Lumbar sympathectomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Searching PubMed
"lumbar sympathectomy" AND peripheral vascular disease
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Lumbar Sympathectomy
Definition and Background
Lumbar sympathectomy is the interruption of the lumbar sympathetic chain ganglia (L1-L4), abolishing sympathetic outflow to the lower limbs and pelvic viscera. It was widely performed in the 1940s-1960s for hypertension and lower limb ischaemia, but its clinical role has progressively narrowed as endovascular and pharmacological treatments have improved.
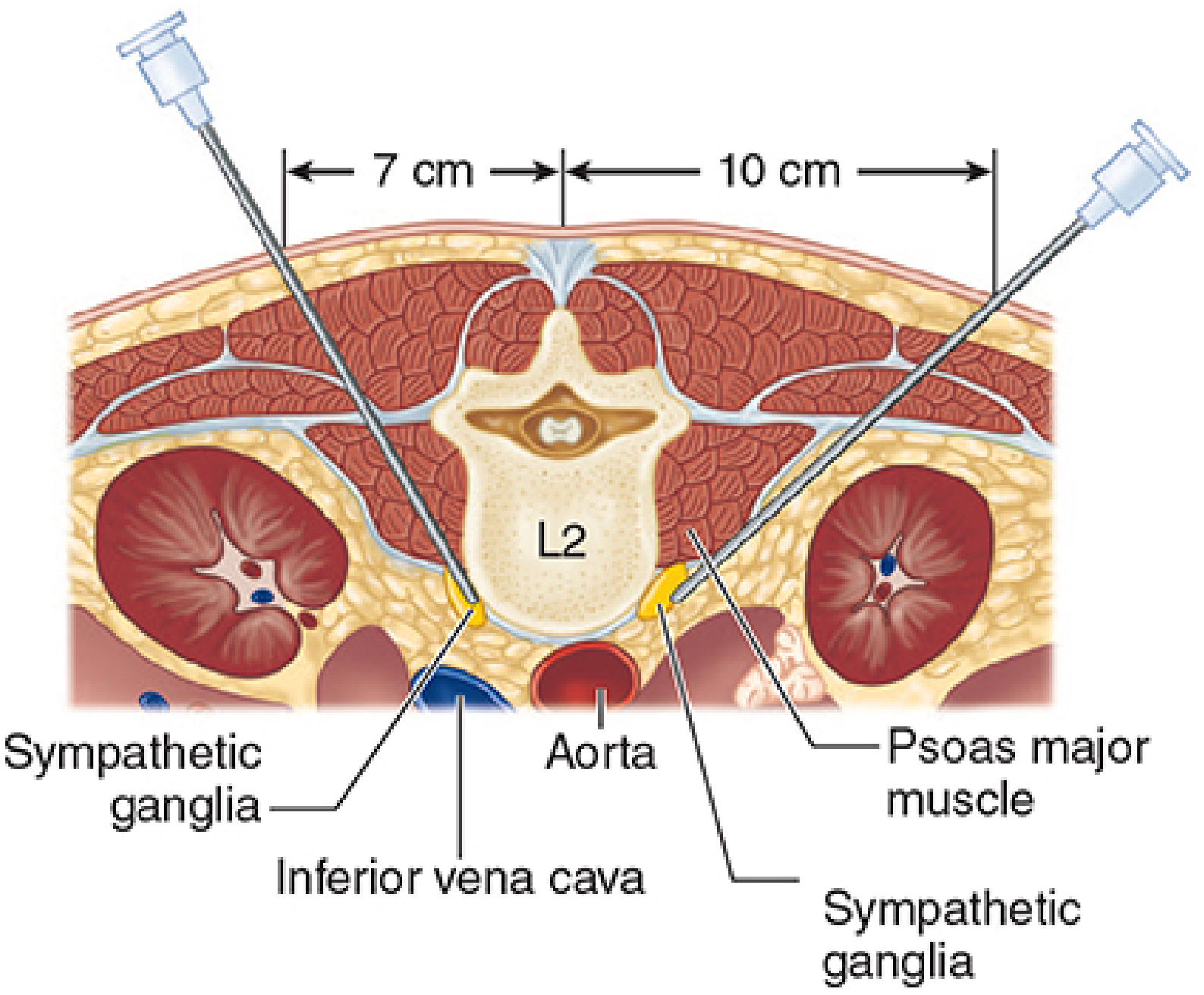
Anatomy
The lumbar sympathetic chain contains 3-5 ganglia and is a direct caudal continuation of the thoracic sympathetic trunk. Key relations:
- Lies anterior to the psoas muscle and fascia
- Located in a more anteromedial position relative to the lumbar vertebral bodies than the thoracic ganglia
- On the right side: typically posterior to the inferior vena cava
- On the left side: just lateral to the aorta
- Supplies sympathetic fibers to the lower limbs and also to the pelvic plexus
The ganglia most targeted are L2 and L3. Sympathetic preganglionic neurons originate from T1-L3 spinal cord segments.
Indications
The indications are now limited:
| Category | Indication |
|---|---|
| Vascular | Chronic lower limb ischaemia with rest pain or skin ulceration not amenable to reconstruction |
| Pain | Painful conditions of the lower extremities or pelvis (causalgia, complex regional pain syndrome) |
| Dermatology | Plantar hyperhidrosis (sympathectomy at the lumbar level); Raynaud's phenomenon of the lower limb |
| Oncology | Pelvic cancer pain unresponsive to other blocks |
| Historical | Hypertension treatment (1940s-50s - now obsolete) |
Sympathectomy tends to be used to relieve rest pain or aid the healing of skin ulcers in patients who are either medically unstable or who have not responded fully to vascular reconstruction - Pye's Surgical Handicraft.
Bailey & Love is explicit: lumbar sympathectomy for lower limb ischaemia "has become obsolete," largely replaced by endovascular interventions.
Methods of Lumbar Sympathectomy
1. Chemical (Neurolytic) Sympathectomy - most common today
This is the preferred minimally invasive approach:
- Patient positioned prone or lateral
- Single-needle technique at L3 is most commonly employed
- Needle inserted at the upper edge of the L3 spinous process, directed above or just lateral to the transverse process
- Fluoroscopic or ultrasound guidance is used
- Lignocaine is infiltrated along the needle track first (diagnostic and analgesic)
- Confirmation of correct placement: warming of the affected lower limb
- If placement is correct: 5-10 mL of 5% phenol is injected (neurolytic agent)
- Many clinicians prefer phenol for lumbar sympathetic block (vs. alcohol which is preferred for celiac plexus)
- "This technique is often best done by experts in pain relief as severe complications can arise if the phenol is injected in the wrong place" - Pye's
2. Surgical (Open) Sympathectomy - largely historical
- Retroperitoneal approach to the lumbar chain
- Resection of L2-L4 ganglia and the intervening chain
- Now rarely performed
3. Laparoscopic Sympathectomy
- Described as a minimally invasive surgical option, including in urological procedures
Physiological Effects
Following lumbar sympathectomy:
- Vasodilation of lower limb vessels - loss of sympathetic vasoconstrictor tone causes increased skin blood flow and warmth
- Orthostatic hypotension - pooling of blood in the splanchnic bed and lower extremities causes faintness and syncope on standing; patients tend to faint when standing but compensate over months by increased use of muscle pumps
- Loss of sweating (anhidrosis) over the denervated lower limb - this is the most consistent effect; exploited for plantar hyperhidrosis
- Ejaculatory dysfunction - retrograde ejaculation or emission failure may occur; semen is ejaculated into the posterior urethra and bladder due to paralysis of the periurethral muscle at the verumontanum (colliculus seminalis). Bilateral sympathectomy at L2 is particularly implicated.
Complications
| Complication | Mechanism |
|---|---|
| Orthostatic hypotension | Loss of sympathetic vasoconstrictor reflexes; most pronounced effect |
| Retrograde ejaculation | Disruption of L2 sympathetic outflow controlling internal urethral sphincter |
| Genitofemoral neuralgia | The genitofemoral nerve may be blocked or damaged during needle placement |
| Intravascular injection | Into the vena cava, aorta, or lumbar vessels |
| Somatic nerve block / damage | Lumbar plexus injury from misplaced needle or spread of neurolytic |
| Postsympathectomy neuralgia | Burning pain in the thigh, typically weeks after the procedure (thought to be deafferentation pain) |
| Phenol spread to wrong tissue | If the neurolytic agent is not in the correct retroperitoneal plane |
Comparison with Thoracic Sympathectomy
| Feature | Lumbar | Thoracic (T2-T3) |
|---|---|---|
| Target | Lower limbs | Upper limbs, palms, axillae |
| Main current indication | Plantar hyperhidrosis, rest pain palliation | Palmar/axillary hyperhidrosis (endoscopic) |
| Key complication | Retrograde ejaculation, orthostatic hypotension | Horner syndrome, compensatory hyperhidrosis |
| Approach | Percutaneous chemical / open retroperitoneal | Endoscopic transthoracic |
Current Status
- Endoscopic transthoracic sympathectomy remains in active use for palmar/axillary hyperhidrosis
- Lumbar sympathectomy for ischaemia is largely obsolete given angioplasty and bypass surgery outcomes
- Chemical lumbar sympathetic block retains a role in palliative pain management (cancer, CRPS, inoperable ischaemia)
- The procedure should be preceded by a diagnostic block with local anaesthetic alone to confirm the pain pathway before committing to neurolysis
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e | Bailey & Love's Surgery 28e | Pye's Surgical Handicraft 22e | Adams & Victor's Principles of Neurology 12e | Medical Physiology (Boron & Boulpaep) | Smith & Tanagho's General Urology 19e
Mention indication steps and complication of lumbar sympathectomy
Based on the comprehensive research already done, here is a focused, structured answer:
Lumbar Sympathectomy: Indications, Steps, and Complications
INDICATIONS
1. Vascular / Ischaemic
- Chronic lower limb ischaemia with rest pain (inoperable or failed reconstruction)
- Ischaemic skin ulcers of the lower limb not amenable to bypass or angioplasty
- Used when the patient is medically unstable for major vascular surgery
2. Pain Conditions
- Causalgia (complex regional pain syndrome type II) of the lower extremity
- Painful legs / intractable lower limb neuropathic pain
- Pelvic cancer pain unresponsive to epidural or caudal blocks
- Painful legs-moving toes syndrome (transient relief)
3. Dermatological
- Plantar hyperhidrosis (excessive foot sweating) - sympathectomy at the lumbar level
- Raynaud's phenomenon / lower limb digital vasculopathy and ulceration
4. Historical (now obsolete)
- Hypertension treatment (widely used in the 1940s-50s, now completely replaced)
- General lower limb ischaemia management (replaced by endovascular techniques)
Key principle: Lumbar sympathectomy is used to relieve rest pain or aid healing of skin ulcers in patients who are either medically unstable OR who have not responded fully to vascular reconstruction. (Pye's Surgical Handicraft)
STEPS / TECHNIQUE
Pre-procedure
- Diagnostic block first - always perform a diagnostic block with local anaesthetic alone before any neurolytic procedure to:
- Confirm the correct pain pathway
- Assess potential efficacy
- Identify morbidity of planned neurolysis
- Confirm lower limb warming as positive response
Patient Positioning and Setup
- Patient placed prone or in the lateral decubitus position
- Imaging guidance set up - fluoroscopy (image intensifier) or ultrasound is used throughout
Needle Placement (Chemical Sympathectomy - most common modern technique)
- Single-needle technique at the L3 level is most commonly employed
- Needle inserted at the upper edge of the L3 spinous process
- Directed above or just lateral to the transverse process of L3 (direction varies with distance from midline)
- The needle is advanced until it lies anteromedial to the L3 vertebral body, anterior to the psoas fascia
Injection Sequence
- Lignocaine infiltrated along the entire needle track (local anaesthesia + diagnostic)
- Verify correct position by confirming warming of the affected lower limb
- Local anaesthetic injected immediately prior to neurolytic agent under fluoroscopic guidance
- If position confirmed: inject 5-10 mL of 5% phenol (neurolytic agent of choice for lumbar sympathetic block)
- After injection, the needle is cleared with air or saline before withdrawal - prevents damage to superficial structures along the needle tract
Post-procedure
- Monitor blood pressure (orthostatic hypotension risk)
- Assess for limb warming and pain relief
- If pain relief follows isolated sympathetic blockade signs (BP drop, no sensory/motor loss) → pain is sympathetically mediated and the block was appropriate
Note on neurolytic agents: Phenol is preferred for lumbar sympathetic block; alcohol is preferred for celiac plexus block. Phenol in glycerin is hyperbaric.
Open Surgical Sympathectomy (now rarely done)
- Retroperitoneal approach
- Resection of L2-L4 ganglia and interconnecting chain
- Largely replaced by the chemical technique
COMPLICATIONS
Immediate / Procedural
| Complication | Detail |
|---|---|
| Intravascular injection | Into the IVC (right side), aorta, or lumbar vessels - most dangerous immediate complication |
| Somatic nerve block | Inadvertent block of the lumbar plexus from needle misplacement or phenol spread |
| Genitofemoral neuralgia | The genitofemoral nerve runs along psoas and is the most commonly blocked somatic nerve; causes pain/paraesthesia in groin and inner thigh |
| Phenol in wrong tissue | If injected outside the retroperitoneal sympathetic plane, severe tissue damage can result |
Early Post-procedure
| Complication | Detail |
|---|---|
| Orthostatic hypotension | Loss of vasoconstrictor reflexes causes blood pooling in lower limbs and splanchnic bed on standing; faintness and syncope - the most pronounced physiological effect |
| Postsympathectomy neuralgia | Burning, aching pain in the anterior thigh/groin, typically appearing 1-2 weeks post-procedure; thought to be deafferentation pain; usually self-limiting over weeks to months |
Long-term / Permanent
| Complication | Detail |
|---|---|
| Retrograde ejaculation | Paralysis of the periurethral muscle at the verumontanum (colliculus seminalis); semen ejected back into the bladder; especially with bilateral L2 sympathectomy - important to counsel male patients |
| Anhidrosis | Loss of sweating over the denervated lower limb (expected; therapeutic in hyperhidrosis) |
| Compensatory hyperhidrosis | Increased sweating elsewhere on the body to compensate for anhidrosis of the denervated area |
| Return of symptoms | Sympathectomy provides time-limited benefit; vasospastic symptoms often recur after 12-18 months, though digital ulceration may remain reduced |
Special Concern
- Bilateral sympathectomy carries a significantly higher risk of orthostatic hypotension and retrograde ejaculation than unilateral
- After lumbar sympathectomy, patients tend to faint on standing but usually compensate after some months by enhanced use of lower limb muscle pumps (Medical Physiology, Boron & Boulpaep)
Summary Table
| Domain | Key Points |
|---|---|
| Best indication today | Rest pain / ischaemic ulcer (inoperable) + plantar hyperhidrosis + cancer pain |
| Preferred technique | Chemical: 5-10 mL 5% phenol at L3 under fluoroscopy |
| Most important step | Diagnostic LA block FIRST to confirm sympathetic mediation |
| Most dangerous complication | Intravascular injection (IVC/aorta) |
| Most common complication | Orthostatic hypotension + postsympathectomy neuralgia |
| Most important male-specific complication | Retrograde ejaculation |
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e | Pye's Surgical Handicraft 22e | Bailey & Love's Surgery 28e | Adams & Victor's Principles of Neurology 12e | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.