Everything about plaster of paris in orthopedics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Plaster of Paris (POP) in orthopedics, drawn from leading textbooks.
Plaster of Paris in Orthopedics
1. History
The use of immobilization for fractures dates to the Fifth Dynasty of Egypt (2498–2345 BCE), when bark was used to splint forearm fractures. Gypsum-based dressings were used in the Ottoman Empire around the 16th century. The modern era of POP in fracture management began in the 1800s:
- Seutin (Belgian surgeon) introduced rigid dressings that could be maintained for longer periods.
- Pirogov (Russia) and Mathijsen (Holland, 1851, Haarlem Military Hospital) introduced POP bandages just prior to the Crimean War — an era when effective fracture treatment had become critical due to Napoleonic-era war injuries.
- In the United States, Sayre, Stimson, and Scudder promoted POP bandages.
- Lorenz Böhler of Vienna was a key proponent, advocating accurate reduction, skintight casts, and intensive physiotherapy.
- Sarmiento later advanced the concept of functional bracing for tibial fractures, permitting early joint mobilization.
- In 1927, hard-coated POP rolls were developed, incorporating a binder to improve adhesion to cloth.
Gradually, POP replaced simple splintage and became the cornerstone of nonoperative fracture management worldwide.
— Rockwood and Green's Fractures in Adults 10th ed., p. 315–316; Pfenninger and Fowler's Procedures for Primary Care, p. 1283
2. Chemistry and Physical Properties
Chemical name: Calcium sulfate hemihydrate (CaSO₄·½H₂O)
How it is made:
Gypsum (calcium sulfate dihydrate) is heated to approximately 128°C, driving off most of the water of crystallization, leaving a fine white powder — Plaster of Paris.
Setting reaction (exothermic):
When water is added, the reaction reverses: POP recrystallizes by incorporating water molecules back into the calcium sulfate dehydrate crystalline lattice. This is an exothermic reaction — heat is produced as the cast hardens.
Physical form: POP is impregnated into strips or rolls of crinoline-type material. The crinoline:
- Facilitates easy application
- Helps maintain proper molding during setting
- Adds structural support to the finished cast/splint
Available in 2-, 3-, 4-, and 6-inch widths and different setting times.
— Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1334; Rosen's Emergency Medicine, p. 1394
3. Advantages and Disadvantages
Advantages of POP over fiberglass
| Feature | POP | Fiberglass |
|---|---|---|
| Cost | Lower | Higher |
| Moldability | Easier | More difficult |
| Shelf life | Long | Shorter |
| Allergenicity | Lower | Higher contact allergy risk |
| Custom fit | Excellent | Good |
Disadvantages of POP
| Feature | POP | Fiberglass |
|---|---|---|
| Weight | Heavier | Lighter |
| Strength | Less | 2–3× stronger per thickness |
| Radiolucency | Less | Better |
| Drying time | Slower (24–72 hr full strength) | Rapid (~20 min) |
| Water resistance | Poor (weakens when wet) | Good |
| Heat generated | More | Less |
— Pfenninger and Fowler's, p. 1284; Rockwood and Green's, p. 321
4. Indications
- Stable, undisplaced, or minimally displaced closed fractures
- Reduced fracture-dislocations requiring immobilization
- Soft tissue injuries: ligament sprains (e.g., grade III ankle sprain), Achilles tendon disruption, tendonitis refractory to other therapy
- Congenital deformities (e.g., correction of clubfoot/talipes equinovarus)
- Postoperative stabilization of vascular, tendon, or nerve repairs
- Acute phase management of unstable fractures (before definitive treatment)
The most common indication in primary care is the stable, nondisplaced, closed fracture of a long bone (radius/ulna, phalanges, metacarpals, metatarsals, malleoli).
— Pfenninger and Fowler's, p. 1284
5. Types of POP Casts and Slabs
Slabs vs. Full Circumferential Casts
- Slabs (back-slabs/half-casts): Applied when post-injury swelling is anticipated. Safer acutely as they allow expansion. Secured with bandages.
- Full casts: More effective immobilization; applied once swelling has subsided.
Upper Limb
| Cast | Application | Indications |
|---|---|---|
| Long arm cast | Below axilla → proximal to MCP joints; elbow 90°, wrist 30° dorsiflexion | Forearm/elbow fractures, pediatric fractures, elderly elbow fractures |
| Hanging cast / U-slab | Over lower chest, elbow 90°; gravity reduces humeral fracture | Humeral diaphyseal fractures (acute phase) |
| Colles (forearm) cast | Below elbow → proximal to metacarpal necks; thumb free | Distal radius/ulna fractures, carpal injuries — the most widely used upper limb cast |
| Scaphoid cast | Below elbow → proximal to metacarpal necks; thumb to proximal IP joint; wrist slightly dorsiflexed | Scaphoid fractures, suspected scaphoid injury |
| Burkhalter cast | Combination forearm cast + dorsal slab | Proximal phalanx fractures |
| James cast | Wrist 40° dorsiflexion, MCP 70–90° flexion, IP joints in full extension | Hand fractures (prevents collateral ligament contracture) |
| Bruner cast | Extended scaphoid variant, wrist released | Ligamentous injuries of thumb MCP |
| Shoulder spica | Rare now | Formerly used for clavicle/proximal humeral fractures |
Lower Limb
| Cast | Application | Indications |
|---|---|---|
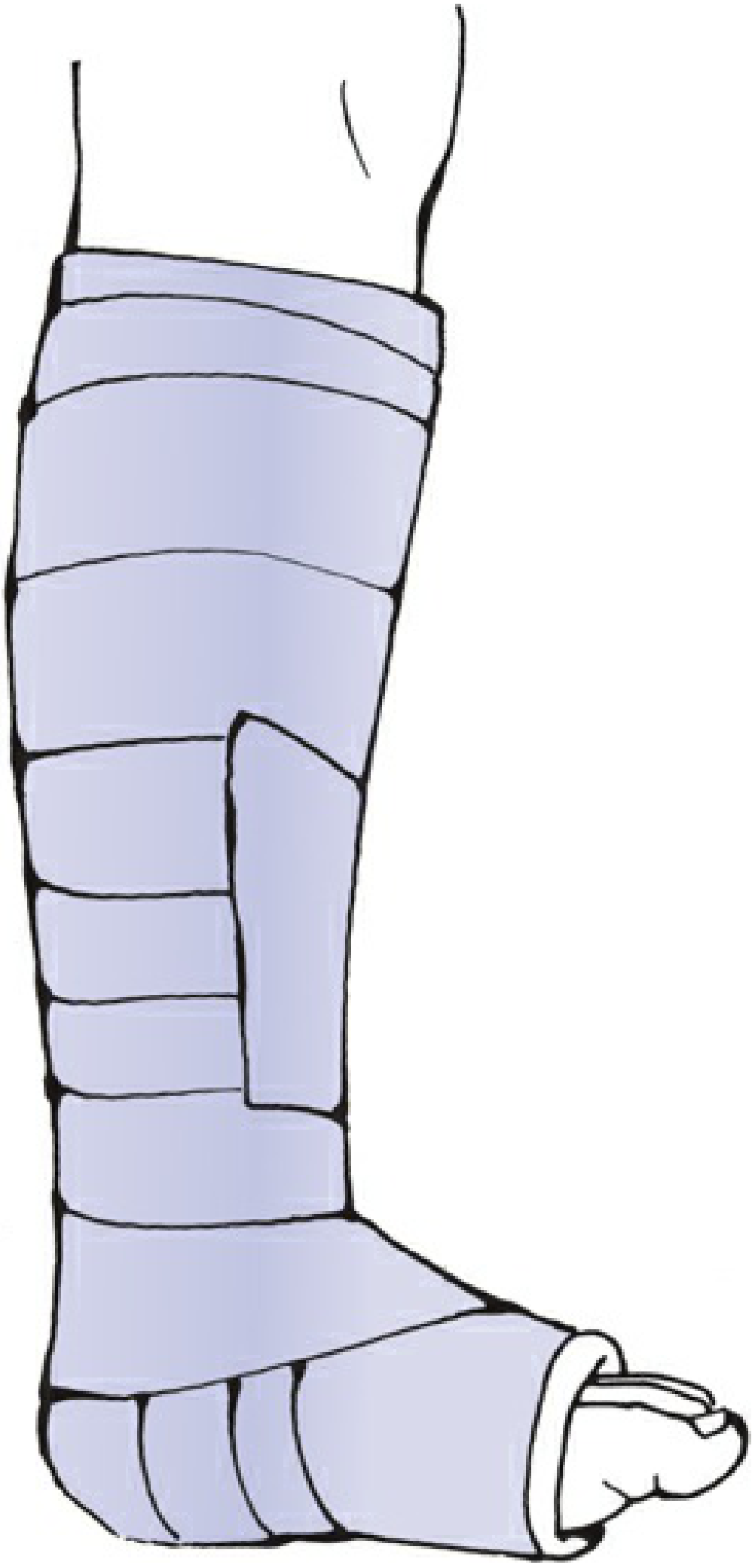
| Below-knee (BK) cast | Below fibular neck → metatarsal heads; ankle 90°, plantigrade | Ankle/foot fractures, soft tissue injuries, undisplaced lower tibial fractures |
| Long-leg cast | BK cast + thigh extension; knee ~10° flexion | Unstable tibial diaphyseal fractures (acute phase) |
| Patellar tendon-bearing (PTB) cast | BK variant with weight-bearing allowed | Tibial fractures after initial swelling subsides |
| Spinal cast / plaster jacket | Sternal notch → symphysis pubis | Spinal fractures (now rarely used; braces preferred) |

— Rockwood and Green's Fractures in Adults 10th ed., pp. 329–337
6. Equipment Required
- Rubber gloves, gown, shoe covers, draping
- Stockinette (2-, 3-, 4-inch widths)
- Cast padding/wool (felt, soft cotton Webril, or synthetic polyester bandages)
- POP rolls/slabs (avoid >10 ply to prevent thermal injury)
- Water source (with plaster trap in drain; water temperature <24°C/75°F)
- Elastic (Ace) bandages
- Cast spreader, cast saw, cast cutter
- Scissors, slings, Chinese finger traps, leg stand
— Pfenninger and Fowler's, p. 1283–1284
7. Application Technique (Step-by-Step)
- Reduce the fracture (if displaced); assistant holds position.
- Measure and apply stockinette — should extend ~10 cm beyond proposed cast ends.
- Apply wool/cast padding distal → proximal, 50% overlap between turns.
- Protect bony prominences with extra padding (malleoli, fibular head, olecranon, radial styloid).
- Submerge POP in water, then squeeze to remove excess water.
- If swelling anticipated → use a slab; apply, mold, then bandage.
- If full cast → apply POP bandages in circumferential layers.
- Hold fracture in reduced position until cast hardens; mold as appropriate.
- Fold stockinette and wool padding back; apply second cast bandage to seal.
- Ensure proximal and distal joints can mobilize adequately.
- Cut the cast if swelling is present or anticipated.
- Obtain post-application radiographs to confirm position.
- Warn the patient about potential complications.
— Rockwood and Green's, Table 10-4, p. 329
8. Thermal Considerations
The setting of POP is exothermic. Factors that increase skin temperature and risk of thermal burns:
- Water temperature >24°C (75°F)
- Cast thickness >8–10 sheets/plies
- Inadequate ventilation of the newly applied cast
- Immersing plaster for too short a time or squeezing out too much water (incomplete hydration → more heat generated)
- Resting the wet cast on an impermeable surface (e.g., rubber pillow) during setting
Rule: Use lukewarm water, apply ≤10 plies, ensure ventilation, and rest cast on breathable material while setting.
— Rosen's Emergency Medicine, p. 1394; Roberts and Hedges', p. 1334; Pfenninger and Fowler's, p. 1284
9. Cast Wedging (Correcting Malunion Within the Cast)
In diaphyseal fractures, angular malalignment can be corrected by wedging:
- Radiographs or fluoroscopy identify fracture site and direction of deformity.
- Cast is cut at the fracture level, leaving a hinge of 2–3 cm intact (hinge position depends on direction of correction).
- Example: Valgus fracture → medial hinge left intact → varus force applied to distal cast to open the window.
- A wooden wedge or doweling is inserted to maintain position while supplementary POP is applied.
- Rotational deformity: cast is cut at the fracture level, rotation corrected — though position is difficult to maintain and reapplication is sometimes preferable.
— Rockwood and Green's, p. 330, Fig. 10-12
10. Complications
| Complication | Mechanism / Notes |
|---|---|
| Compartment syndrome | Most serious. Rising intracompartmental pressure from swelling within a rigid cast. Highest risk in first 24 hours post-injury. |
| Thermal burn | Exothermic setting reaction, especially with thick casts, warm water, or poor ventilation |
| Pressure sores | Bony prominences inadequately padded; migrating padding |
| Plaster blisters | Skin reaction from contact |
| Allergic dermatitis | Contact allergy (benzalkonium chloride in POP formulations is a known allergen) |
| Bacterial/fungal infection | Especially if a wound exists under the casted area |
| Plaster sores (skin breakdown) | From tight or improperly molded casts |
| Peripheral nerve injury | Pressure neuropathy from tight cast |
| Muscle wasting/joint stiffness | Consequence of prolonged immobilization |
| Fracture redisplacement | Secondary displacement within the cast (especially unstable fractures) |
Management of a tight/symptomatic cast
When a patient presents with pain, swelling, distal coolness, or numbness:
Bivalve the cast — cut the cast and padding on each side, remove half the cast at a time, using the other half as a mold to keep the extremity immobile. The bivalved cast can then be held together with bias-cut stockinette or elastic bandaging.
A window may also be placed in the cast for access to wounds requiring observation or dressing changes.
— Rosen's Emergency Medicine, pp. 1394–1396; Rockwood and Green's, p. 329
11. POP vs. Fiberglass: Summary
| POP | Fiberglass | |
|---|---|---|
| Cost | Lower | Higher (gap narrowing) |
| Moldability | Superior | More difficult |
| Weight | Heavier | Lighter |
| Strength | Less | ~2–3× stronger |
| Radiolucency | Poorer | Better |
| Setting time | Longer | ~3 min to set; ~20 min to cure |
| Water resistance | Poor | Good |
| Heat generation | More | Less |
| Allergenicity | Lower | Higher |
| Common use | Resource-limited settings, initial slab, situations requiring precision molding | Now the more frequently used casting material in high-income settings |
POP casts remain widespread globally — inexpensive, easily applied, and well suited to initial/acute-phase immobilization.
— Rockwood and Green's, p. 321
12. Special Notes
- COVID-19 pandemic experience: There was a documented return to nonoperative/POP management during lockdowns, including for distal radius fractures, with generally acceptable outcomes — demonstrating the continued relevance of POP.
- Padding and fracture stability trade-off: Too much padding allows secondary displacement; too little increases compartment syndrome/skin risk. Two layers of wool with 50% overlap is the accepted standard.
- Skin care instruction to patients: Keep cast dry; do not insert objects under the cast; seek review urgently for pain, tingling, swelling, or color change of digits.
- Sink trap required: Plaster waste must not enter drains without a trap — it hardens and blocks plumbing.
— Rockwood and Green's, pp. 328–330; Pfenninger and Fowler's, p. 1284
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed., 2025 — Chapter 10: Nonoperative Fracture Management
- Roberts and Hedges' Clinical Procedures in Emergency Medicine — Chapter 50: Splinting
- Rosen's Emergency Medicine: Concepts and Clinical Practice — Chapter 41: Orthopedic Procedures
- Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. — Chapter 187: Cast Application
- Gray's Anatomy for Students — Bone fractures
This is a shared conversation. Sign in to Orris to start your own chat.