
b9f31777-bdef-4345-838f-401b2b75b9e1.jpeg
Explain questions 3
Reading File
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything I need to give a complete, well-sourced answer to all four sub-parts of Q3.
Q3 - Full Answer: Scurvy (Vitamin C Deficiency)
Clinical Case Summary
A 5-year-old boy from a low socioeconomic family presents with:
- Bleeding gums, swollen gums
- Joint pain and fatigue
- Petechiae over the lower limbs
- Splinter hemorrhages under nails
a) Most Probable Diagnosis (1 mark)
Scurvy - caused by Vitamin C (Ascorbic Acid) deficiency
The classic triad of bleeding gums + perifollicular/skin petechiae + joint pain in a malnourished child from a low-income family is pathognomonic of scurvy. Splinter nail hemorrhages and fatigue are additional supporting features. In children, this is also called Barlow's disease (infantile scurvy).
b) Biochemical Basis of Symptoms (3 marks)
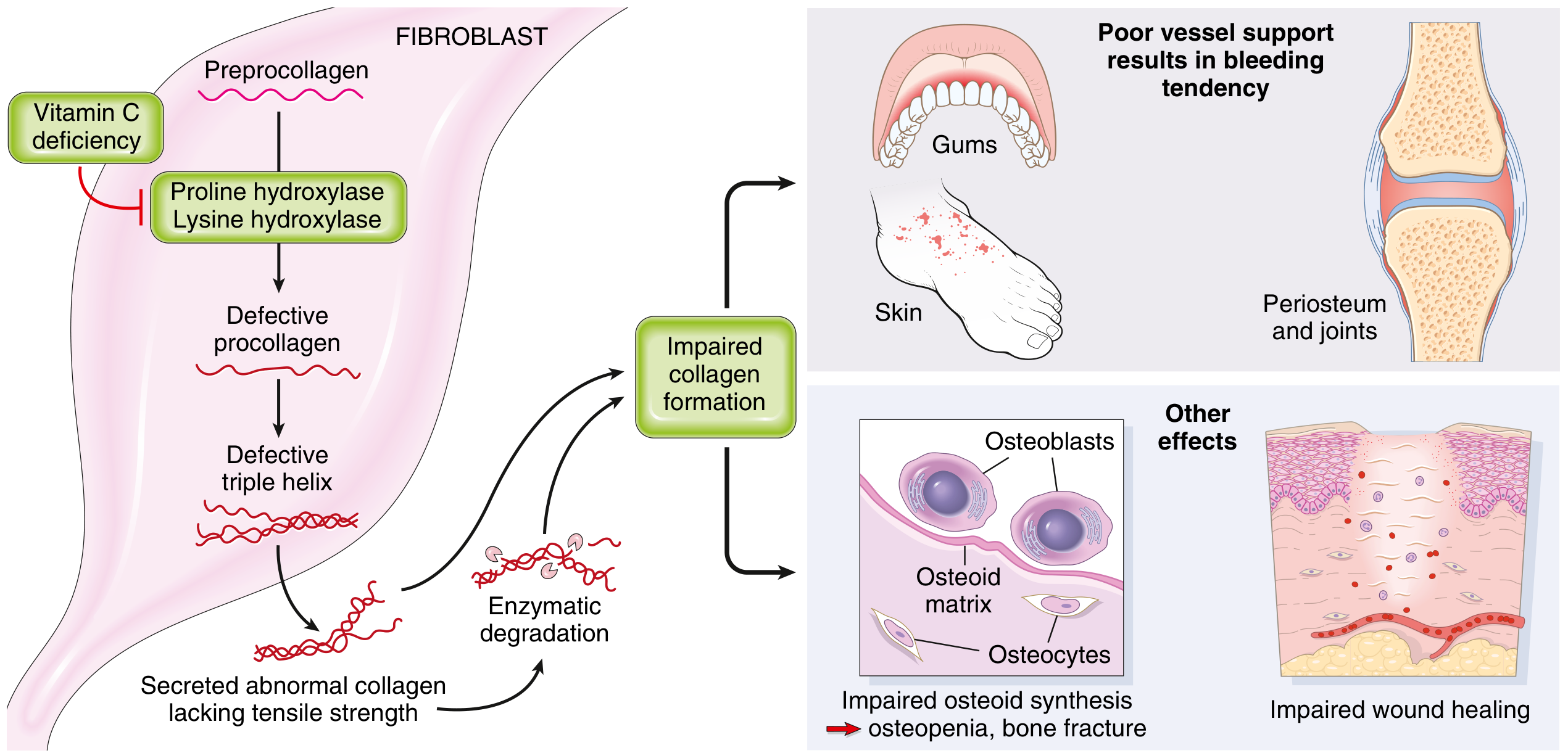
The root cause is impaired collagen synthesis due to deficiency of Vitamin C.
How Vitamin C works normally:
Ascorbic acid is an essential cofactor for two key enzymes:
- Prolyl hydroxylase - hydroxylates proline residues to hydroxyproline
- Lysyl hydroxylase - hydroxylates lysine residues to hydroxylysine
These reactions are required to form a stable triple helix in procollagen. Hydroxyproline provides the hydrogen bonds that hold the three alpha chains together, and hydroxylysine allows cross-linking between collagen fibers.
What goes wrong in Vitamin C deficiency:
| Step | Consequence |
|---|---|
| Prolyl and lysyl hydroxylases are inactive | Proline and lysine residues are not hydroxylated |
| Procollagen cannot form a stable helix | Defective, unstable procollagen is produced |
| Poorly crosslinked collagen is secreted | Lacks tensile strength; more soluble and degraded faster |
| Collagen in blood vessel walls is defective | Vascular fragility → hemorrhages, petechiae, splinter bleeds |
| Periosteal collagen is defective | Joint pain, periosteal hemorrhages, bone abnormalities |
| Synthesis of collagen polypeptides is also suppressed | Independent of hydroxylation effects |
The diagram below (from Robbins & Kumar Basic Pathology) summarizes this beautifully:
Explaining each symptom biochemically:
-
Bleeding/swollen gums: Gum tissue is rich in collagen. Defective collagen in the gingival vessels and connective tissue causes capillary fragility and gingival hemorrhage.
-
Petechiae and splinter hemorrhages: Blood vessel walls lack adequate collagen support, so minor trauma causes pinpoint bleeds (petechiae) and linear bleeds under nails (splinter hemorrhages). Collagen, having the highest content of hydroxyproline of any protein, is most severely affected in blood vessels.
-
Joint pain: Periosteal and periarticular collagen is defective, causing subperiosteal hemorrhages and joint effusions, especially in growing bones.
-
Fatigue/anemia: Vitamin C is required for the synthesis of carnitine (via hydroxylation steps) and for norepinephrine synthesis (dopamine beta-hydroxylase). Deficiency impairs energy metabolism. Vitamin C also enhances non-heme iron absorption; its absence contributes to iron-deficiency anemia.
-
Robbins & Kumar Basic Pathology, p. 296-297
-
Tietz Textbook of Laboratory Medicine, 7th Ed, p. 1303
c) Role of the Deficient Agent (Vitamin C) in Collagen Synthesis (4 marks)
Collagen is synthesized in a complex multi-step process. Vitamin C plays a direct and indispensable role:
Steps of Collagen Synthesis and Where Vitamin C Acts:
-
Transcription and Translation: The COL genes are transcribed and translated on the RER to produce preprocollagen (with a signal peptide).
-
Hydroxylation of Proline and Lysine (VITAMIN C IS REQUIRED HERE):
- Inside the ER, prolyl 4-hydroxylase and lysyl hydroxylase act on proline and lysine residues.
- Vitamin C (ascorbate) keeps the Fe²⁺ ion in the enzyme's active site in its reduced state, preventing oxidation to Fe³⁺ which would inactivate the enzyme.
- This produces hydroxyproline and hydroxylysine.
- Hydroxyproline stabilizes the triple helix via hydrogen bonds.
- Hydroxylysine provides sites for cross-linking and glycosylation.
-
Triple Helix Formation:
- Three alpha chains associate at their C-terminus and wind into a right-handed triple helix stabilized by hydroxyproline-dependent hydrogen bonds.
- Without adequate hydroxylation, the helix is unstable and cannot be properly secreted.
-
Secretion and Cleavage:
- Procollagen is secreted into the extracellular space.
- Procollagen peptidases cleave the propeptides to yield tropocollagen.
-
Cross-linking (VITAMIN C IS REQUIRED HERE INDIRECTLY):
- Lysyl oxidase oxidizes hydroxylysine and lysine to form allysine, which then participates in covalent cross-linking between adjacent tropocollagen molecules.
- Cross-linking gives collagen its tensile strength.
- Without Vitamin C, inadequate hydroxylysine means poor cross-linking.
In summary: Without Vitamin C:
-
Prolyl and lysyl hydroxylases are inactive
-
Procollagen cannot form a stable helix
-
Secreted collagen is defective, lacks tensile strength, and is rapidly degraded
-
All collagen-rich tissues (blood vessels, skin, bone, gums) become structurally weak
-
Robbins & Kumar Basic Pathology, p. 296
-
Harper's Illustrated Biochemistry, 32nd Ed
-
Tietz Textbook of Laboratory Medicine, 7th Ed, p. 1303
d) Dietary Sources and RDA of Vitamin C in Children (2 marks)
Dietary Sources (rich sources first):
| Category | Examples |
|---|---|
| Fruits | Citrus fruits (oranges, lemons, limes), guava, kiwi, strawberries, papaya, mango, amla (Indian gooseberry - extremely rich) |
| Vegetables | Bell peppers (capsicum), broccoli, tomatoes, cabbage, spinach, Brussels sprouts, green chillies |
| Other | Liver, fish (small amounts in animal products) |
Note: Vitamin C is heat-labile and water-soluble, so cooking destroys a significant portion. This is why children in low-income families eating mainly cooked, non-fresh diets are at risk.
RDA for Vitamin C (as per US Institute of Medicine / ICMR):
| Age Group | RDA (mg/day) |
|---|---|
| 0-6 months (AI) | 40 mg/day |
| 7-12 months (AI) | 50 mg/day |
| 1-3 years | 15 mg/day |
| 4-8 years | 25 mg/day |
| 9-13 years | 45 mg/day |
| Adults (males >19 yrs) | 90 mg/day |
| Adults (females >19 yrs) | 75 mg/day |
Minimum to prevent scurvy: Only ~10 mg/day is sufficient to cure clinical scurvy, but the RDA is set higher to maintain tissue saturation.
- Tietz Textbook of Laboratory Medicine, 7th Ed, p. 1303-1304
- Harper's Illustrated Biochemistry, 32nd Ed
Summary Box
| Sub-question | Key Answer |
|---|---|
| a) Diagnosis | Scurvy (Vitamin C deficiency / Barlow's disease in children) |
| b) Biochemical basis | Vit C is cofactor for prolyl/lysyl hydroxylase → defective collagen → vascular fragility (bleeds, petechiae), joint pain, anemia |
| c) Role in collagen synthesis | Keeps Fe²⁺ active in hydroxylases → hydroxyproline/lysine formation → stable triple helix + cross-linking |
| d) Sources & RDA | Citrus fruits, guava, amla, bell peppers, broccoli; RDA 25 mg/day (4-8 yrs), 45 mg/day (9-13 yrs) |
Mechanism of action of steroids hormone
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have everything needed. Let me now give a complete, well-illustrated answer.
Mechanism of Action of Steroid Hormones
Overview
Steroid hormones (glucocorticoids, mineralocorticoids, sex hormones - estrogen, progesterone, testosterone, and also Vitamin D and thyroid hormones) are lipophilic molecules derived from cholesterol. Because they are fat-soluble, they diffuse freely across the cell membrane and exert their effects by binding to intracellular nuclear receptors that function directly as gene-specific transcription factors.
This is fundamentally different from peptide/protein hormones (like insulin, adrenaline) which act on cell-surface receptors and use second messengers.
Step-by-Step Mechanism
Step 1 - Synthesis and Transport
- Steroid hormones are synthesized in endocrine glands (adrenal cortex, gonads, placenta).
- They are lipid-soluble and do not dissolve freely in plasma; they are carried bound to carrier proteins (e.g., cortisol-binding globulin, sex hormone-binding globulin).
- The free (unbound) fraction is biologically active.
Step 2 - Membrane Crossing
- The free hormone diffuses passively across the lipid bilayer of the target cell membrane - no receptor or transporter needed.
- (Thyroid hormones, though not true steroids, use carrier-mediated transporters to enter cells.)
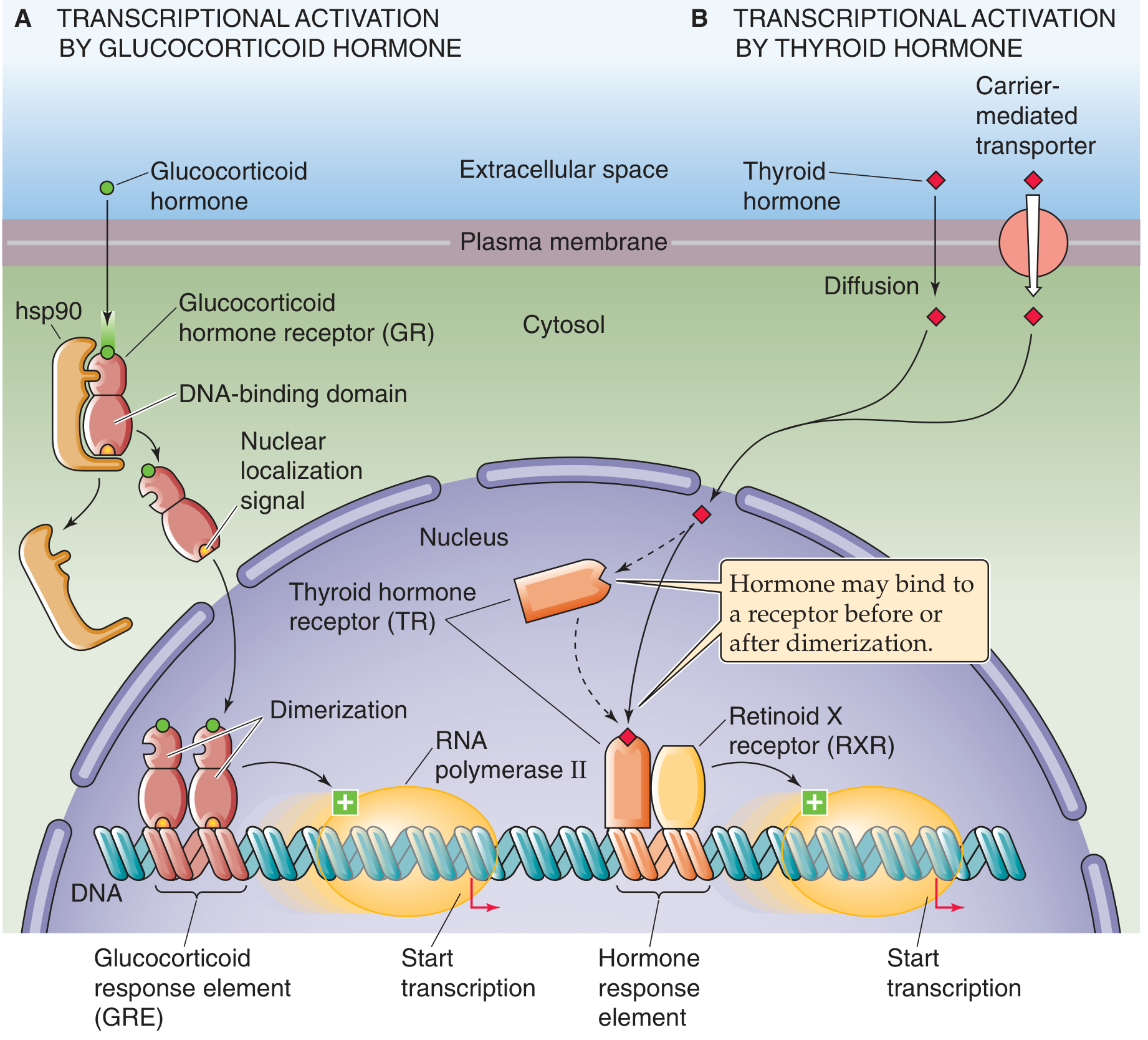
Step 3 - Binding to the Cytoplasmic Receptor (Type I - Glucocorticoid/Mineralocorticoid/Sex Hormone Model)
In the cytoplasm, the receptor (e.g., Glucocorticoid Receptor, GR) exists in an inactive state - bound to a chaperone protein called Heat Shock Protein 90 (Hsp90).
- Hsp90 keeps the receptor in the cytoplasm and masks the nuclear localization signal (NLS).
- Hsp90 also maintains the ligand-binding domain in a conformation that has high affinity for the hormone.
When the steroid hormone binds to the receptor's Ligand-Binding Domain (LBD):
- Hsp90 dissociates from the receptor.
- The Nuclear Localization Signal (NLS) is exposed.
- A conformational change occurs in the receptor.
Step 4 - Dimerization and Nuclear Translocation
- Two hormone-receptor complexes come together and form a homodimer (for glucocorticoid, androgen, progesterone, estrogen receptors).
- The dimer is transported through the nuclear pore into the nucleus via the exposed NLS.
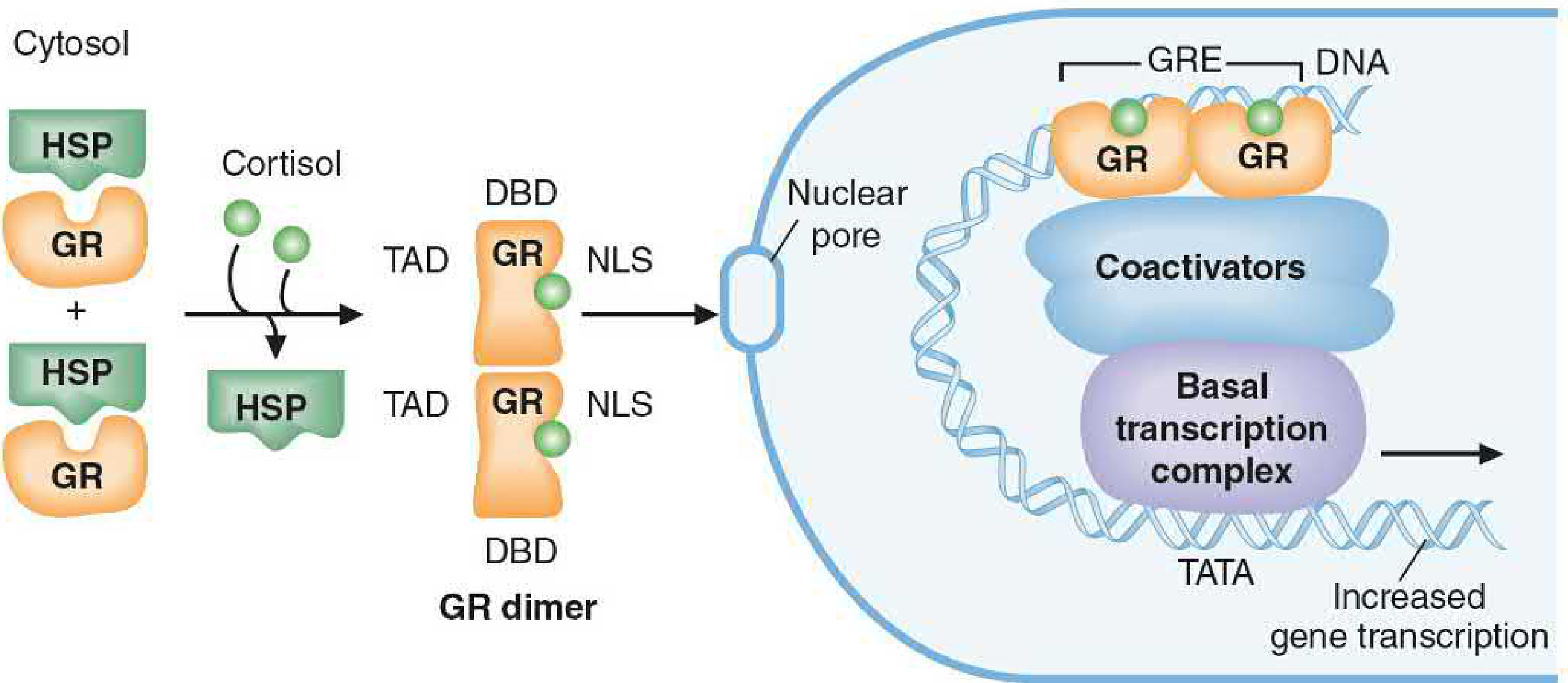
Step 5 - Binding to Hormone Response Element (HRE)
Inside the nucleus, the receptor homodimer's DNA-Binding Domain (DBD) binds to specific short DNA sequences in the promoter/enhancer regions of target genes called Hormone Response Elements (HREs).
For glucocorticoids, this is called the Glucocorticoid Response Element (GRE).
- Each class of steroid hormone has its own specific HRE sequence.
- HREs are typically palindromic hexanucleotide sequences.
Step 6 - Transcriptional Activation or Repression
Once bound to the HRE, the receptor's Transactivation Domain (TAD) recruits:
- Coactivators (e.g., SRC/p160 family, CBP/p300) - which have Histone Acetyltransferase (HAT) activity - loosen chromatin structure, making DNA more accessible.
- Mediator proteins / TRAP220 - which recruit the Basal Transcription Complex (RNA Pol II + general transcription factors) to the TATA box.
- Chromatin remodeling complexes (e.g., SWI/SNF via Brg1) - slide nucleosomes off DNA.
- Histone methyltransferases (e.g., CARM1) - further enhance transcription.
The result: Increased (or decreased) transcription of specific target genes.
- The mRNA produced is then translated into new effector proteins that produce the biological response.
Step 7 (Type II Receptors - Thyroid Hormone / Retinoic Acid Model - Contrast)
Some nuclear receptors (e.g., Thyroid Hormone Receptor, TR) are already inside the nucleus before hormone binding:
- They form heterodimers with Retinoid X Receptor (RXR) and are constitutively bound to HREs.
- In the absence of hormone, they bind corepressors (with HDAC activity) and repress transcription.
- When the hormone binds, the receptor undergoes a conformational change, corepressors are released, coactivators are recruited, and transcription is activated.
Domains of the Steroid Hormone Receptor
| Domain | Abbreviation | Function |
|---|---|---|
| Transactivation Domain | TAD | Binds coactivators; activates transcription |
| DNA-Binding Domain | DBD | Binds to Hormone Response Element on DNA |
| Ligand-Binding Domain | LBD | Binds the steroid hormone |
| Nuclear Localization Signal | NLS | Directs receptor to the nucleus after hormone binding |
| Dimerization Site | - | Allows two receptor molecules to pair |
| Inhibitor-Binding Site | - | Binds Hsp90; masks NLS in absence of hormone |
Key Features Compared to Peptide Hormone Signaling
| Feature | Steroid Hormones | Peptide Hormones |
|---|---|---|
| Receptor location | Intracellular (cytoplasm/nucleus) | Cell surface |
| Mechanism | Direct gene regulation | Second messenger cascade |
| Onset of action | Slow (hours to days - needs new protein synthesis) | Fast (seconds to minutes) |
| Duration | Long-lasting | Short-lived |
| Transportable in blood | Bound to carrier proteins | Dissolved freely |
| Examples | Cortisol, estrogen, testosterone | Insulin, adrenaline, glucagon |
Biological Effects (Examples)
- Glucocorticoids (cortisol): Anti-inflammatory genes upregulated; pro-inflammatory genes (IL-2, TNF-α) downregulated via transrepression.
- Estrogen: Upregulates genes for uterine growth, breast development, LH receptor synthesis.
- Testosterone: Promotes muscle protein synthesis, spermatogenesis genes.
- Aldosterone: Upregulates ENaC (epithelial Na⁺ channel) and Na⁺/K⁺-ATPase genes in kidney tubules.
- Vitamin D (1,25-OH₂D₃): Upregulates calcium-binding proteins in the gut for Ca²⁺ absorption.
Summary Flowchart
Steroid hormone (lipophilic)
↓
Diffuses across plasma membrane
↓
Binds cytoplasmic receptor (displaces Hsp90)
↓
NLS exposed → Receptor dimerizes
↓
Translocates into nucleus via nuclear pore
↓
DBD binds HRE (specific DNA sequence)
↓
TAD recruits coactivators + chromatin remodelers
↓
RNA Pol II basal complex assembled
↓
Gene transcription ↑ or ↓
↓
New mRNA → New proteins → Biological effect
- Basic Medical Biochemistry: A Clinical Approach, 6th Ed, p. 517-518
- Medical Physiology (Boron & Boulpaep), p. 143-144
Enumerate lft , discuss disords associate with it . 1st yr mbbs student
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive, well-sourced content. Here is a complete, 1st year MBBS-friendly answer:
Liver Function Tests (LFTs) - Complete Notes for 1st Year MBBS
What are LFTs?
Liver Function Tests are a battery of blood tests that assess different aspects of liver function - its integrity, excretory ability, synthetic capacity, and metabolism. No single test tells the whole story; the pattern of results together gives the diagnosis.
"The best way to increase sensitivity and specificity is to employ a battery of tests that includes aminotransferases, alkaline phosphatase, bilirubin, albumin, and prothrombin time." - Harrison's Principles of Internal Medicine, 22nd Ed
Classification of LFTs
The liver performs 3 broad functions, and tests are grouped accordingly:
| Category | What it Tests | Tests Used |
|---|---|---|
| Hepatocyte Integrity | Liver cell damage/necrosis | AST, ALT, LDH |
| Biliary Excretory Function | Bile secretion and flow | Bilirubin (total, direct, indirect), ALP, GGT, Urine bilirubin |
| Hepatocyte Synthetic Function | Liver's ability to make proteins | Serum Albumin, PT/INR, Serum Ammonia |
1. TESTS OF HEPATOCYTE INTEGRITY (Cell Damage Tests)
A. Serum Transaminases (Aminotransferases)
Alanine Aminotransferase (ALT) - also called SGPT
- Location: Predominantly in liver cytoplasm (liver-specific)
- Normal: 7-56 U/L
- Rises in: Acute hepatitis, hepatocellular necrosis, drug toxicity
- Key point: ALT is more specific for liver disease than AST because AST is also found in heart and skeletal muscle
Aspartate Aminotransferase (AST) - also called SGOT
- Location: Liver, heart, skeletal muscle, kidney (less specific)
- Normal: 10-40 U/L
- Rises in: Liver disease, MI, muscle injury
- Key ratio - AST:ALT >2:1 strongly suggests alcoholic liver disease or cirrhosis
ALT > AST = viral hepatitis; AST:ALT > 2 = alcoholic hepatitis/cirrhosis
Lactate Dehydrogenase (LDH)
- Non-specific enzyme; rises in hepatic necrosis, hemolysis, malignancy
- Less commonly used now; elevated in space-occupying lesions of liver
2. TESTS OF BILIARY EXCRETORY FUNCTION
A. Serum Bilirubin
Bilirubin is the breakdown product of haemoglobin. It exists in two forms:
| Form | Also Called | Solubility | Rises In |
|---|---|---|---|
| Unconjugated bilirubin | Indirect bilirubin | Insoluble (bound to albumin) | Hemolysis, Gilbert's syndrome, neonatal jaundice |
| Conjugated bilirubin | Direct bilirubin | Water-soluble | Obstructive jaundice, hepatocellular disease |
- Normal total bilirubin: 0.2-1.2 mg/dL
- Jaundice appears clinically when bilirubin >2.5-3 mg/dL
- Urine bilirubin: Only conjugated (direct) bilirubin appears in urine (dark urine in obstructive jaundice); absent in hemolytic jaundice
B. Alkaline Phosphatase (ALP)
- Located on the canalicular surface of hepatocytes
- Normal: 44-147 IU/L
- Rises markedly (>4x normal) in: Obstructive jaundice (stones, tumors blocking bile duct), infiltrative liver disease
- Also raised in: Bone disease (Paget's disease, bone metastases) - if uncertain about source, confirm with GGT or 5'-nucleotidase
C. Gamma-Glutamyl Transferase (GGT)
- Located on the hepatic surface of the canaliculus
- Normal: 9-48 U/L
- Very sensitive marker; rises early in:
- Obstructive jaundice
- Alcoholic liver disease (most sensitive marker for alcohol use)
- Drug-induced liver disease
- Used to confirm liver origin of elevated ALP (bone disease does NOT raise GGT)
3. TESTS OF HEPATOCYTE SYNTHETIC FUNCTION
The liver makes >90% of all plasma proteins. Synthetic function is compromised only when >80% of liver tissue is destroyed (cirrhosis, fulminant failure).
A. Serum Albumin
- Entirely synthesized in the liver
- Normal: 3.5-5.0 g/dL (35-50 g/L)
- Half-life = ~20 days (reflects chronic liver function)
- Low albumin = chronic liver disease (cirrhosis), malnutrition, nephrotic syndrome
- NOT useful in acute liver disease (takes weeks to fall)
B. Prothrombin Time (PT) / INR
- Liver synthesizes coagulation factors II, V, VII, IX, X (all except VIII)
- PT is prolonged when liver cannot make enough clotting factors
- Half-life of Factor VII = ~6 hours → PT reflects acute liver function
- Key clinical point:
- PT prolonged + corrects with Vitamin K = obstructive jaundice (fat-soluble Vitamin K not being absorbed)
- PT prolonged + does NOT correct with Vitamin K = hepatocellular damage (liver can't synthesize factors even with adequate Vitamin K)
C. Serum Ammonia
- Liver converts toxic ammonia to urea via the urea cycle (Krebs-Henseleit cycle)
- Rises only when >80% liver tissue is destroyed
- Elevated ammonia → Hepatic Encephalopathy (confusion, altered consciousness, flapping tremor - asterixis)
- Useful in cirrhosis and fulminant hepatic failure
4. DISORDERS ASSOCIATED WITH LFT PATTERNS
Here is the most important table for exams - the pattern of LFT abnormalities in common liver diseases:
| Disorder | AST/ALT | ALP | Bilirubin | Albumin | PT |
|---|---|---|---|---|---|
| Acute Viral Hepatitis | ↑↑↑ (>500 U/L) ALT>AST | Normal or mildly ↑ | Both fractions ↑ | Normal | Usually normal |
| Alcoholic Hepatitis | ↑ (AST:ALT >2:1) | Normal to mildly ↑ | Both ↑ | ↓ | Prolonged |
| Cirrhosis | Normal or mildly ↑ | Normal | Both ↑ | ↓↓ (low) | Prolonged, doesn't correct with Vit K |
| Obstructive Jaundice | Normal to moderate ↑ | ↑↑↑ (>4x normal) | Direct bilirubin ↑↑ | Normal | Prolonged, corrects with Vit K |
| Liver Metastases/Tumors | Normal to mildly ↑ | ↑↑↑ | Usually normal | Normal | Normal |
| Fulminant Hepatic Failure | ↑↑↑↑ (>10,000 U/L) | ↑ | ↑↑ | ↓↓ | Prolonged |
| Hemolysis/Gilbert's | Normal | Normal | Indirect (unconjugated) ↑ | Normal | Normal |
- Harrison's Principles of Internal Medicine, 22nd Ed, Table 348-1
- Henry's Clinical Diagnosis and Management by Laboratory Methods
Specific Disorder Discussions
1. Acute Viral Hepatitis
- AST and ALT rise markedly (>500 IU/L), days before jaundice appears
- ALT > AST (liver-specific injury)
- <80% liver destroyed → albumin and ammonia remain normal
- Self-limiting; full regeneration occurs
2. Cirrhosis
- Fibrosis replaces hepatocytes → no regeneration → >80% tissue lost
- AST/ALT are normal or mildly elevated (few cells left to lyse)
- Albumin ↓, Ammonia ↑, PT prolonged = signs of failed synthetic function
- Both conjugated + unconjugated bilirubin elevated
3. Obstructive (Cholestatic) Jaundice
- Caused by gallstones, carcinoma of head of pancreas, bile duct stricture
- ALP and GGT rise dramatically (canalicular enzymes backed up)
- Direct bilirubin rises predominantly (conjugated bilirubin cannot be excreted)
- Dark urine (bilirubinuria), pale stools (no stercobilin)
- PT prolonged but corrects with parenteral Vitamin K (absorption problem, not synthesis)
4. Alcoholic Liver Disease
- Classic finding: AST:ALT ratio >2:1
- GGT markedly elevated (most sensitive marker for alcohol use)
- Macrocytosis on CBC is an additional clue
5. Fulminant Hepatic Failure
- Most severe - total liver failure
- AST/ALT >10,000 IU/L + AST disproportionately > ALT
- Albumin markedly low, Ammonia very high → hepatic encephalopathy
- PT markedly prolonged, doesn't correct with Vit K
- Medical emergency → requires liver transplantation
Memory Aid - Quick Summary
LFT Tests grouped by function:
DAMAGE tests (↑ = bad):
AST (SGOT) - less specific
ALT (SGPT) - more specific for liver
LDH
BILE tests (↑ = bad):
Bilirubin (direct/indirect/total)
ALP - obstructive
GGT - obstructive + alcohol
SYNTHETIC tests (↓ = bad):
Albumin (chronic failure)
PT/INR (acute failure)
Ammonia (>80% destruction)
Key rule for exams:
-
High ALT/AST + normal ALP = Hepatocellular disease (hepatitis)
-
High ALP + normal ALT/AST = Cholestatic/Obstructive disease
-
Low albumin + prolonged PT = Chronic liver failure (cirrhosis)
-
Robbins & Kumar Basic Pathology, Table 14.1, p. 596
-
Harper's Illustrated Biochemistry, 32nd Ed, p. 586
-
Harrison's Principles of Internal Medicine, 22nd Ed
Monoclonal antibodies, production, application - 1st yr mbbs student
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have all the content I need including two excellent diagrams. Here is a complete, well-illustrated 1st year MBBS-level answer.
Monoclonal Antibodies - Complete Notes for 1st Year MBBS
What is an Antibody? (Quick Recap)
When the body encounters a foreign substance (antigen), B lymphocytes are activated and differentiate into plasma cells that secrete antibodies. Normally, many different B cell clones respond, each making antibodies against a different part (epitope) of the antigen. These are called polyclonal antibodies - a mixture of different antibodies with different specificities.
| Type | Produced by | Specificity |
|---|---|---|
| Polyclonal antibodies | Many different B cell clones | Recognize multiple epitopes on the same antigen |
| Monoclonal antibodies (mAbs) | A single B cell clone | Recognize only one specific epitope |
Definition of Monoclonal Antibodies
"Monoclonal antibodies are identical antibodies produced by a single clone of cells... the hybridoma is immortal and produces a single (monoclonal) antibody." - Medical Microbiology, 9th Ed
Monoclonal antibodies are:
- Produced by a single clone of identical cells
- All structurally identical to each other
- All binding to the exact same epitope of an antigen
- Produced in unlimited quantities
Historical Background
- 1975 - Köhler and Milstein (Cambridge, UK) developed the hybridoma technique for producing monoclonal antibodies from B-cell hybridomas.
- They were awarded the Nobel Prize in Physiology or Medicine in 1984 for this discovery.
- This technology completely transformed immunology, diagnostics, and therapeutics.
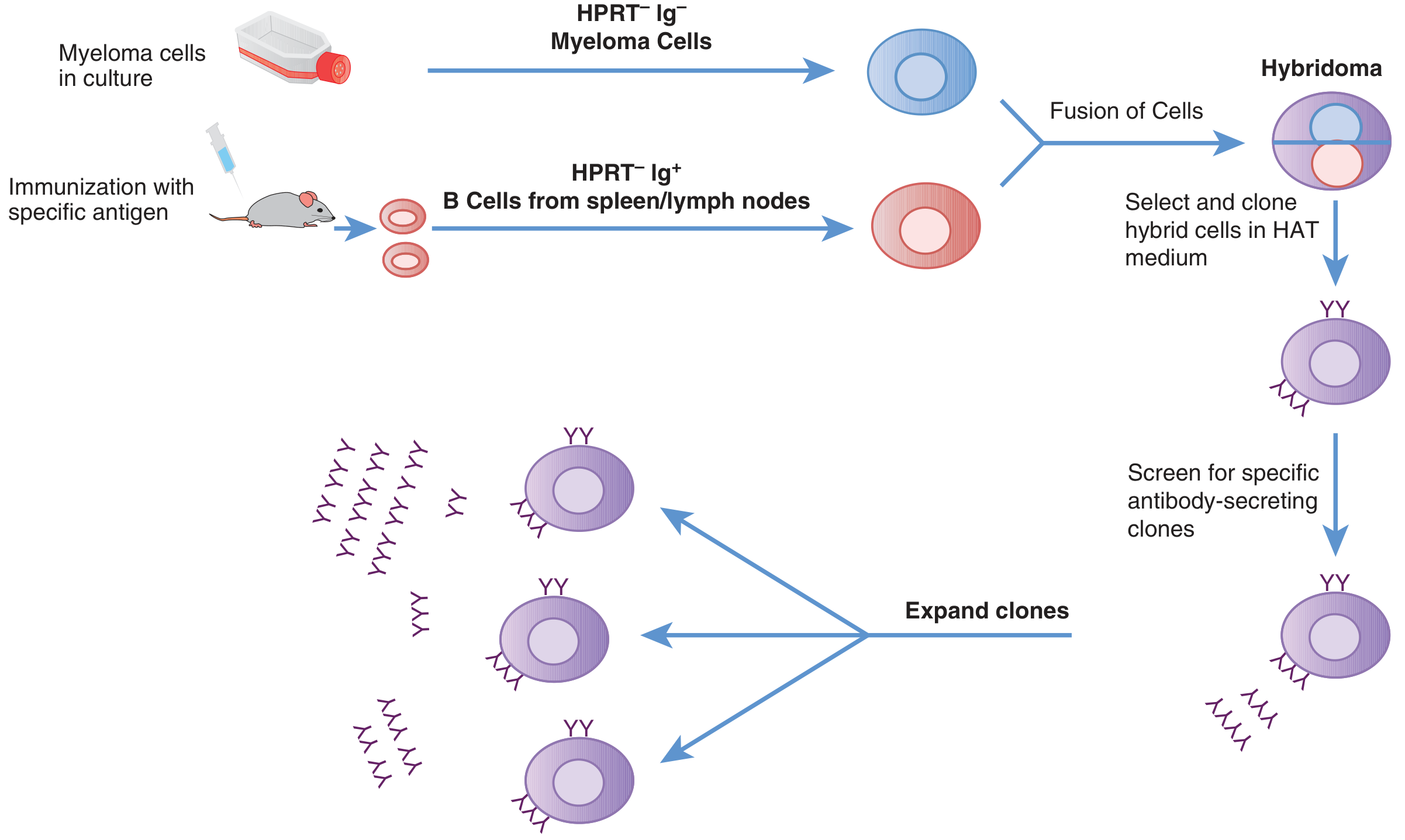
Production of Monoclonal Antibodies - Hybridoma Technology
The central problem to solve: B cells can make specific antibodies, but they die after a few days in culture. Myeloma cells (cancerous plasma cells) are immortal but don't make useful antibodies. The solution: fuse them.
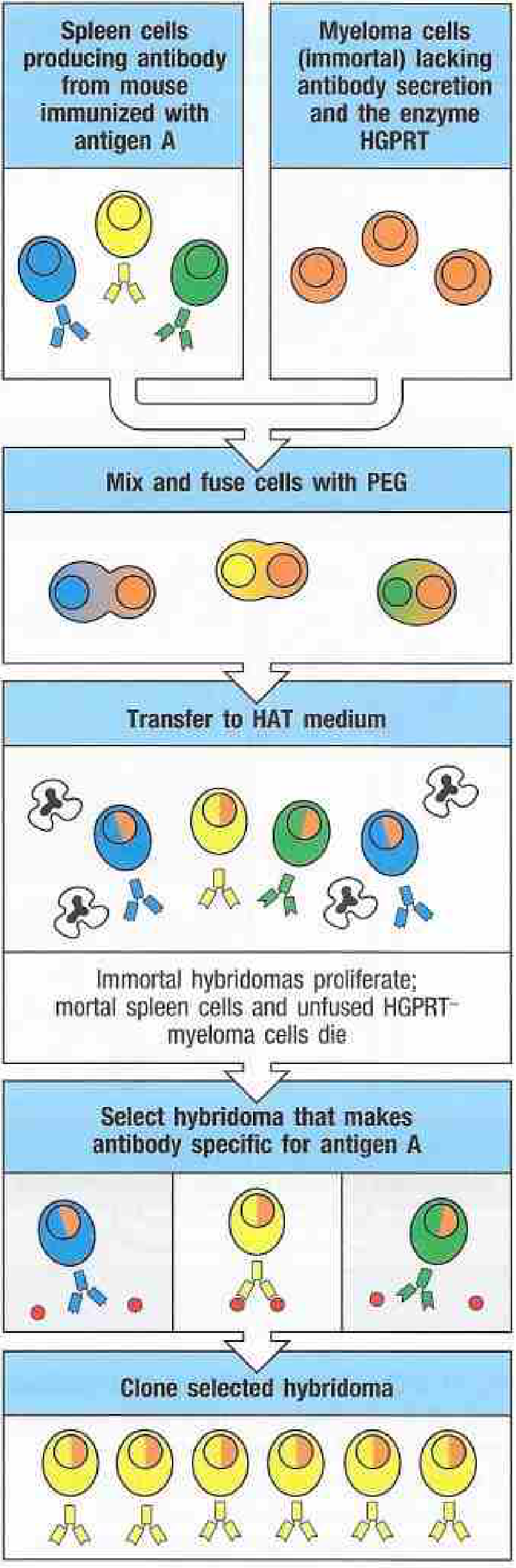
Step-by-Step Production
Step 1 - Immunization of the Mouse
- A mouse (or rat) is injected with the desired antigen (e.g., a tumor protein, viral protein, hormone).
- The mouse mounts an immune response - its B lymphocytes are activated and produce antibodies specific for that antigen.
- A booster injection is given 3 days before sacrifice to maximize antibody-producing cells.
Step 2 - Isolation of Spleen/Lymph Node B Cells
- The mouse is sacrificed.
- The spleen (or lymph nodes) is removed and a suspension of B lymphocytes is prepared.
- These cells produce the desired antibody but will die in culture (mortal cells).
Step 3 - Preparation of Myeloma Cells
- A myeloma cell line (cancerous B cell, immortal) is grown in culture.
- These myeloma cells are specially selected to:
- Not secrete their own antibodies (so they don't contaminate the product)
- Lack the enzyme HGPRT (hypoxanthine-guanine phosphoribosyltransferase) - this is the key to selection (explained below)
Step 4 - Cell Fusion using Polyethylene Glycol (PEG)
- Spleen B cells + Myeloma cells are mixed and fused using polyethylene glycol (PEG), a chemical fusogen that promotes cell membrane merging.
- The fusion produces a mixture of:
- Unfused spleen B cells
- Unfused myeloma cells
- Hybridomas (fused B cell + myeloma cell) - the ones we want
Step 5 - Selection in HAT Medium
- The mixture is transferred to HAT medium (Hypoxanthine + Aminopterin + Thymidine).
- Aminopterin blocks the main DNA synthesis pathway (de novo pathway) in ALL cells.
- Cells can survive only if they use the salvage pathway (using HGPRT enzyme).
| Cell Type | HGPRT | Fate in HAT medium |
|---|---|---|
| Unfused myeloma cells | ❌ Absent | Die (can't use salvage pathway) |
| Unfused spleen B cells | ✅ Present | Die anyway (short lifespan - mortal) |
| Hybridoma cells | ✅ From spleen cell | SURVIVE (immortal + HGPRT from B cell) |
Only hybridomas survive - they have immortality from myeloma + HGPRT from B cells.
Step 6 - Screening and Cloning
- Surviving hybridomas are separated into individual wells (single-cell dilution / limiting dilution).
- Each well is tested (screened) for production of the desired antibody using ELISA or other assays.
- Positive clones are selected and expanded.
Step 7 - Mass Production
- The selected hybridoma clone is grown in bulk tissue culture or injected into the peritoneal cavity of mice (as ascites fluid) to produce large amounts.
- The monoclonal antibody is then purified for use.
Production Diagrams (from Janeway's Immunobiology & Goodman & Gilman's)
Types of Monoclonal Antibodies (Based on Origin)
As mAbs were originally derived from mice, they caused immune reactions (HAMA - Human Anti-Mouse Antibody response) when given to humans. This led to progressively "humanized" versions:
| Type | Description | % Human | Suffix | Example |
|---|---|---|---|---|
| Murine | Fully from mouse | 0% | -omab | Ibritumomab |
| Chimeric | Mouse variable region + Human constant region | ~65% | -ximab | Rituximab, Infliximab |
| Humanized | Only mouse hypervariable loops + rest human | ~95% | -zumab | Trastuzumab, Bevacizumab |
| Fully Human | Entirely human (phage display / transgenic mice) | 100% | -umab | Adalimumab, Pembrolizumab |
The suffix -mab always denotes a monoclonal antibody in drug names.
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Advantages and Disadvantages
| Advantages | Disadvantages |
|---|---|
| Extremely specific - recognize single epitope | Can be too specific (one strain of a virus but not others) |
| Unlimited supply from immortal hybridoma | Expensive to produce |
| Homogeneous (identical molecules) | Mouse-derived mAbs cause immune reactions (HAMA) |
| Can be engineered (chimeric, humanized) | Long development time |
| Can be conjugated with drugs/toxins/radioactive labels | Risk of infection and immunosuppression with therapeutic use |
Applications of Monoclonal Antibodies
1. Diagnostic Applications
| Use | Example |
|---|---|
| Pregnancy tests | Detection of hCG (human chorionic gonadotropin) in urine |
| Blood grouping | Typing ABO and Rh blood groups |
| ELISA assays | Detection of HIV, Hepatitis B/C antigens and antibodies |
| Immunohistochemistry (IHC) | Identifying cancer cell types on biopsy (e.g., ER/PR in breast cancer) |
| Flow cytometry | Counting CD4+ T cells in HIV patients |
| Tumor markers | PSA for prostate cancer, CEA for colorectal cancer |
| Rapid diagnostic tests | COVID-19 antigen tests, Malaria RDTs |
2. Therapeutic Applications
a) Cancer Treatment (most important use today)
| Drug | Target | Used For |
|---|---|---|
| Trastuzumab (Herceptin) | HER2 receptor | HER2+ Breast cancer |
| Rituximab | CD20 on B cells | Non-Hodgkin's lymphoma, B-cell cancers |
| Bevacizumab (Avastin) | VEGF (tumor blood vessel growth) | Colorectal, lung, breast cancer |
| Pembrolizumab (Keytruda) | PD-1 (immune checkpoint) | Melanoma, lung cancer (immunotherapy) |
| Cetuximab | EGFR | Colorectal, head and neck cancer |
Antibody-Drug Conjugates (ADCs): mAbs linked to a cytotoxic drug - the antibody delivers the poison directly to the cancer cell like a "magic bullet."
b) Autoimmune / Inflammatory Diseases
| Drug | Target | Used For |
|---|---|---|
| Infliximab, Adalimumab | TNF-α | Rheumatoid arthritis, Crohn's disease |
| Omalizumab | IgE | Severe allergic asthma |
| Ustekinumab | IL-12/IL-23 | Psoriasis, Crohn's disease |
| Dupilumab | IL-4/IL-13 receptor | Atopic dermatitis, asthma |
c) Transplant Rejection Prevention
- Basiliximab, Daclizumab - target IL-2 receptor on T cells → prevent rejection of transplanted organs
d) Infectious Diseases
- Palivizumab - prevents RSV (Respiratory Syncytial Virus) in premature infants
- COVID-19 neutralizing antibodies - e.g., Sotrovimab
e) Cardiovascular Disease
- Abciximab - targets glycoprotein IIb/IIIa on platelets; prevents clot formation during coronary angioplasty
f) Research Tools
- Used in immunohistochemistry, ELISA, Western blots, flow cytometry - standard tools in all medical research labs
Summary - Key Points for Exam
MONOCLONAL ANTIBODIES
│
├── DEFINITION: Identical antibodies from a single B-cell clone
│ targeting ONE epitope
│
├── PRODUCTION (Hybridoma Technology - Kohler & Milstein, 1975):
│ Mouse immunized → Spleen B cells isolated
│ + Myeloma cells (HGPRT⁻, immortal, no Ab)
│ ↓ Cell fusion with PEG
│ → Hybridoma = immortal + antibody-producing
│ ↓ Selection in HAT medium (kills unfused cells)
│ → Screen for desired antibody → Clone → Mass produce
│
├── TYPES: Murine (-omab) → Chimeric (-ximab)
│ → Humanized (-zumab) → Fully human (-umab)
│
└── APPLICATIONS:
DIAGNOSTIC: Pregnancy tests, ELISA, blood grouping, cancer IHC
THERAPEUTIC: Cancer (Rituximab, Trastuzumab), Autoimmune (Infliximab),
Transplant (Basiliximab), Infection (Palivizumab)
- Medical Microbiology, 9th Ed (Murray)
- Janeway's Immunobiology, 10th Ed
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Histology: A Text and Atlas (Ross & Pawlina)
This is a shared conversation. Sign in to Orris to start your own chat.