Low Anterior Resection (LAR) procedure in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
low anterior resection LAR procedure surgical technique steps
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the detailed response.
Low Anterior Resection (LAR) - Detailed Overview
Definition and Context
Low anterior resection (LAR) is defined as resection of the rectum with an extraperitoneal rectal anastomosis. The primary indication is rectal cancer, though it is also performed for diverticular disease, inflammatory bowel disease, large polyps, GI bleeding, and rectal prolapse. The defining principle is complete extirpation of the tumor and involved lymphatics, with re-establishment of bowel continuity as a secondary goal.
The anatomical goal that underpins LAR for cancer is Total Mesorectal Excision (TME), introduced by Heald and Ryall in the 1980s - complete removal of the mesorectal envelope surrounding the rectum in its visceral fascial layer, which dramatically reduces local recurrence rates compared to blunt dissection.
Fascial Anatomy - The Foundation of Safe Dissection
Understanding the fascial planes is the key to performing LAR correctly:
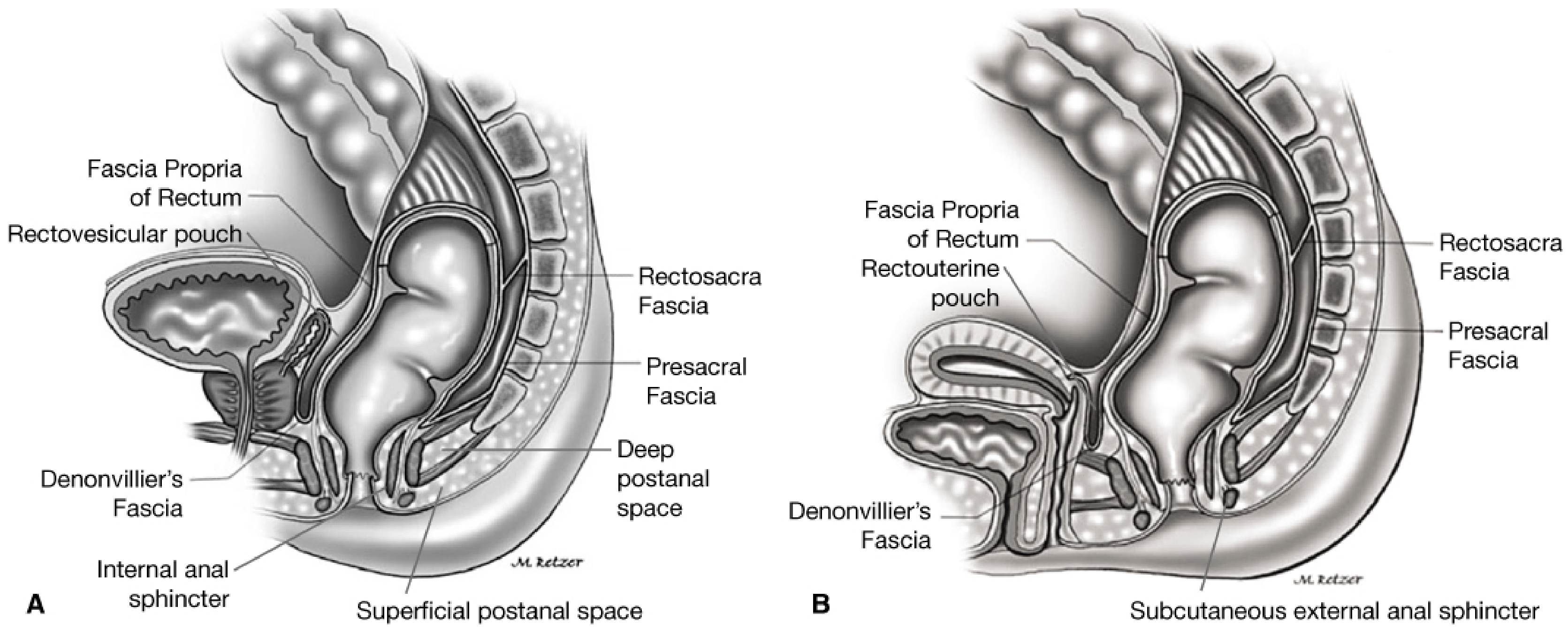
- Fascia propria of the rectum - thin visceral fascia enveloping the rectum and mesorectum; the correct dissection plane is outside this layer
- Denonvilliers' fascia - bilaminar layer anterior to the rectum, separating it from the prostate/seminal vesicles (male) or vagina (female); included with the specimen in cancer surgery
- Presacral (Waldeyer's) fascia - covers the anterior sacrum; dissection deep to this risks catastrophic bleeding from the presacral venous plexus
- Rectosacral fascia - connects presacral fascia at ~S4 to the posterior-inferior rectum; divided close to the presacral fascia during TME
- Lateral stalks - fibrous condensations connecting the rectum to the pelvic sidewall; the middle rectal artery traverses them in ~25% of cases
Pre-operative Evaluation
- Endorectal ultrasound (ERUS) or MRI for staging and defining the circumferential resection margin (CRM)
- Distance from the anorectal ring determines feasibility of LAR vs. abdominoperineal resection (APR)
- Patients with levator or external sphincter involvement are not candidates for sphincter-preserving LAR
- Assessment of fecal continence, comorbidities, and prior radiation
- If patient is at high risk for anastomotic leak, pre-operative marking of a potential stoma site by a Wound, Ostomy, Continence nurse (WOCN)
- For distal tumors: a clear resection margin of ≥2 cm distal bowel is the standard goal; <1 cm may be acceptable for low rectal tumors after chemoradiotherapy (CRT)
- Neoadjuvant CRT (typically 5-FU based + 50.4 Gy radiation) is standard for stage II-III rectal cancers
Surgical Technique (Laparoscopic LAR - Standard Approach)
(Maingot's Abdominal Operations, 37th Ed.)
Step 1 - Patient Positioning and Room Setup
- Modified lithotomy (Lloyd-Davies) position, thighs roughly level with the abdominal wall to avoid interference with lower quadrant instruments
- Surgeon stands on the right side, assistant on the right, scrub nurse on the left
- Camera initially placed left of the patient's hips; moves cephalad as dissection progresses
- Steep Trendelenburg with left side up for left colon and rectal mobilization
Step 2 - Port Placement and Exploration
- 30-degree laparoscope via supraumbilical port
- Three 5-mm trocars: suprapubic, right lower lateral quadrant, left lower lateral quadrant - all lateral to epigastric vessels
- Abdominal exploration to confirm pathology and rule out peritoneal disease
Step 3 - Mobilization of the Left Colon
- Patient in steep Trendelenburg, left side up
- Peritoneum lateral to sigmoid colon is retracted medially, the left peritoneal reflection opened along the white line of Toldt using cautery or scissors
- Left ureter identified at the base of the sigmoidal fossa on the medial aspect - maintaining correct retroperitoneal plane exposes Gerota's fascia
- Splenic flexure mobilization performed if needed for a tension-free anastomosis
Step 4 - Vascular Pedicle Ligation (High Tie)
- Right and perirectal peritoneum scored cephalad to expose the origin of the superior hemorrhoidal and sigmoidal vessels
- Windows developed on either side of the vascular pedicle; both ureters confirmed out of the field
- For cancer: high ligation of the inferior mesenteric artery (IMA) at the aortic bifurcation (or just below the left colic take-off for upper rectal tumors)
- Divided using vascular stapler, Harmonic scalpel, or LigaSure
Step 5 - Mobilization of the Rectum (TME)
This is the oncologically critical step:
- Care to never penetrate the mesorectal fascia (fascia propria)
- Posterior plane: Table tilted right-side up, sigmoid retracted anteriorly and to the right. The presacral space is developed with sharp dissection to the pelvic floor. The hypogastric nerves are identified and gently swept toward the sacrum
- Left lateral plane: Left lateral dissection continued along the lateral aspect of the rectum, meeting the presacral plane
- Anterior plane: Dissection taken above the peritoneal reflection; in cancer, the Denonvilliers' fascia is included with the specimen (anterior plane kept close to posterior vaginal wall / seminal vesicles)
- The lateral stalks are divided to allow deep pelvic exposure for mid-to-low rectal tumors
- Dissection carried to the levator ani level
- Flexible sigmoidoscopy confirms the optimal level of transection
Step 6 - Excision of the Rectum
- Mesorectum divided with LigaSure or Harmonic scalpel, perpendicular to the bowel wall (to avoid a "coning" effect that compromises distal mesorectal clearance)
- Rectum transected with a laparoscopic articulating linear stapler introduced through a small suprapubic incision or hand-port
- Specimen extracted through the supraumbilical incision
- Distal margin: at least 2 cm distal bowel clearance; at least 4 cm distal mesorectal clearance below the tumor
Step 7 - Anastomosis (Colorectal / Coloanal)
Standard colorectal anastomosis (double-staple technique):
- A purse-string suture is placed in the proximal colon resection margin, and the circular stapler anvil is tied in place
- Proximal colon returned to the abdomen; incision closed; pneumoperitoneum re-established
- Circular stapler (25-29 mm) inserted transanally; trocar advanced across (or just in front of) the rectal staple line under laparoscopic visualization
- Anvil coupled to the shaft; device fired, creating an end-to-end anastomosis
- Leak test: pelvis filled with saline, rectum insufflated with air via flexible scope, proximal colon occluded with alligator clamp - air bubbles indicate a leak requiring suture reinforcement or diversion
For ultra-low / coloanal anastomosis:
- Extended LAR is used for distal rectal lesions several cm above the sphincter
- Anterior dissection extended to the rectovaginal septum in women, distal to seminal vesicles/prostate in men
- Options: colonic J-pouch (preferred for first 1-2 years function), side-to-end anastomosis (anvil 3-4 cm from stapled end), or straight coloanal anastomosis
- J-pouch and side-to-end anastomosis significantly improve postoperative bowel function for the first 1-2 years without increasing anastomotic complications (supported by multiple RCTs)
Step 8 - Defunctioning Stoma (Selective)
A diverting loop ileostomy (DLI) significantly reduces clinical anastomotic leak rates and reoperation rates (prospective studies). Indications for DLI:
- Low rectal anastomosis (<5 cm from sphincters)
- Neoadjuvant radiotherapy
- Male sex (independent risk factor for leak)
- Technically difficult or tension on anastomosis
- Evidence of leak on intraoperative testing
- Immunosuppression, poor nutritional status
Approaches
| Approach | Notes |
|---|---|
| Laparoscopic LAR | Standard of care; 4-5 ports; steep learning curve (~150 cases for laTME) |
| Hand-assisted laparoscopic | 6-8 cm hand-port incision; useful for bulky tumors |
| Robotic LAR | Shorter learning curve (~25 cases); better visualization in deep male pelvis; ROLARR trial (2017) showed no significant difference vs. laparoscopic in conversion rate or margins; Chinese multicenter RCT (2023, n=1240) showed lower positive margin rate (4% vs. 7.2%) and lower complications with robotic approach |
| Open LAR | Reserved for advanced/bulky disease or failed minimally invasive approach |
| Transanal TME (taTME) | Emerging technique; bottom-up approach from transanal route; improves access in narrow pelvis |
Complications
Intraoperative
- Ureteral injury - from failure to identify/protect ureters during vascular ligation or rectal mobilization
- Presacral venous bleeding - life-threatening; occurs when dissection goes deep to presacral fascia; torn vessels retract into sacral foramina making control extremely difficult
- Hypogastric nerve injury - sexual and bladder dysfunction
- Splenic injury during flexure mobilization
Early Postoperative
| Complication | Notes |
|---|---|
| Anastomotic leak | Most feared; higher risk with low anastomosis, male sex, neoadjuvant radiation, diabetes, obesity. Minor leaks: antibiotics + percutaneous drain. Major leaks: return to OR, proximal diversion (loop ileostomy) or Hartmann's (end colostomy + rectal stump). CT with minimal rectal contrast for diagnosis |
| Pelvic sepsis | Often secondary to anastomotic leak |
| Bleeding | From anastomosis, staple lines, presacral vessels |
| Ileus / bowel obstruction | Port site hernias more common laparoscopically |
| DVT/PE | Prolonged lithotomy position + pelvic surgery = high risk; sequential compression devices + LMWH |
Late Complications
- Anastomotic stricture - managed by serial dilatation
- Stoma reversal complications (if DLI created)
Low Anterior Resection Syndrome (LARS)
LARS is a well-recognized constellation of bowel dysfunction following LAR, experienced by 25-50% of patients (Fischer's Mastery of Surgery):
Symptoms:
- Increased stool frequency and fragmentation
- Fecal urgency and clustering
- Fecal incontinence
- Incomplete evacuation
- Gas incontinence
Risk factors: Female sex, neoadjuvant radiotherapy, TME (vs. partial mesorectal excision), low tumors, anastomotic leak, handsewn anastomosis
Pathophysiology: Loss of rectal reservoir, disruption of the rectoanal inhibitory reflex (RAIR), autonomic denervation, impaired neo-rectal compliance, sphincter/pelvic floor trauma
Scoring: The validated LARS score is the internationally accepted assessment tool.
Treatment algorithm:
- Loperamide (first-line antidiarrheal)
- Rectal irrigation (transanal irrigation to aid emptying)
- Biofeedback / pelvic floor physiotherapy - effective for mild-moderate LARS
- Sacral nerve stimulation (SNS/Interstim) - 71% success rate at 15 months follow-up (systematic review of 7 studies)
- End colostomy - for intractable, progressive fecal incontinence
Genitourinary Dysfunction
Disturbances to bladder and sexual function are common sequelae. With careful autonomic nerve preservation, rates can be reduced from 25-75% down to 10-28% (Fischer's Mastery of Surgery):
- Male: Erectile dysfunction, absent/retrograde ejaculation (hypogastric plexus at L5/S1, pelvic parasympathetics at S2-S4)
- Female: Dyspareunia, reduced orgasm
- Bladder: Difficulty emptying, incontinence (injury to inferior hypogastric plexus)
Oncologic Outcomes
- Standard LAR with TME achieves local recurrence rates of <10% compared to >25% with blunt dissection
- Quality of the TME specimen (complete, nearly complete, or incomplete) is a major determinant of local recurrence
- Circumferential resection margin (CRM): positive CRM (≤1 mm) is associated with significantly worse local recurrence and overall survival
- Neoadjuvant CRT downstages T3/T4 tumors, increases R0 resection rates, and reduces local recurrence
Key Surgical Principles Summary
- Correct fascial plane (outside fascia propria, inside presacral fascia)
- Protect autonomic nerves (hypogastric nerves posterolateral, pelvic parasympathetics lateral/anterior)
- Protect ureters throughout dissection
- Perpendicular mesorectal transection to avoid coning
- Tension-free, well-vascularized anastomosis - check with leak test
- Intraoperative colonoscopy to confirm tumor clearance and anastomotic integrity
- Selective DLI for high-risk anastomoses
Sources: Maingot's Abdominal Operations; Fischer's Mastery of Surgery, 8th ed.; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.