Mesenteric cyst short information
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a concise overview of mesenteric cysts based on authoritative surgical textbooks:
Mesenteric Cyst
Definition & Incidence
Rare benign intra-abdominal lesions arising within the mesentery. Incidence: 1 in 27,000 to 1 in 250,000 hospital admissions. Occur in both children and adults.
Classification / Types
| Type | Features |
|---|---|
| Chylolymphatic (most common) | Arise from congenitally misplaced lymphatics with no efferent connection; mostly in ileal mesentery; thin wall lined by flat endothelium; filled with clear lymph or chyle |
| Enterogenous | Derived from sequestrated intestinal diverticulum or gut duplication; thick wall lined by mucous membrane; content is mucinous |
| Traumatic | Post-injury origin |
| Hydatid | Parasitic origin |
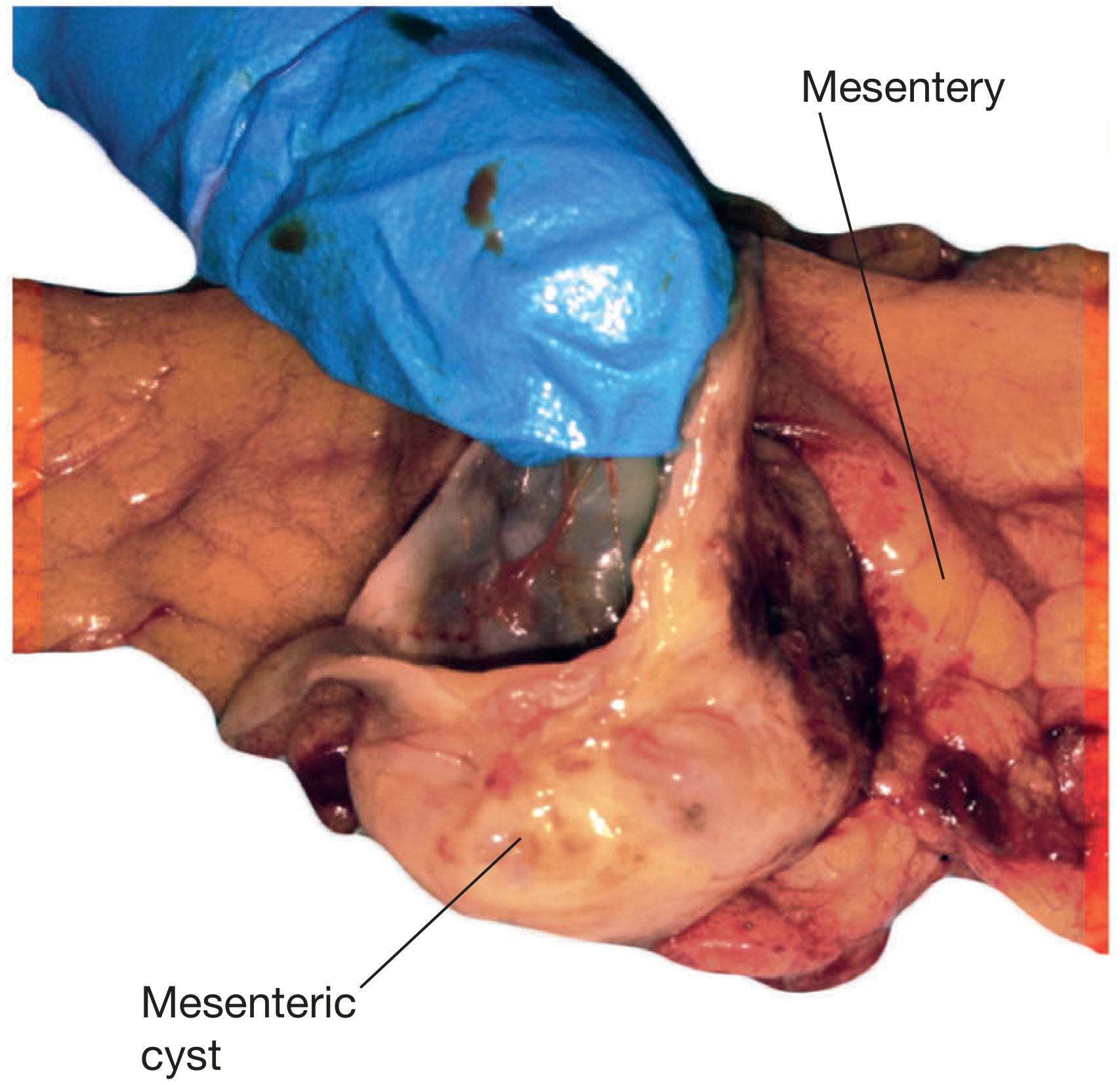
Pathology
- Usually unilocular; may be multilocular
- Lined by a single layer of columnar (or flat endothelial) cells
- Typically large (average ~13 cm, ~2000 mL fluid)
- Up to 3% contain malignancy (usually sarcomatous); solid components raise malignancy risk
- Thought to arise from disrupted/obstructed lymphatics or congenital lymphatic malformations
Clinical Features
- Up to 45% found incidentally on imaging
- Chronic symptoms (nonspecific): abdominal pain/discomfort, anorexia, distension, nausea, vomiting, altered bowel habits
- Acute presentation: cyst rupture, bowel torsion, obstruction
- Most common symptom: pain (58%); most common sign: abdominal distension (68%)
- Abdominal mass detected on exam in up to 60% of patients
Classic Sign
Tillaux's sign: the mass is mobile only laterally (perpendicular to the root of the mesentery), unlike omental cysts which are freely mobile in all directions.
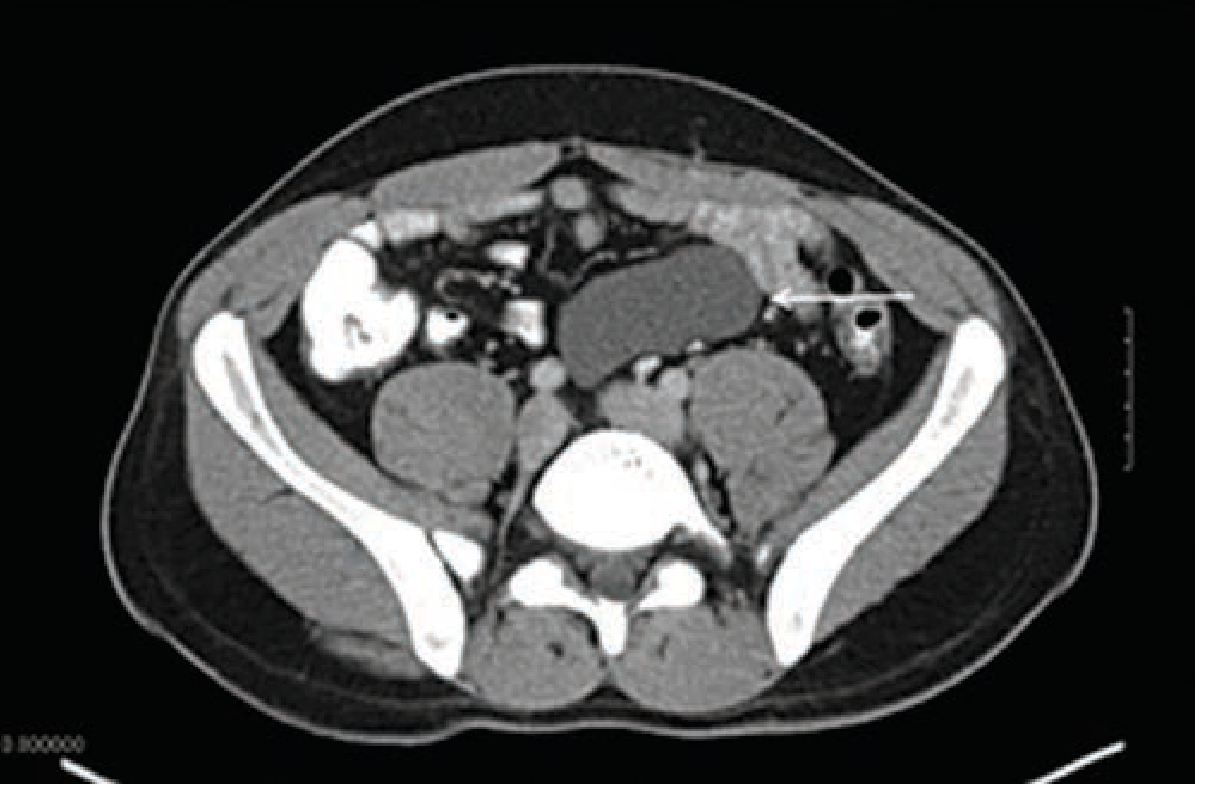
Diagnosis
- CT scan and ultrasound are the primary imaging modalities
- Appear as a homogeneous, fluid-filled mass without solid components in the mesentery
- Mesenteric cystic lymphangioma may appear as multiple cysts on imaging
Treatment
- Complete surgical excision (enucleation for benign; resection with clear margins for malignant)
- Can be performed laparoscopically or open
- Marsupialisation and simple aspiration have high recurrence rates — generally discouraged
- Chylolymphatic cysts: independent blood supply from adjacent bowel → enucleation possible without gut resection
- Enterogenous/duplication cysts: share blood supply with bowel wall → bowel resection and anastomosis required
- Small incidentally found cysts at laparotomy do not require resection unless complicated
- Usually cured by complete excision
Sources: Schwartz's Principles of Surgery 11e; Bailey & Love's Short Practice of Surgery 28e; Sleisenger & Fordtran's GI and Liver Disease
Upper gi hemorrhage classification, type,cause,sign symptoms, investigation management in short for mbbs neet pg students
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information. Let me compile a complete, exam-oriented answer.
Upper GI Hemorrhage — MBBS / NEET PG Quick Reference
Definition
Bleeding proximal to the ligament of Treitz (esophagus, stomach, duodenum).
- Annual hospitalization: ~300,000/year (USA)
- Mortality: 3.5–7%
Classification
By Aetiology
| Type | Examples |
|---|---|
| Variceal | Oesophageal/gastric varices (portal HTN) |
| Non-variceal | Peptic ulcer, Mallory-Weiss tear, erosions, tumors, Dieulafoy, angiodysplasia |
By Onset
- Acute (overt, haemodynamically significant)
- Chronic (occult — iron deficiency anaemia, +ve FOBT)
Causes (with Frequency)
| Cause | % |
|---|---|
| Peptic ulcer (gastric/duodenal) ← MC cause | 38–40% |
| Gastric/oesophageal varices | 16% |
| Erosive oesophagitis | 13% |
| Upper GI tumours | 7% |
| Angiodysplasia / angiomas | 6% |
| Mallory-Weiss tear | 4% |
| Gastric/duodenal erosions | 4% |
| Dieulafoy lesion | 2% |
| Others (aortoenteric fistula, haemobilia, Cameron ulcer) | 2% |
Mnemonic: PEPTIC VAGUE — Peptic ulcer, Erosions, Portal hypertension (varices), Tumours, Inflammation (esophagitis), Cancer, Vascular (Dieulafoy, AVM), Aortoenteric, G-W tear, Ulcer (Cameron), etc.
Signs & Symptoms
Presenting Features
| Symptom | Details |
|---|---|
| Haematemesis | Vomiting fresh blood (active bleeding) or coffee-ground material (digested blood) |
| Melaena | Black, tarry, foul-smelling stool — blood digested in upper GI; ~50–80 mL blood needed |
| Haematochezia | Fresh rectal blood — usually lower GI, but ~15% can be from upper GI source (massive bleed) |
~50% present with haematemesis + melaena; ~30% haematemesis alone; ~20% melaena alone
Symptoms of Hypovolaemia
- Dizziness, syncope, thirst
- Cold clammy skin, pallor
- Oliguria
Signs on Examination
| System | Findings |
|---|---|
| Vitals | Tachycardia, hypotension, orthostasis |
| Skin | Pallor, spider naevi, palmar erythema, petechiae, purpura |
| Abdomen | Ascites, hepatosplenomegaly (portal HTN), epigastric tenderness |
| Rectal | Black/tarry stool on DRE |
Risk Stratification Scores ⭐ (High-yield for NEET PG)
1. Glasgow-Blatchford Score (GBS) — Pre-endoscopy, triage
Used at admission to identify low-risk patients (score 0–1 = safe for outpatient management).
| Parameter | Points |
|---|---|
| BUN ≥18.2 mg/dL | 2–6 |
| Hb <13 (men) / <12 (women) | 1–6 |
| SBP <110 mmHg | 1–3 |
| Pulse ≥100/min | 1 |
| Melaena | 1 |
| Syncope | 2 |
| Hepatic disease | 2 |
| Cardiac failure | 2 |
2. Rockall Score — Post-endoscopy, predicts rebleeding & mortality
| Variable | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Age | <60 | 60-79 | ≥80 | — |
| Shock | No | Pulse>100 | SBP<100 | — |
| Comorbidity | None | — | Cardiac/other | Renal/liver/cancer |
| Diagnosis | MW tear/no lesion | All other | GI malignancy | — |
| Stigmata | None/dark spot | — | Blood/clot/vessel | — |
Score ≤2 = low risk; ≥8 = high mortality
3. Forrest Classification — Endoscopic stigmata of peptic ulcer bleeding
| Class | Finding | Rebleed Risk |
|---|---|---|
| Ia | Active arterial (spurting) | 90% |
| Ib | Active oozing | 50% |
| IIa | Visible vessel (non-bleeding) | 50% |
| IIb | Adherent clot | 25–30% |
| IIc | Flat pigmented spot | 7–10% |
| III | Clean base | <5% |
Endoscopic treatment indicated for Ia, Ib, IIa (and IIb - clot removal + treatment)
Investigations
Immediate
- CBC: Hb, Hct (may not reflect acute loss for 24–72 hrs), platelet count
- BUN/Creatinine: BUN rises disproportionately (blood protein breakdown) → BUN:Cr ratio >20 suggests upper GI source
- LFT + coagulation (PT/INR, aPTT) — assess liver disease
- Blood group & cross-match — prepare packed RBCs
- Vital signs + urine output monitoring
Diagnostic
| Investigation | Purpose |
|---|---|
| Upper GI Endoscopy (OGD) ← Gold standard | Identifies source, provides therapy; within 12–24 hours |
| CT angiography | If endoscopy non-diagnostic or fails; detects bleeding rate ≥0.3–0.5 mL/min |
| Mesenteric angiography | If active bleeding; therapeutic embolisation possible |
| Radionuclide scan (Tc-99m RBC) | Detects slow bleeding ≥0.1 mL/min |
Management
Step 1: Resuscitation (ABC)
- 2 large-bore IV lines (14–16 G)
- Normal saline bolus to maintain haemodynamic stability
- Blood transfusion: give pRBCs if Hb <7 g/dL (restrictive strategy); target Hb 7–9 g/dL
- Exception: Hb target 9–10 g/dL in cardiovascular disease or haemodynamic instability
- Platelets if <50,000/μL with active bleeding
- Consider endotracheal intubation if altered sensorium or active haematemesis (aspiration risk)
Step 2: Pharmacotherapy
| Drug | Use |
|---|---|
| IV PPI (omeprazole/pantoprazole) | Non-variceal bleed — high-dose (80 mg bolus + 8 mg/hr infusion); reduces rebleed |
| IV Octreotide/Somatostatin | Variceal bleed — decreases portal pressure |
| Terlipressin | Variceal bleed (reduces portal HTN) |
| IV Erythromycin 250 mg (30–60 min pre-endoscopy) | Prokinetic — clears stomach blood, improves endoscopic view |
| Antibiotic prophylaxis (ceftriaxone) | Cirrhotic patients with variceal bleed |
Step 3: Endoscopic Therapy (within 12–24 hrs)
- Non-variceal: Adrenaline injection + coagulation (heater probe/APC/clips)
- Variceal: Band ligation (oesophageal) or cyanoacrylate injection (gastric varices)
- Balloon tamponade (Sengstaken-Blakemore tube): temporary bridge in uncontrolled variceal bleed
Step 4: Radiological Interventions
- Angiographic embolisation — if endoscopy fails
- TIPS (Transjugular Intrahepatic Portosystemic Shunt) — refractory variceal bleed
Step 5: Surgery (last resort)
- Indications: failed endoscopy + radiology, exsanguinating haemorrhage
- Procedures: oversewing of ulcer, gastric resection, devascularisation
- Malignant lesions → appropriate surgical resection
Key Exam Points 🎯
| Fact | Value |
|---|---|
| MC cause of UGIB | Peptic ulcer (38–40%) |
| Minimum blood for melaena | ~50–80 mL |
| Gold standard investigation | Upper GI endoscopy (OGD) |
| Pre-endoscopy scoring | Glasgow-Blatchford Score |
| Post-endoscopy scoring | Rockall Score |
| Forrest Ia (spurting) rebleed risk | ~90% |
| Transfusion trigger (restrictive) | Hb <7 g/dL |
| Pre-endoscopy prokinetic | IV Erythromycin 250 mg |
| Variceal bleed drug | Octreotide / Terlipressin |
| Balloon tube for varices | Sengstaken-Blakemore tube |
Sources: Goldman-Cecil Medicine 2e; Schwartz's Principles of Surgery 11e; Bailey & Love's 28e
This is a shared conversation. Sign in to Orris to start your own chat.