Explain stomach for my anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full anatomy of the stomach answer.
The Stomach - Anatomy
The stomach is a J-shaped, distensible dilation of the alimentary canal, interposed between the esophagus proximally and the duodenum distally. Its volume ranges from ~30 mL in a neonate to 1.5-2 L in the adult.
1. Position and Relations
The stomach lies in the left hypochondriac and epigastric regions of the abdomen:
- The esophagogastric junction sits to the left of the T10 vertebral body, 1-2 cm below the diaphragmatic hiatus
- The gastroduodenal junction lies at L1, generally right of midline
Anterior relations: liver, anterior abdominal wall
Posterior relations (forming the "stomach bed"): pancreas, transverse colon, diaphragm, spleen, left kidney and adrenal gland. The posterior gastric wall forms the anterior wall of the omental bursa (lesser sac).
2. Gross Anatomy - Parts
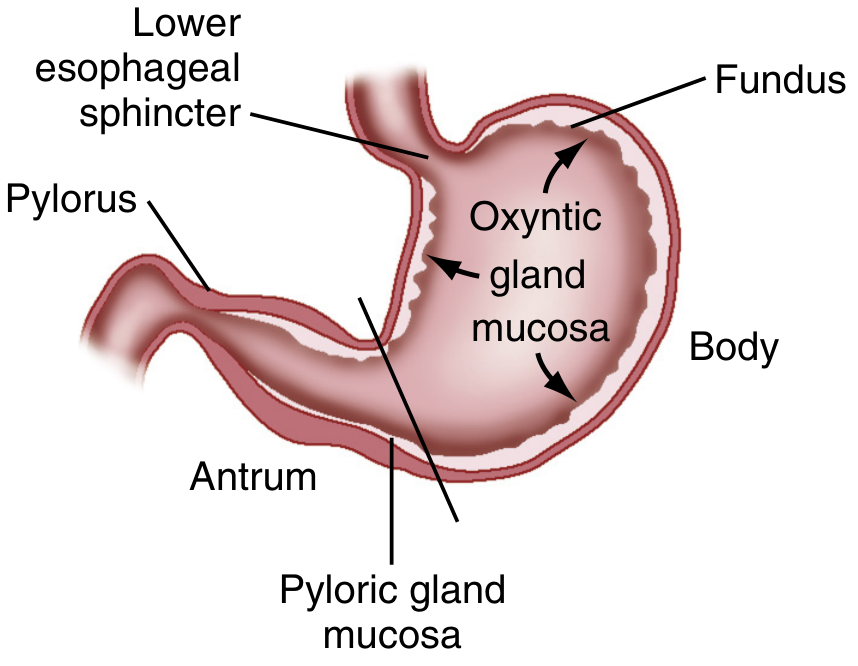
The stomach has 4 anatomical regions:
| Region | Description |
|---|---|
| Cardia | Small area immediately at the esophagogastric junction |
| Fundus | Dome-shaped superior portion, lies above the cardia, contacts the left hemidiaphragm and spleen |
| Body (Corpus) | Largest part, extends from fundus to the incisura angularis |
| Antrum + Pylorus | Distal region ending at the pyloric sphincter; the pylorus joins the duodenum at L1 |
The incisura angularis is a fixed, sharp indentation two-thirds down the lesser curvature - it marks the caudal boundary of the body.
Curvatures:
- Lesser curvature - right upper border, shorter
- Greater curvature - left lower border, longer; may extend below the umbilicus when distended
3. Peritoneal Attachments (Ligaments)
The stomach is almost completely covered by peritoneum. This peritoneum extends as:
| Ligament | From - To |
|---|---|
| Lesser omentum (gastrohepatic part) | Lesser curvature → liver |
| Greater omentum / Gastrocolic ligament | Greater curvature → transverse colon |
| Gastrosplenic ligament | Greater curvature → spleen |
| Gastrophrenic ligament | Fundus → diaphragm |
4. Blood Supply
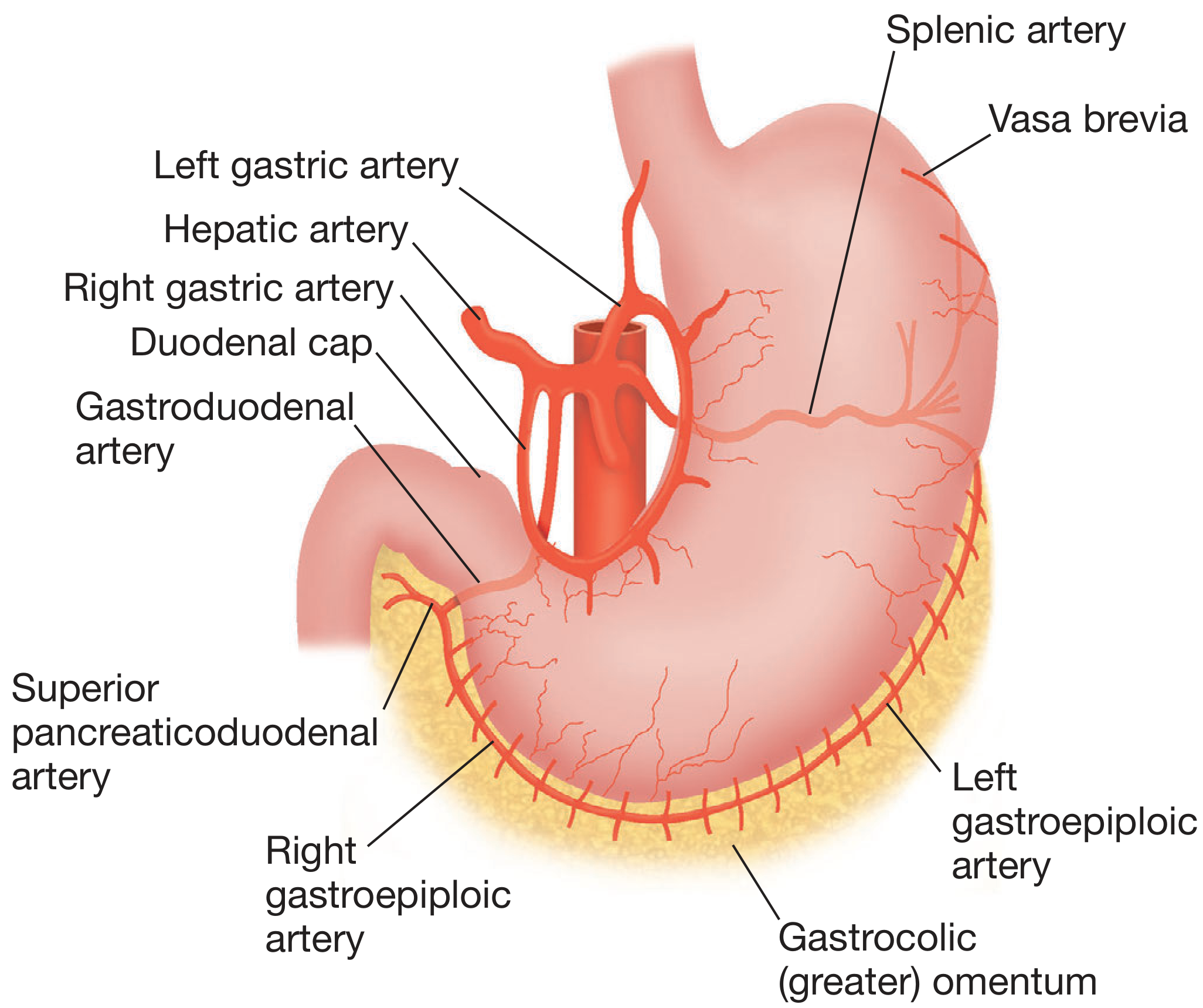
All arterial supply derives from the celiac trunk via three branches:
Lesser curvature arcade:
- Left gastric artery (direct celiac branch) - from above
- Right gastric artery (from common hepatic artery) - from below
Greater curvature arcade:
- Left gastroepiploic artery (from splenic artery) - from above/left
- Right gastroepiploic artery (from gastroduodenal artery) - from below/right
Fundus:
- Short gastric arteries (vasa brevia) - from the terminal splenic artery
The gastroduodenal artery passes behind the first part of the duodenum - clinically important because a posterior duodenal ulcer can erode it causing severe bleeding.
Venous drainage: Mirrors the arteries, all draining ultimately into the portal vein (or its tributaries - splenic and superior mesenteric veins). The left gastric (coronary) vein becomes dilated in portal hypertension, forming oesophageal varices.
5. Lymphatic Drainage
Most gastric lymph drains ultimately to the celiac nodes via 4 intermediate groups:
- Inferior gastric → subpyloric/omental → hepatic → celiac
- Splenic/superior greater curvature → pancreaticosplenic → celiac
- Superior gastric/lesser curvature → left & right gastric nodes → celiac
- Hepatic/pyloric → suprapyloric → hepatic → celiac
Lymphatics anastomose freely within the gastric wall - this explains why gastric cancer can spread widely before detection.
6. Nerve Supply
Parasympathetic (vagus nerve):
- Left and right vagus nerves form the anterior and posterior vagal trunks at the cardia
- Each trunk gives celiac and hepatic branches, then continues as the anterior and posterior nerves of Latarjet (running in the lesser omentum)
- These give multiple gastric branches and end as the "crow's foot" at the antrum
- Due to the 90° embryological rotation: left vagus = anterior trunk; right vagus = posterior trunk
Sympathetic:
- Preganglionic fibers from T6-T8, synapsing in the celiac ganglia
- Postganglionic fibers travel with blood vessels
- Carry afferent pain fibers and motor fibers to the pyloric sphincter
7. Histology - Wall Layers
The stomach wall has the standard GI layers (mucosa, submucosa, muscularis propria, serosa) with some specializations:
Muscularis propria has 3 layers (unlike the rest of the GI tract which has 2):
- Outer longitudinal
- Middle circular
- Inner oblique (unique to stomach - helps churning)
The pyloric sphincter is a thickening of the circular muscle layer.
8. Microscopic Anatomy - Gastric Mucosa
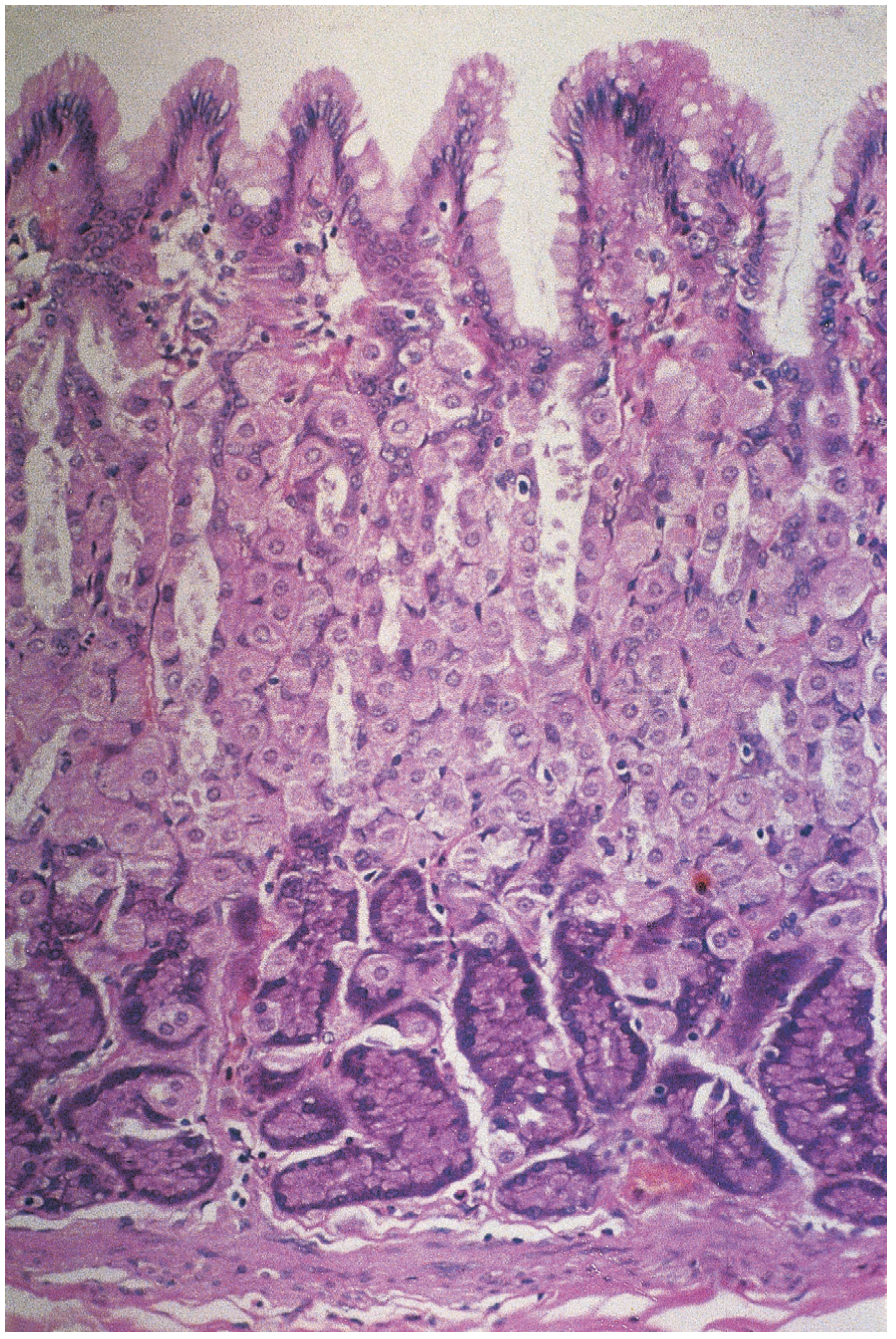
The entire mucosa is lined by columnar epithelium with numerous gastric pits (crypts) - tubular invaginations each opening into 4-5 gastric glands.
Three types of gastric glands:
Cardiac glands
- Adjacent to the esophagogastric junction
- Contain mucous, endocrine, and undifferentiated cells
- No parietal or chief cells
Oxyntic (parietal) glands - Body & Fundus (75-80% of stomach)
Contain three specialized cell types:
| Cell | Location in gland | Secretion | Function |
|---|---|---|---|
| Parietal cells | Upper/mid gland | HCl + Intrinsic Factor | Acid secretion via H⁺/K⁺-ATPase; essential for B12 absorption |
| Chief cells | Deepest part | Pepsinogen I & II | Protein digestion (activated to pepsin by acid) |
| Surface mucous cells | Mucosal surface | Mucus | Protective barrier |
Pyloric glands - Antrum (15-25% of stomach)
- Contain G cells (secrete gastrin - stimulates acid)
- D cells (secrete somatostatin - inhibits acid)
ECL cells (enterochromaffin-like) are distributed throughout the body and produce histamine, a key driver of parietal cell acid secretion.
9. Functional Areas Summary
| Functional Zone | Anatomical Region | Key Cells/Function |
|---|---|---|
| Oxyntic gland area | Cardia, Fundus, Body | Parietal cells (HCl), Chief cells (pepsinogen) |
| Pyloric gland area | Antrum + Pylorus | G cells (gastrin), antral pump for gastric emptying |
10. Embryology (Brief)
The stomach is recognizable at week 4 as a dilation of the distal foregut. It rotates 90° around its longitudinal axis, which explains:
- Greater curvature points left (was dorsal)
- Lesser curvature points right (was ventral)
- Left vagus innervates the anterior wall; right vagus innervates the posterior wall
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Ch. 49 | Bailey & Love's Short Practice of Surgery, 28th ed., Ch. 67 | Yamada's Textbook of Gastroenterology, 7th ed., Ch. 17
This is a shared conversation. Sign in to Orris to start your own chat.