DILI by depleting hepatic glutathione, which is the liver's primary antioxidant defense against toxic drug metabolites (particularly critical for acetaminophen hepatotoxicity)
- Target 25-35 kcal/kg/day for most patients (higher end if malnourished or with significant liver injury)
- Small, frequent meals (5-6 per day) help maintain blood glucose and reduce hepatic metabolic load
- Eat a protein-containing snack before bed to reduce overnight fasting; limit overnight fast to under 7 hours
Protein
- Do not restrict protein in acute DILI (unlike historically recommended for encephalopathy) unless overt hepatic encephalopathy is present
- Target 1.2-1.5 g/kg/day of high-quality protein - this supports liver cell regeneration
- Good sources: eggs, poultry, fish, dairy (milk, yoghurt), legumes
- If encephalopathy develops: short-term modest protein restriction may be needed, then resume adequate intake as encephalopathy resolves; branched-chain amino acids (BCAAs) may be considered as an alternative protein source
Carbohydrates
- Adequate carbohydrate intake maintains hepatic glycogen and spares protein from being used for energy
- Prioritize complex carbohydrates: oats, rice, sweet potato, whole grains
- Avoid alcohol entirely - alcohol induces CYP2E1 and depletes glutathione, directly potentiating hepatotoxicity
Fats
- Avoid high-fat meals acutely, which increase hepatic metabolic burden
- Avoid saturated and trans fats
- Small amounts of healthy fats (olive oil, oily fish) are acceptable
- Avoid vitamin A megadosing - high-dose vitamin A is directly hepatotoxic and worsens liver disease (Harrison's)
Key Micronutrients
- N-acetylcysteine (NAC) - the most evidence-based intervention; replenishes glutathione. Used medically for acetaminophen overdose but also given to support general recovery in severe DILI
- Zinc - commonly deficient in liver disease; supports immune function and wound healing
- B vitamins (B1/thiamine, B6, B12, folate) - often depleted in liver disease
- Avoid high-dose iron supplements - iron accumulates in damaged hepatocytes and worsens oxidative injury
- Avoid copper supplements - can be hepatotoxic in excess when liver is already injured
Hydration
- Maintain good hydration to support renal clearance of drug metabolites
- Avoid anything that stresses the kidneys (NSAIDs, excess caffeine) since acetaminophen DILI can cause concurrent renal injury
What to Avoid
| Avoid | Reason |
|---|---|
| Alcohol | Induces CYP2E1, depletes glutathione, directly toxic |
| Acetaminophen / paracetamol | Primary cause of direct DILI; contraindicated |
| NSAIDs | Additional hepatotoxic risk; also nephrotoxic |
| High-dose fat-soluble vitamins (A, D) | Can be hepatotoxic in excess |
| All herbal supplements | Many are hepatotoxic (kava, green tea extract, comfrey, black cohosh) |
| Fasting / crash dieting | Depletes glutathione, worsens toxicity threshold |
| Processed/salty foods | Increases metabolic load; risk of fluid retention if cholestasis is present |
PART 2: Weightlifting and Exercise During Recovery
Acute Phase (Active Liver Injury - Elevated ALT/AST, Jaundice)
- Rest from strenuous exercise - heavy resistance training significantly raises ALT and AST from muscle breakdown, which confounds liver monitoring and increases overall metabolic burden on the liver
- The EASL DILI guidelines explicitly note that "aminotransferase elevations are often confounded by the effects of physical exercise" during recovery - making it harder to track liver healing
- Light walking is acceptable and may improve circulation and mood
- Resume weightlifting only after LFTs normalize or are trending strongly downward, typically confirmed by your physician
Recovery Phase (Improving LFTs, Asymptomatic)
- Gradually reintroduce activity: walking → light aerobic exercise → bodyweight training → progressive resistance training
- Diet and exercise together have been shown to reverse liver inflammation and reduce fibrosis (University of Missouri study, 2023)
- Avoid training to exhaustion - this generates reactive oxygen species that further challenge a recovering liver
Chronic/Stable Phase (LFTs Normal)
- Full return to training is appropriate
- Regular moderate-to-vigorous exercise is actually hepatoprotective - improves insulin sensitivity, reduces hepatic fat, and reduces inflammatory cytokines
- Resistance training specifically reduces visceral fat and improves liver enzyme profiles
PART 3: Prevention - Supplements and Substances Weightlifters Must Avoid
This is the most important section for gym-goers, as dietary and herbal supplements now account for ~20% of all DILI cases in the US (DILIN data), and this proportion is rising sharply.
High-Risk Supplements Commonly Used by Weightlifters
| Supplement | Risk | Notes |
|---|---|---|
| Anabolic androgenic steroids (AAS) | Very high | Most dangerous - causes cholestatic hepatitis, peliosis hepatis, hepatic adenoma, rarely HCC. Illicit use increasing markedly (EASL 2019) |
| OxyELITE Pro | Very high | Contains dimethylamylamine (DMAA) + aegeline - multiple cases of ALF, recalls by FDA |
| Hydroxycut | High | Contains green tea extract, ephedra, caffeine - linked to hepatocellular hepatitis and ALF |
| Green tea extract (EGCG) | Moderate-high | Concentrated extract (not brewed tea) is hepatotoxic in high doses |
| Usnic acid (LipoKinetix, UCP-1) | High | Associated with acute hepatocellular hepatitis and ALF (PMID 38904414) |
| Kava-kava | High | Well-documented hepatotoxicity |
| Ephedra (Ma Huang) | High | Banned by FDA; causes ALF |
| Creatine | Low | Considered safe at recommended doses; mild transient AST/ALT rise possible |
| Whey protein | Generally safe | High doses may stress liver in those with pre-existing disease; choose products with NSF or Informed Sport certification |
| Pre-workouts with stimulant blends | Variable, often moderate-high | Often contain undisclosed or novel stimulants; avoid during and after DILI |
| SARMs (Selective Androgen Receptor Modulators) | High | Increasingly used illicitly for muscle-building; multiple case reports of severe cholestatic hepatitis and ALF |
Safe Supplementation After Recovery
Once LFTs are fully normalized and the offending agent is identified and stopped:
- Protein supplements (plain whey, casein, pea protein): Generally safe; choose third-party certified products (NSF Certified for Sport, Informed Sport)
- Creatine monohydrate: Well-established safety profile; acceptable
- Vitamin D (moderate dose, not megadose): Often deficient; appropriate supplementation is safe
- Omega-3 fatty acids: Anti-inflammatory; no hepatotoxicity at standard doses
- Magnesium, zinc: Safe at standard doses; support muscle recovery
- Avoid ALL proprietary "fat burner," "pre-workout," or "test booster" blends - these frequently contain undisclosed hepatotoxic compounds or are contaminated (PMID 38826497 - 2024 case series on cholestasis from contaminated bodybuilding supplements)
Label Reading Rules for Athletes
- Products with long lists of proprietary blends = higher risk
- "Natural" or "herbal" does not mean safe for the liver
- Any product with a disclaimer like "not for individuals with liver disease" is a red flag
- Always check LiverTox - the NIH's free database of hepatotoxic drugs and supplements
Summary Table: Return to Training Timeline
| Phase | Liver Status | Exercise | Nutrition Focus |
|---|---|---|---|
| Acute DILI | ALT/AST actively elevated, symptomatic | Rest; light walking only | Small frequent meals, adequate protein, no fasting, no alcohol |
| Subacute | ALT/AST falling, improving | Light aerobic activity | Maintain protein 1.2-1.5 g/kg, antioxidant-rich diet |
| Recovery | ALT/AST near normal | Bodyweight → light resistance | Full balanced diet, no supplement use |
| Full recovery | LFTs normal | Full training | Normal sports nutrition; avoid all hepatotoxic supplements permanently |
Bottom line: The most important step is identifying and permanently stopping the offending agent. For weightlifters, anabolic steroids, SARMs, and proprietary supplement blends are now leading causes of serious DILI. Nutrition during recovery centers on adequate protein, avoidance of fasting and alcohol, and no herbal supplements. Return to heavy training should wait until LFTs normalize to avoid confounding liver monitoring.
What about UDCA for treatment
Finding Sources
Searching PubMed
"ursodeoxycholic acid" AND "drug-induced liver injury"
Reading Article
PMID: 36672522
Finding Sources
Finding Sources
Finding Sources
Searching the Web
UDCA ursodeoxycholic acid drug-induced liver injury cholestatic DILI evidence guidelines 2023 2024
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11797819
I now have detailed, current evidence. Here is a thorough answer.
UDCA (Ursodeoxycholic Acid) for Drug-Induced Hepatitis
The Core Position: Empirical Use, Weak Evidence
UDCA occupies a nuanced space in DILI management. It is not a first-line standard-of-care drug, but it is widely used empirically, particularly for cholestatic DILI, and the evidence base is growing - though still far from robust.
The key problem, as Teschke (2022, PMID 36672522) notes: no well-designed RCT has specifically evaluated UDCA in DILI. Most supporting evidence comes from case series, individual case reports, and retrospective analyses - all without control groups. This means it is impossible to separate the effect of UDCA from spontaneous recovery after drug withdrawal alone.
What the Major Guidelines Say
| Guideline | Statement on UDCA |
|---|---|
| EASL 2019 | "Chronic cholestasis following DILI is often treated with UDCA. However, the effects of UDCA in DILI are not well documented and contradicting results have been reported." Grade D (inconclusive evidence) |
| AASLD 2023 | "Ursodeoxycholic acid may improve symptoms of pruritus and hasten DILI recovery" - cautiously supportive for symptomatic use |
| APASL 2021 | "Case reports and series suggested UDCA may improve cholestatic liver injuries associated with certain antimicrobials and steroid-resistant immune checkpoint inhibitors combined with corticosteroids" |
| Chinese TB-DILI Guideline 2024 | Includes UDCA as part of the management algorithm for anti-TB drug cholestatic DILI |
The bottom line across all guidelines: stopping the offending drug remains the primary intervention; UDCA is considered a reasonable add-on particularly in cholestatic DILI, but its use is discretionary.
Mechanisms - Why UDCA Could Help
UDCA's properties extend well beyond simple "bile acid replacement." Relevant mechanisms include (Journal of Clinical and Translational Hepatology, 2025; Seminars in Liver Disease, 2024):
| Mechanism | Relevance to DILI |
|---|---|
| Anticholestatic | Replaces toxic hydrophobic bile acids; reduces bile acid-mediated hepatocyte injury; stimulates bile flow (choleresis) |
| Anti-apoptotic | Inhibits mitochondria-mediated apoptosis; stabilizes mitochondrial membrane potential |
| Antioxidant | Reduces reactive oxygen species (ROS) generated by CYP450 drug metabolism |
| Anti-inflammatory | Downregulates inflammatory cytokines (TNF-α, IL-1β) that amplify hepatocyte damage |
| Anti-necrotic | Reduces necrotic hepatocyte death pathways |
| BSEP protection | Counteracts pharmacological inhibition of bile salt export pump (BSEP) - a key mechanism of cholestatic DILI from drugs like flucloxacillin, amoxicillin-clavulanate |
| Transporter upregulation | Modulates expression of hepatic, renal, and intestinal transporters to improve clearance of hepatotoxic compounds |
| ER stress relief | Reduces endoplasmic reticulum stress triggered by drug metabolites |
These multi-pathway effects explain why UDCA may offer benefit even in hepatocellular DILI, not just cholestatic - an observation confirmed in the 2025 systematic review (PMC11797819).
Clinical Evidence - What the Case Series Show
A MEDLINE review (1995-2025) retrieved 41 clinical studies suggesting benefit. Key observations:
- Improvements seen in both cholestatic/mixed and hepatocellular DILI patterns (no statistically significant difference between groups)
- Most commonly benefited drugs: amoxicillin-clavulanate, flucloxacillin, bosentan, anabolic steroids
- Clinical and laboratory improvement typically occurred within 7-12 weeks of UDCA treatment initiation
- UDCA doses used ranged from 15 to 45 mg/kg/day; no clear dose-response relationship observed
- Maximum reported dose: 1,500 mg/day with no adverse effects
- Beneficial responses also reported in immune checkpoint inhibitor hepatitis refractory to steroids (used as add-on to corticosteroids)
- Preventive role: some evidence UDCA reduces the incidence of DILI when co-prescribed with known hepatotoxic drugs (e.g., methotrexate, anti-TB regimens)
Practical Use - When to Consider UDCA
Strongest indication:
- Cholestatic or mixed DILI - particularly with jaundice, pruritus, and elevated ALP/GGT
- Prolonged cholestasis / vanishing bile duct syndrome - where bile duct injury may persist despite drug withdrawal (associated with drugs like chlorpromazine, amoxicillin-clavulanate)
- Anabolic steroid-induced cholestasis - one of the better-documented scenarios
Reasonable consideration:
- Cholestatic DILI from anti-TB drugs (UDCA included in Chinese 2024 TB-DILI guidelines)
- Checkpoint inhibitor hepatitis not responding to steroids alone (combined with corticosteroids)
- Symptom control of pruritus in cholestatic DILI (AASLD 2023)
For symptom relief specifically:
- Pruritus from cholestasis: UDCA 300 mg twice daily is a reasonable first step before adding cholestyramine or rifampicin
Dose
- Standard range in DILI case reports: 10-15 mg/kg/day in 2-3 divided doses (similar to PBC dosing)
- Some cases used up to 45 mg/kg/day without toxicity, though the optimal dose for DILI is not established
- Duration: typically continued until LFTs normalize or plateau, often 2-4 months
Safety
UDCA has an excellent safety profile - it is one of the safest drugs used in hepatology. Side effects are uncommon and include:
- Loose stools / mild diarrhea (usually dose-dependent)
- Rarely: pruritus worsening at very high doses in complete biliary obstruction (contraindication)
Contraindication: Complete biliary obstruction (mechanical) - UDCA is ineffective and potentially harmful here. Always exclude biliary obstruction with ultrasound before starting.
Summary
| Question | Answer |
|---|---|
| Is UDCA recommended by all guidelines? | No - evidence grade is D (EASL); AASLD is cautiously supportive |
| Is it used in practice? | Yes - widely, especially for cholestatic DILI |
| Does it work? | Probably yes for symptom relief and LFT improvement, but RCT proof is absent |
| Best indication | Cholestatic/mixed DILI, prolonged cholestasis, pruritus |
| Dose | ~10-15 mg/kg/day in divided doses |
| Safe? | Yes - very well tolerated |
| Replace drug withdrawal? | No - stopping the offending drug always comes first |
The most honest summary comes from Teschke (2022): "some patients with cholestatic DILI may benefit from UDCA" - empirical use is reasonable given its safety, the lack of alternatives, and plausible multi-mechanism hepatoprotection, while we await proper RCTs.
Sources:
- Teschke R. Treatment of Drug-Induced Liver Injury. Biomedicines 2022 (PMID 36672522)
- Bessone F et al. UDCA for Drug-Induced Liver Disease. Seminars in Liver Disease 2024
- EASL DILI Clinical Practice Guidelines 2019
- AASLD Practice Guidance on DILI 2023
- PMC11797819 - UDCA mechanisms and clinical evidence 2025
UDCA use and mechanism of action
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have everything needed for a complete, well-sourced answer.
Ursodeoxycholic Acid (UDCA / Ursodiol) - Uses and Mechanism of Action
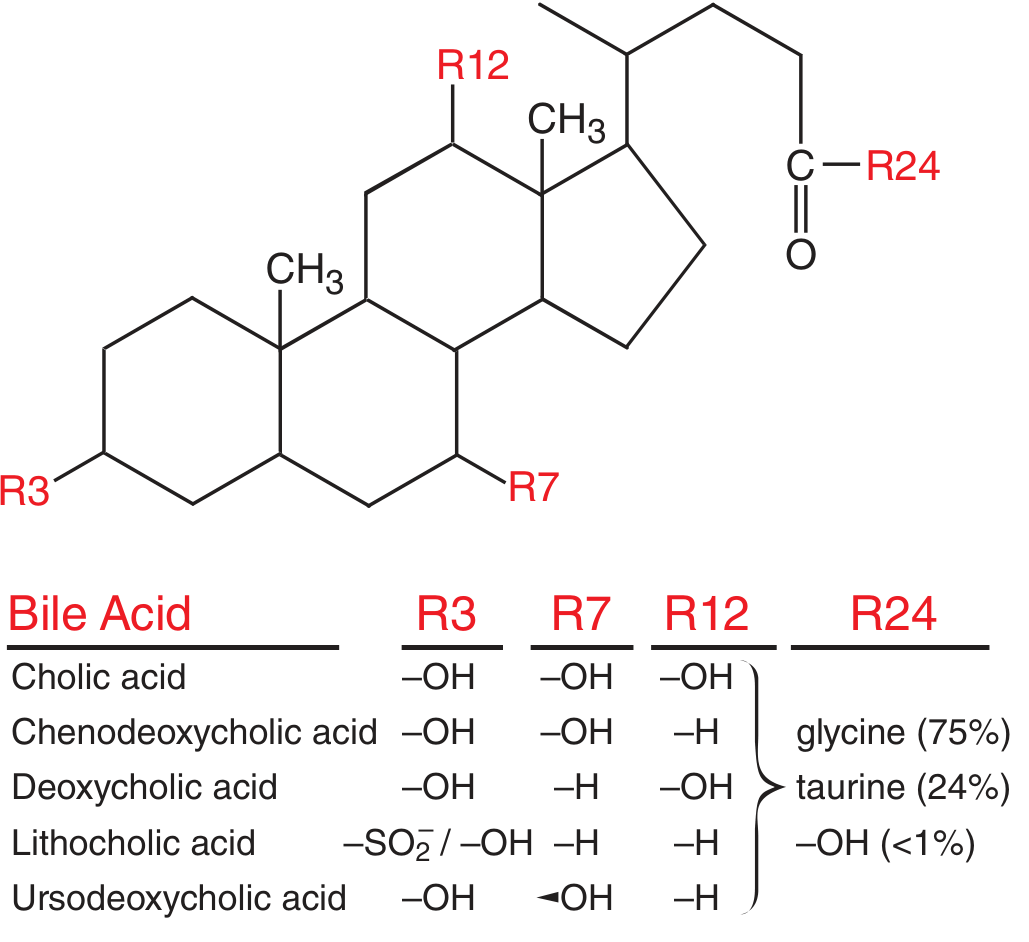
1. Chemistry and Origin
UDCA is a naturally occurring, hydrophilic bile acid - it constitutes only a minor fraction (<5%) of the normal human bile acid pool. It is formed by epimerization of chenodeoxycholic acid (CDCA) in the gut by intestinal bacteria. The key structural difference from other bile acids: at position R7, UDCA has a beta-oriented hydroxyl group (pointing upward), whereas CDCA has an alpha-oriented hydroxyl. This seemingly small change makes UDCA hydrophilic and non-toxic, compared with the hydrophobic, membrane-damaging bile acids like CDCA, deoxycholic acid (DCA), and lithocholic acid.
2. Mechanisms of Action
UDCA acts through multiple complementary pathways, which explains its utility across a broad range of liver conditions.
A. Replacement of Toxic Hydrophobic Bile Acids
The primary mechanism. In cholestatic liver disease, hydrophobic bile acids (CDCA, DCA, lithocholic acid) accumulate and cause direct membrane damage to hepatocytes and cholangiocytes. When UDCA is given in therapeutic doses, it becomes the dominant biliary bile acid (up to 40-60% of the bile acid pool), physically displacing and diluting the toxic hydrophobic species. This reduces bile acid-mediated membrane disruption. (Goodman & Gilman's, p. 1124)
B. Choleretic / Bile Flow Stimulation
UDCA stimulates bile secretion (choleresis) by:
- Upregulating expression of bile acid transporters, particularly BSEP (bile salt export pump) and MRP2 on the canalicular membrane
- Stimulating vesicular exocytosis at the canalicular level
- Increasing bicarbonate-rich cholangiocyte secretion ("bicarbonate umbrella"), which protects the bile duct epithelium from protonated toxic bile acids
C. Cytoprotection of Hepatocytes
UDCA directly protects hepatocytes from bile acid-induced apoptosis and necrosis:
- Anti-apoptotic: stabilizes the mitochondrial membrane, preventing cytochrome c release and caspase activation; inhibits the Fas/FasL apoptotic pathway
- Anti-necrotic: reduces toxic bile acid-induced membrane disruption and calcium overload
- Mitochondrial protection: preserves mitochondrial membrane potential and β-oxidation capacity
D. Immunomodulation
Particularly relevant in autoimmune liver diseases:
- Reduces aberrant MHC class I and II expression on hepatocytes and cholangiocytes (which drives immune-mediated destruction)
- Reduces circulating IgM and IgG levels in PBC
- Modulates T-lymphocyte and NK cell activity
- Downregulates pro-inflammatory cytokines (Robbins Basic Pathology, p. 2251)
E. Reduction of Cholesterol Saturation / Litholytic Action
For gallstone disease specifically:
- Decreases biliary cholesterol secretion by suppressing hepatic HMG-CoA reductase and cholesterol 7α-hydroxylase
- Reduces cholesterol absorption from the gut
- Makes bile less lithogenic (less saturated with cholesterol)
- Directly dissolves cholesterol crystals in gallstones over time
F. Antioxidant Effects
- Scavenges reactive oxygen species (ROS) generated during drug metabolism (CYP450 reactions)
- Reduces oxidative stress in hepatocytes subjected to toxic metabolites
G. Endoplasmic Reticulum (ER) Stress Relief
- Attenuates ER stress triggered by accumulation of toxic metabolites and misfolded proteins in hepatocytes
3. Pharmacokinetics (ADME)
- Absorption: well absorbed orally via passive and active transport in the small intestine; undergoes extensive first-pass extraction by the liver
- Distribution: becomes a major biliary and plasma bile acid after repeated dosing; enters enterohepatic circulation
- Metabolism: conjugated with glycine and taurine in the liver before biliary secretion; largely reabsorbed in the terminal ileum (>95% enterohepatic recycling)
- Elimination: primarily fecal excretion
- Taking UDCA with food improves absorption and enterohepatic cycling
4. Clinical Uses and Doses
| Indication | Dose | Evidence/Status |
|---|---|---|
| Primary biliary cholangitis (PBC) | 13-15 mg/kg/day in 2-4 divided doses | First-line, standard of care; improves LFTs, delays progression, reduces transplant need - Grade A |
| Gallstone dissolution | 8-10 mg/kg/day in divided doses | Effective for small (<10 mm), radiolucent, cholesterol-rich stones in functioning gallbladder; treatment takes 6-24 months |
| Gallstone prevention | 300 mg twice daily | Reduces gallstone formation in rapid weight loss (e.g., post-bariatric surgery) |
| Intrahepatic cholestasis of pregnancy (ICP) | 13-15 mg/kg/day or 1 g/day | Relieves maternal pruritus and improves liver biochemistry; considered first-line |
| Primary sclerosing cholangitis (PSC) | 15 mg/kg/day | Modest symptomatic benefit only; does NOT slow disease progression or improve survival - not routinely recommended by EASL/AASLD. High dose (>25 mg/kg/day) is potentially harmful |
| Cholestatic DILI | 10-45 mg/kg/day (empirical) | Improves symptoms and LFTs; evidence from case series only - no RCTs (see previous discussion) |
| Non-alcoholic fatty liver disease (NAFLD) | Various | Not recommended - trials show improved LFTs but no histological or clinical outcome benefit |
| Cystic fibrosis-related liver disease | 20 mg/kg/day | Used in children/adults with CF-associated cholestasis; improves LFTs |
| Total parenteral nutrition (TPN)-associated cholestasis | Variable | Evidence limited; used empirically in selected cases |
5. Second-Line Options When UDCA Fails
For PBC with inadequate response to UDCA (defined as persistent elevated ALP >1.67× ULN or bilirubin >ULN after 1 year):
- Obeticholic acid (OCA) - a potent farnesoid X receptor (FXR) agonist; approved as second-line add-on or monotherapy in UDCA-intolerant patients. Mechanism: suppresses hepatic bile acid synthesis via FXR → reduced bile acid pool size; increases canalicular bile acid excretion. Dose: 5-10 mg once daily. Important: black box warning for hepatic decompensation in incorrectly dosed cirrhotic patients (dose must be reduced to 5 mg weekly in Child-Pugh B/C). Most common side effect: pruritus (Goodman & Gilman's, p. 1124)
- Fibrates (bezafibrate, fenofibrate) - PPARα agonists with anti-cholestatic effects; now recommended as second-line by some guidelines
- Budesonide - for PBC with overlap autoimmune features (non-cirrhotic only)
For PSC: liver transplantation remains the only effective treatment.
6. Adverse Effects
UDCA is exceptionally well-tolerated at standard doses. Adverse effects are uncommon:
- Loose stools / mild diarrhea (most common, usually transient, dose-dependent)
- Nausea, headache, abdominal discomfort
- At high doses (>25-28 mg/kg/day in PSC): paradoxically worsens outcomes in PSC (increased risk of varices, transplantation, death in one RCT) - this is an important warning
Contraindications:
- Complete biliary obstruction (mechanical)
- Acute cholangitis
- Calcified, pigment, or radio-opaque gallstones (UDCA cannot dissolve these)
- Allergy to bile acids
7. Summary: Where UDCA Stands
| Disease | UDCA Role |
|---|---|
| PBC | Indispensable first-line; best evidence |
| ICP | First-line for symptoms |
| Gallstones | Effective; now largely replaced by laparoscopic cholecystectomy |
| Cholestatic DILI | Reasonable empirical use; symptom relief |
| PSC | Symptomatic use only; no disease-modifying effect |
| NAFLD/viral hepatitis/alcoholic liver disease | Not recommended |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 54
- Goldman-Cecil Medicine, Ch. 110 (PSC)
- Robbins & Kumar Basic Pathology
- Teschke R. Treatment of DILI. Biomedicines 2022 (PMID 36672522)
- EASL DILI Clinical Practice Guidelines 2019
This is a shared conversation. Sign in to Orris to start your own chat.