Teach me about ECG
Reading File
Finding Sources
Searching Images
ECG electrocardiogram waves P QRS T normal
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have a comprehensive body of textbook content to deliver a thorough ECG lesson. Let me compose this.
Electrocardiogram (ECG) — A Complete Guide
1. What Is an ECG?
An ECG (electrocardiogram) is a recording of the electrical potentials generated by the heart at the body surface. When a cardiac impulse spreads through the heart, electrical current also diffuses into adjacent tissues and all the way to the skin. Electrodes placed on opposite sides of the heart detect these potential differences and produce the characteristic waveform tracing.
— Guyton and Hall Textbook of Medical Physiology
2. The Cardiac Conduction System
Before reading an ECG, you must understand the pathway of electrical activation:
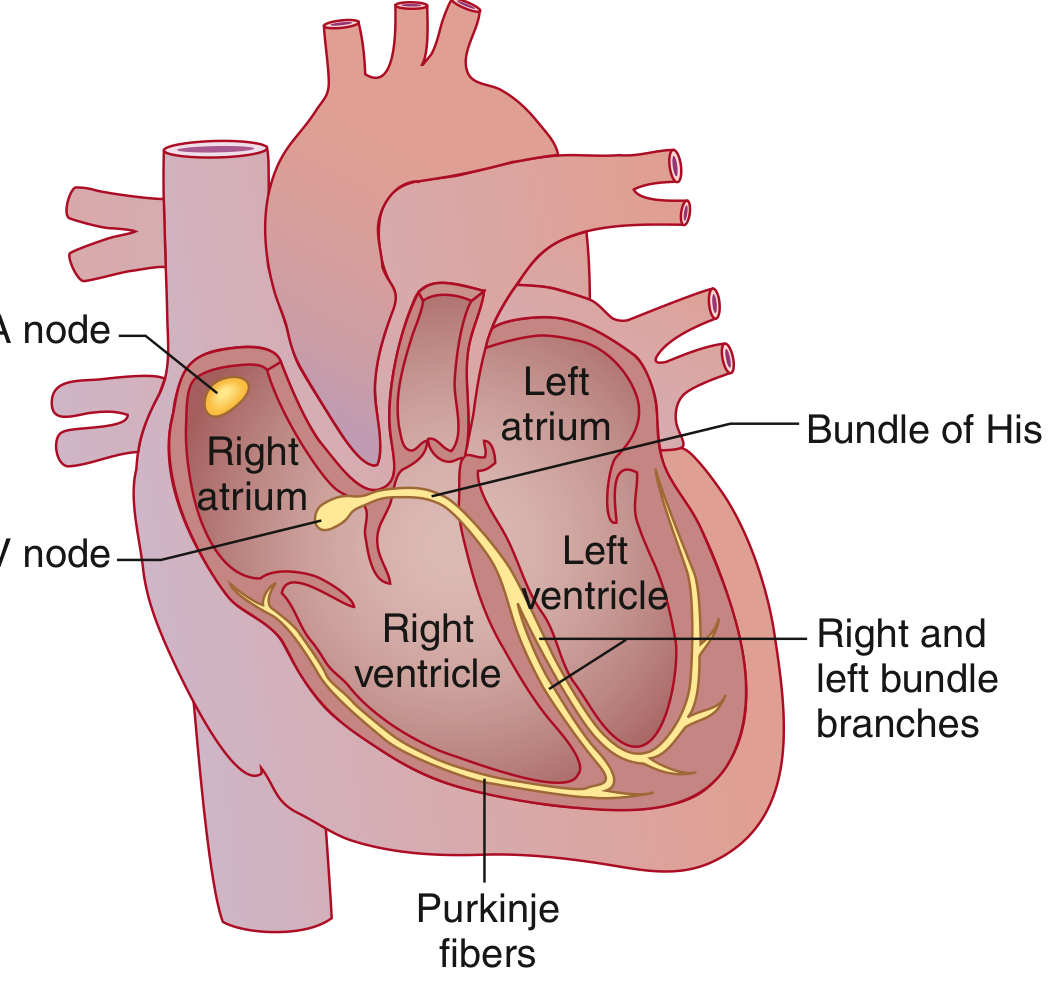
The sequence of activation is:
| Step | Structure | Function |
|---|---|---|
| 1 | SA node | Dominant pacemaker; high lateral right atrium near SVC; spontaneously depolarizes fastest |
| 2 | Atrial muscle | Wave spreads across both atria; Bachmann bundle speeds activation to left atrium |
| 3 | AV node | Only electrical link between atria and ventricles; physiologic conduction delay occurs here |
| 4 | Bundle of His | Rapid conduction; exits AV node into interventricular septum |
| 5 | Right & Left bundle branches | Left bundle further divides into anterior and posterior fascicles |
| 6 | Purkinje fibers | Fastest conduction tissue; distributes impulse to ventricular myocardium |
| 7 | Ventricular myocardium | Final activation triggers contraction |
— Goldman-Cecil Medicine, 15th Ed
3. The ECG Waveforms

P Wave
- Represents atrial depolarization
- Generated by spread of the action potential from the SA node across both atria
- Triggers atrial contraction (systole)
- Normal duration: <0.09 sec (2.5 small boxes); amplitude <3 mm
- Should be upright in leads I and II in sinus rhythm
PR Interval
- Measured from the onset of P wave to onset of QRS complex
- Normal: 0.12–0.20 sec (3–5 small boxes)
- Represents the physiologic delay at the AV node (plus conduction through atria and His-Purkinje system)
- >0.20 sec = first-degree AV block (prolonged AV nodal conduction)
- Short PR (<0.12 sec) → consider pre-excitation (Wolff-Parkinson-White) or junctional rhythm
QRS Complex
- Represents ventricular depolarization
- Composed of:
- Q wave: initial negative deflection (septal depolarization, left to right)
- R wave: first positive deflection
- S wave: negative deflection following R
- Capital letters (Q, R, S) = deflection ≥5 mm; lowercase (q, r, s) = <5 mm
- Normal duration: 0.06–0.10 sec (upper limit of normal ~0.11 sec = 3 small boxes)
- Prolonged QRS → bundle branch block or intraventricular conduction delay
- Pathological Q waves (≥0.04 sec wide, ≥25% of R height) may indicate prior MI
ST Segment
- From end of QRS (J point) to start of T wave
- Normally isoelectric (flat, on the baseline)
- ST elevation → acute myocardial injury/infarction, pericarditis, vasospasm
- ST depression → myocardial ischemia, digitalis effect, posterior MI
T Wave
- Represents ventricular repolarization
- Occurs 0.25–0.35 sec after depolarization
- Should be upright in I, II, V3–V6; inverted in aVR (normal)
- Peaked T waves → hyperkalemia
- Flattened/inverted T waves → ischemia, electrolyte disturbance, LVH
QT Interval
- From onset of QRS to end of T wave
- Reflects total ventricular depolarization + repolarization time
- Rate-corrected using Bazett's formula: QTc = QT / √RR
- Normal QTc: ≤0.44 sec (men), ≤0.46 sec (women)
- Prolonged QTc → risk of Torsades de Pointes (dangerous polymorphic VT)
U Wave
- Small deflection after T wave (not always present)
- Represents late phases of ventricular repolarization
- Prominent U waves → hypokalemia, bradycardia
— Goldman-Cecil Medicine; Guyton & Hall Physiology; Harriet Lane Handbook
4. Paper Speed & Measurements
ECG paper runs at 25 mm/sec:
| Box | Size | Time | Voltage |
|---|---|---|---|
| 1 small box | 1 mm | 0.04 sec | 0.1 mV |
| 1 large box | 5 mm | 0.20 sec | 0.5 mV |
| Standard calibration | 10 mm | — | 1 mV |
Heart rate calculation (two methods):
- Method 1: HR = 60 ÷ (R-R interval in seconds)
- Method 2 (fast): HR = 300 ÷ (number of large boxes between two R waves)
- 1 box = 300 bpm | 2 boxes = 150 | 3 = 100 | 4 = 75 | 5 = 60 | 6 = 50
5. The 12-Lead System
A standard ECG uses 12 leads — 12 different "views" of the heart's electrical activity:
Limb Leads (Frontal Plane)
| Lead | View |
|---|---|
| I | Lateral (left arm positive) |
| II | Inferior-lateral |
| III | Inferior |
| aVR | Right shoulder (cavity view) |
| aVL | High lateral |
| aVF | Inferior |
Precordial Leads (Horizontal Plane)
| Lead | Position | View |
|---|---|---|
| V1 | 4th ICS, right sternal border | Right ventricle |
| V2 | 4th ICS, left sternal border | Septum |
| V3 | Between V2 and V4 | Anterior |
| V4 | 5th ICS, mid-clavicular line | Anterior |
| V5 | Anterior axillary line | Lateral |
| V6 | Mid-axillary line | Lateral |
R-wave progression: Normally, R waves increase in amplitude from V1 → V6, with a transition (dominant R) around V3–V4. Loss of R-wave progression suggests anterior MI.
6. QRS Axis
The electrical axis tells you the dominant direction of ventricular depolarization.
| Axis | Degrees | Clinical Significance |
|---|---|---|
| Normal | −30° to +90° | Normal |
| Left axis deviation (LAD) | −30° to −90° | Left anterior fascicular block, inferior MI, LVH |
| Right axis deviation (RAD) | +90° to +180° | Right ventricular hypertrophy, left posterior fascicular block, PE |
| Extreme axis | −90° to ±180° | Ventricular rhythms |
Quick axis check: Look at leads I and aVF:
- I (+), aVF (+) → Normal axis
- I (+), aVF (−) → LAD
- I (−), aVF (+) → RAD
7. Systematic Approach to ECG Interpretation
Always read an ECG in a systematic order (from Goldman-Cecil Medicine):
- Rate — Calculate heart rate
- Rhythm — Regular vs. irregular? P waves present?
- P wave morphology — Normal sinus vs. ectopic?
- P-to-QRS relationship — 1:1 conduction? PR interval normal?
- Intervals — PR, QRS duration, QT/QTc
- QRS axis — Normal, LAD, or RAD?
- QRS morphology — Q waves? Bundle branch block? Voltage?
- ST segments — Elevation or depression? Which leads?
- T wave morphology — Upright, inverted, peaked?
- U waves — Present?
8. Normal Sinus Rhythm Criteria
A rhythm is normal sinus rhythm when:
- Rate 60–100 bpm
- Every QRS is preceded by a P wave
- P wave is upright in leads I and II (confirming SA nodal origin)
- Regular R-R intervals (minor variation = sinus arrhythmia — normal)
- PR interval 0.12–0.20 sec
- QRS ≤0.10 sec
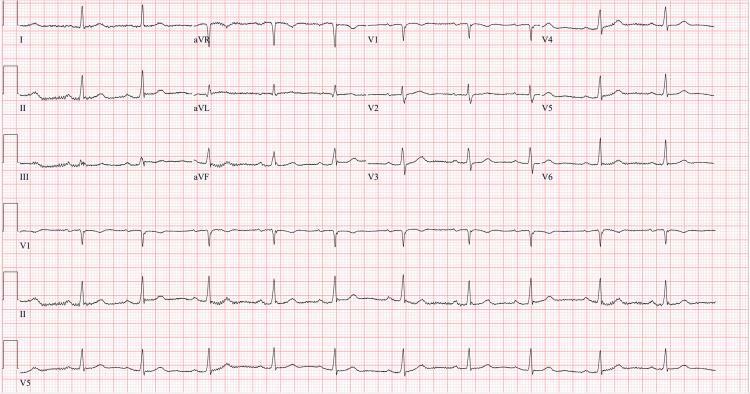
9. Example ECG
Here is an example of a normal 12-lead ECG showing normal sinus rhythm with appropriate P-QRS-T morphology:
10. Key Clinical Patterns to Know
| Finding | Likely Cause |
|---|---|
| ST elevation (regional) | STEMI — acute MI |
| ST depression | Ischemia, posterior MI, digoxin |
| Prolonged PR (>0.20s) | 1st-degree AV block |
| Wide QRS (>0.12s) | Bundle branch block, hyperkalemia, accessory pathway |
| Prolonged QTc | Drug toxicity, hypokalemia, hypomagnesemia, congenital LQTS |
| Peaked T waves | Hyperkalemia |
| Pathological Q waves | Prior MI |
| Delta wave (slurred QRS upstroke) | Wolff-Parkinson-White syndrome |
| Osborn J wave | Hypothermia |
| No P waves, irregularly irregular | Atrial fibrillation |
| Sawtooth flutter waves | Atrial flutter (typically 300 bpm atrial rate, 2:1 block → 150 ventricular) |
Sources: Guyton and Hall Textbook of Medical Physiology; Goldman-Cecil Medicine, 14th Ed; Miller's Anesthesia, 10th Ed; Harriet Lane Handbook, 23rd Ed.
Want me to go deeper on any specific topic — arrhythmias, bundle branch blocks, STEMI patterns, or axis determination?
This is a shared conversation. Sign in to Orris to start your own chat.