Latest guidelines for management of hypertension in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "pregnancy" AND "management"
Searching the Web
hypertension in pregnancy management guidelines 2024 2025 ACOG ISSHP
Reading File
Reading File
Searching PubMed
"hypertensive disorders of pregnancy" AND "guidelines"
Reading File
Reading File
Reading Web Page
https://www.sicardiologia.it/wp-content/uploads/2025/06/arti…
Reading File
Reading File
Loading Image
Reading File
I now have sufficient information from multiple authoritative sources to construct a comprehensive answer. Let me compile:
Management of Hypertension in Pregnancy — Current Guidelines
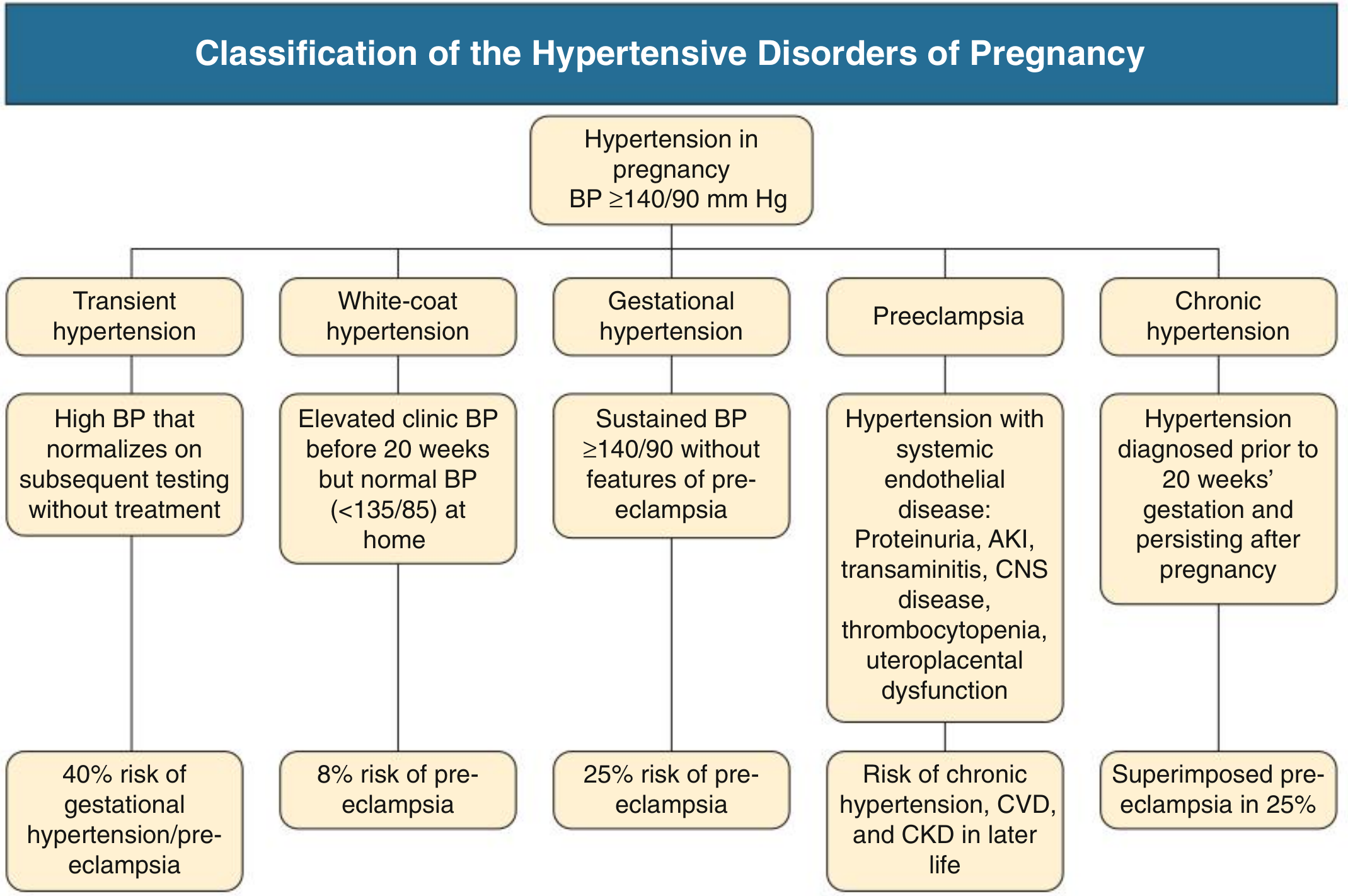
1. Classification
The hypertensive disorders of pregnancy are defined by BP ≥ 140/90 mmHg after 20 weeks and classified as:
| Disorder | Definition | Risk |
|---|---|---|
| Transient hypertension | BP normalises on repeat testing without treatment | 40% risk of gestational HTN/preeclampsia |
| White-coat hypertension | Clinic BP ≥140/90, home BP <135/85 | ~8% risk of preeclampsia |
| Gestational hypertension | New BP ≥140/90 after 20 weeks, no features of preeclampsia | ~25% progress to preeclampsia |
| Preeclampsia | New hypertension + organ dysfunction (see below) | Chronic HTN, CVD, CKD later in life |
| Chronic hypertension | BP ≥140/90 predating pregnancy or before 20 weeks, persisting >12 weeks postpartum | Superimposed preeclampsia in ~25% |
Diagnostic criteria for preeclampsia (ISSHP/ACOG): new hypertension after 20 weeks plus ≥1 of:
- Proteinuria: uPCR >30 mg/mmol, uACR >8 mg/mmol, or >300 mg/24h
- Serum creatinine >90–100 µmol/L or doubling in pregnancy
- Thrombocytopenia, elevated transaminases, pulmonary oedema, CNS symptoms, or uteroplacental dysfunction (fetal growth restriction, abnormal umbilical artery Doppler)
Proteinuria is not essential if other criteria exist. — Comprehensive Clinical Nephrology, 7th Ed.
2. BP Measurement
- Home BP monitoring (HBPM) and 24-hour ABPM should be used to exclude white-coat and masked hypertension, both of which are more prevalent in pregnancy.
- Normal range: nadir ~113/69 mmHg at 18–19 weeks; upper limit 136/86 at mid-pregnancy, rising to 144/95 at term. The threshold of 140/90 mmHg is thus appropriate for defining hypertension throughout pregnancy.
3. BP Targets
| Guideline | Mild-moderate HTN | Target |
|---|---|---|
| 2024 ESC | All chronic + gestational HTN | Below 140/90, but diastolic ≥ 80 mmHg |
| ACOG/ISSHP | Treat at ≥140/90 (chronic); ≥150/95 in low-risk gestational | <140/90 in most |
| ESC 2024 (severe) | SBP ≥170 or DBP ≥110 | Emergency — admit immediately |
The 2024 ESC guidelines (Class I, Level B) state:
"In chronic and gestational hypertension, it is recommended to lower BP below 140/90 mmHg but not below 80 mmHg diastolic."
The landmark CHIPS trial (NEJM 2015) showed less-tight control (target DBP 100 mmHg) versus tight control (DBP 85 mmHg) did not reduce pregnancy loss or NICU admissions, but tight control reduced risk of severe hypertension.
4. Prevention
Aspirin:
- Low-dose aspirin (75–150 mg/day), started before 16 weeks gestation, is recommended for women at high risk of preeclampsia (prior preeclampsia, chronic hypertension, CKD, diabetes, multifetal pregnancy, antiphospholipid syndrome).
Calcium supplementation:
- Calcium 1.5–2 g/day is recommended in women with low calcium intake to reduce the risk of preeclampsia (Cochrane evidence; 2024 NEJM trial also supports low-dose supplementation).
Lifestyle:
- Low-to-moderate intensity exercise is recommended in all pregnant women without contraindications (ESC 2024, Class I, Level B).
5. Antihypertensive Drug Choice
First-line oral agents
| Drug | Notes |
|---|---|
| Labetalol (oral/IV) | Preferred beta-blocker; alpha-blockade preserves uteroplacental flow; multiple daily dosing needed |
| Long-acting nifedipine (CCB) | Once-daily; preferred by 2024 ESC; may cause oedema. Beta-blockers and CCBs are more effective than methyldopa at preventing severe HTN (Cochrane) |
| Methyldopa | Longest safety record; short half-life, sedation; less favoured in newer guidelines |
Second-line oral agents
- Metoprolol (less data than labetalol), verapamil/diltiazem (limited data)
Intravenous agents (for acute/severe HTN)
| Drug | Notes |
|---|---|
| IV Labetalol | First choice; good safety data |
| IV Nicardipine | Extensive data (used as tocolytic); effective |
| Oral nifedipine (fast-release) | Can be used acutely in many settings |
| IV Hydralazine | Widely used but higher risk of maternal hypotension and placental abruption; now second-line |
Drugs to avoid
| Drug | Reason |
|---|---|
| ACE inhibitors | Fetal anomalies, neonatal renal failure, oligohydramnios — contraindicated |
| ARBs (angiotensin receptor blockers) | Same risks as ACEi — contraindicated |
| Atenolol | Associated with fetal growth restriction |
| Nitroprusside | Risk of fetal cyanide toxicity if used >4 hours |
| Diuretics | May impair pregnancy-associated plasma volume expansion (avoid unless pulmonary oedema) |
— Brenner and Rector's The Kidney; 2024 ESC Guidelines for Elevated Blood Pressure
6. Management of Preeclampsia
Seizure prophylaxis:
- Magnesium sulfate (MgSO₄) is the drug of choice for both prevention and treatment of eclampsia. It is superior to phenytoin and diazepam for seizure prevention.
- Dose: IV loading dose 4–6 g over 15–20 min, followed by maintenance infusion 1–2 g/hour.
- Monitor for toxicity: loss of deep tendon reflexes (first sign), respiratory depression. Antidote: calcium gluconate IV.
Definitive treatment:
- Delivery is the only cure. Timing depends on gestational age and severity:
- ≥37 weeks: deliver
- 34–37 weeks with severe features: deliver
- <34 weeks without severe features: expectant management with close monitoring in a tertiary centre
Corticosteroids: Betamethasone (2 doses, 12 mg IM, 24h apart) for fetal lung maturity if delivery anticipated at <34 weeks.
7. Severe/Hypertensive Emergency in Pregnancy
| Threshold | Action (2024 ESC) |
|---|---|
| SBP ≥170 or DBP ≥110 mmHg | Immediate hospitalisation — emergency (Class I, Level C) |
| SBP ≥160 or DBP ≥110 mmHg | Hospital admission should be strongly considered (Class IIa, Level C) |
Goals: reduce SBP to 140–155 mmHg and DBP to 90–105 mmHg (avoid precipitous drops).
8. Postpartum Management
- Hypertension may worsen in the first 3–5 days postpartum (fluid mobilisation).
- NSAIDs should be avoided postpartum in women with hypertension (raise BP, risk of renal impairment).
- Most antihypertensives are compatible with breastfeeding; labetalol and nifedipine are preferred.
- ACE inhibitors (enalapril, captopril) are acceptable postpartum and during breastfeeding.
- Women with hypertensive disorders of pregnancy have a 2-fold increased lifetime risk of CVD and stroke and should receive long-term cardiovascular risk counselling.
9. Secondary Causes to Consider
Investigate in refractory or early-onset severe HTN: renal artery stenosis (fibromuscular dysplasia), pheochromocytoma (can be fatal if missed), primary hyperaldosteronism, OSA (40% of pregnant women with HTN), and rare mineralocorticoid receptor mutations.
Recent Evidence (2023–2025)
| Study/Source | Key finding |
|---|---|
| Wu P et al., BMJ 2023 [PMID 37391211] | Comprehensive review: confirms early aspirin, MgSO₄, and tight BP control as cornerstones |
| Countouris M et al., Circulation 2025 [PMID 39960983] | Highlights postpartum period as underrecognised window for BP escalation and CVD risk reduction |
| 2024 ESC Guidelines | Updated BP targets (Class I, Level B): treat chronic HTN at ≥140/90; target <140/90 but diastolic ≥80 mmHg |
Note: The 2025 Circulation review (PMID 39960983) emphasises that postpartum hypertension management remains an underserved area and a key opportunity to reduce long-term cardiovascular risk in women.
Key take-home points:
- Treat BP ≥140/90 in chronic and gestational hypertension; target <140/90 (ESC 2024)
- First-line drugs: labetalol, nifedipine (preferred over methyldopa by current ESC guidance); avoid ACEi/ARBs
- Aspirin 75–150 mg/day from <16 weeks for high-risk women
- MgSO₄ for eclampsia prevention and treatment
- SBP ≥170 or DBP ≥110 mmHg = obstetric emergency
- Delivery is definitive treatment for preeclampsia; timing guided by gestational age and severity
- Long-term CVD counselling for all women with hypertensive disorders of pregnancy
This is a shared conversation. Sign in to Orris to start your own chat.