Differential diagnosis of nummular eczema
"nummular eczema" OR "discoid eczema" AND "differential diagnosis"
Differential Diagnosis of Nummular Eczema

Most Likely (Common Mimics)
| Condition | Key Distinguishing Features |
|---|---|
| Allergic contact dermatitis | Geometric distribution matching allergen exposure; history of contactant (nickel, fragrance, rubber, neomycin); positive patch testing (32-50% of NE patients have relevant positive tests - these may overlap or be primary cause) |
| Atopic dermatitis (nummular type) | More chronic/lichenified lesions; personal/family history of atopy; begins in childhood; flexural predilection; elevated IgE common; nummular morphology more typical in adolescents with AD |
| Stasis dermatitis | Restricted to lower legs with dependent edema; associated with varicose veins and hemosiderin deposition; can mimic or disseminate as nummular plaques |
| Tinea corporis | Must always be ruled out - KOH scraping shows hyphae; active scaly border with central clearing (central sparing); single or few lesions common; responds to antifungals; NE lacks central clearing |
Consider
| Condition | Key Distinguishing Features |
|---|---|
| Psoriasis (longstanding plaques) | Silvery micaceous scale; Auspitz sign; nail pitting/onycholysis; well-defined plaques at extensor elbows, knees, scalp; Koebner phenomenon; family history; biopsy shows acanthosis, dilated capillaries, neutrophilic parakeratosis without spongiosis |
| Impetigo | Honey-colored crusts; rapidly spreading; fever; positive bacterial culture; common in children; responds to antibiotics |
| Mycosis fungoides (CTCL) | Longstanding, recalcitrant plaques; may be misdiagnosed for years; photodistributed early lesions; skin biopsy with atypical lymphocytes in epidermis (epidermotropism); CD4+ T-cell dominance; clonal TCR rearrangement |
| Paget disease | Unilateral involvement of nipple/areola only; persistent, resistant to steroids; biopsy shows large pale Paget cells |
| Bullous pemphigoid | Tense blisters, not vesicles; urticarial prodrome; elderly; direct immunofluorescence shows IgG + C3 at dermoepidermal junction |
| Pemphigus vulgaris | Flaccid blisters; mucosal involvement; Nikolsky sign positive; acantholysis on biopsy; IgG against desmoglein |
| Bowen disease (SCC in situ) | Solitary, slowly enlarging, sharply defined plaque; hyperkeratotic/scaly surface; sun-exposed or anogenital sites; biopsy shows full-thickness epidermal dysplasia |
Other Nummular Dermatoses to Consider
| Condition | Key Distinguishing Features |
|---|---|
| Fixed drug eruption | Recurs at same site(s) with drug re-exposure; often hyperpigmented; medication history |
| Pityriasis rotunda | Circular, scaly, hyperpigmented or hypopigmented patches; often in Asian or African patients; associated with systemic disease (malignancy, liver disease) |
| Erythema migrans (Lyme disease) | Expanding annular erythema; central clearing; tick exposure; flu-like illness; southern/mid-Atlantic endemic area; not vesicular or crusted |
Always Rule Out
- Tinea corporis - KOH preparation and/or fungal culture is mandatory in all cases before initiating steroid therapy, as steroids will worsen tinea (tinea incognito).
Diagnostic Approach
- KOH preparation - first step to exclude tinea corporis
- Patch testing - indicated in chronic/recalcitrant cases; clinically relevant allergens found in 12-67% of positive testers
- Skin biopsy - if psoriasis, CTCL, bullous pemphigoid, or Bowen disease is suspected; histology shows spongiotic dermatitis (acute), or parakeratosis, scale crust, psoriasiform hyperplasia (subacute)
- Bacterial culture - if impetigo or secondary infection suspected
- Direct immunofluorescence - if autoimmune blistering disorder is in the differential
Create a diagnostic algorithm or decision tree for nummular eczema vs. mimics
A professional medical diagnostic algorithm / decision tree flowchart titled "Diagnostic Algorithm: Nummular Eczema vs. Mimics". Clean white background, dark navy blue and teal color scheme, medical textbook style. The flowchart starts at the top with a rounded rectangle: "Coin-shaped (nummular) erythematous plaque(s)" with an arrow pointing down. First decision diamond: "KOH scrape / fungal culture positive?" - YES arrow → right → rounded box (green): "TINEA CORPORIS — Active scaly border, central clearing, hyphae on KOH → Antifungal therapy" - NO arrow → down Second decision diamond: "Tense blisters / bullae present?" - YES arrow → right → rounded box (green): "Consider BULLOUS PEMPHIGOID or PEMPHIGUS — Send DIF biopsy; IgG+C3 at DEJ = BP; flaccid blisters + mucosal involvement = PV" - NO arrow → down Third decision diamond: "Honey-colored crusts? Rapid spread? Child?" - YES arrow → right → rounded box (green): "IMPETIGO — Bacterial culture; antibiotic therapy" - NO arrow → down Fourth decision diamond: "Thick silvery scale? Auspitz sign? Nail pitting? Extensor surfaces?" - YES arrow → right → rounded box (green): "PSORIASIS — Biopsy: acanthosis, neutrophilic parakeratosis, dilated capillaries" - NO arrow → down Fifth decision diamond: "Lesion confined to nipple/areola (unilateral)?" - YES arrow → right → rounded box (green): "PAGET DISEASE — Biopsy: large pale Paget cells" - NO arrow → down Sixth decision diamond: "Longstanding recalcitrant plaques > 6 months, no response to steroids?" - YES arrow → right → rounded box (orange): "Consider MYCOSIS FUNGOIDES (CTCL) — Biopsy: epidermotropism, atypical CD4+ T cells, TCR gene rearrangement" - NO arrow → down Seventh decision diamond: "Contact allergen history? Geometric distribution?" - YES arrow → right → rounded box (teal): "ALLERGIC CONTACT DERMATITIS — Patch testing (common: nickel, fragrance, neomycin, rubber)" - NO arrow → down Eighth decision diamond: "Lower leg location? Varicose veins? Edema? Hemosiderin pigmentation?" - YES arrow → right → rounded box (teal): "STASIS DERMATITIS — Compression therapy; treat venous insufficiency" - NO arrow → down Ninth decision diamond: "Personal/family history of atopy? Flexural involvement? Elevated IgE? Child?" - YES arrow → right → rounded box (teal): "ATOPIC DERMATITIS (nummular type) — More lichenified, chronic; treat as AD" - NO arrow → down Final rounded rectangle at bottom (navy blue, white text): "NUMMULAR ECZEMA (Discoid Eczema) — Spongiotic dermatitis on biopsy; patch test if recalcitrant; treat with potent TCS ± NB-UVB" Add a small legend box in the bottom right: Green = rule out first; Orange = biopsy-urgent; Teal = further workup needed; Navy = diagnosis Clean arrows, well-spaced nodes, professional font, portrait orientation, suitable for a medical textbook or clinical reference poster.
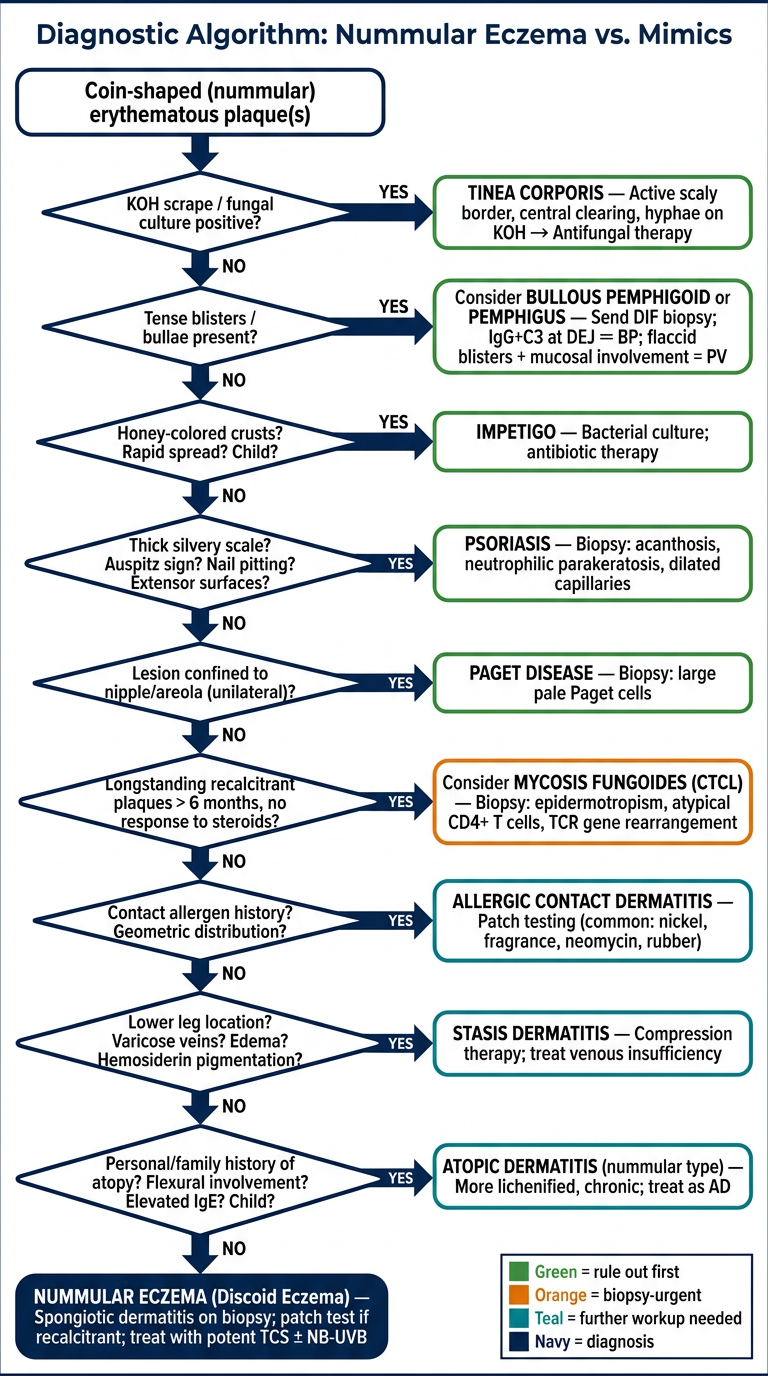
- KOH scrape first - tinea corporis must be excluded before any steroid is applied (steroids worsen tinea, causing "tinea incognito")
- Blistering disorders next - bullous pemphigoid and pemphigus present urgently and require DIF biopsy
- Impetigo - quick to diagnose clinically, especially in children
- Psoriasis - distinguished by thick silvery scale, Auspitz sign, nail changes, extensor predominance
- Paget disease - rare but important; always consider if a unilateral nipple/areola plaque fails to respond
- Mycosis fungoides - flagged for any chronic, steroid-resistant plaque over 6 months; biopsy with TCR rearrangement testing
- Allergic contact dermatitis - patch testing is indicated here; up to 50% of NE patients have a relevant positive allergen
- Stasis dermatitis - lower-leg distribution with venous signs
- Atopic dermatitis (nummular type) - more lichenified, chronic, flexural, with atopic history
- Nummular eczema - diagnosis of exclusion at the bottom, confirmed by spongiotic biopsy if needed