Total thyroidectomy -with emphasis on proper positioning
Reading File
Finding Sources
Searching the Web
total thyroidectomy surgical technique patient positioning neck extension
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative surgical textbooks. Let me compile the full response.
Total Thyroidectomy - Complete Surgical Guide (with Emphasis on Positioning)
Overview
Total thyroidectomy involves excision of all visible thyroid tissue. It is distinguished from near-total thyroidectomy (< 1 g left at the ligament of Berry) and thyroid lobectomy (hemithyroidectomy). Over 130,000 thyroidectomies are performed annually in the United States. The fundamental open technique has changed little in decades; energy-sealing devices have reduced operative time but not altered the broad steps. - Sabiston Textbook of Surgery, p. 1522
Indications
- Hyperthyroidism unresponsive to or not preferred for medical management
- Symptomatic goiter (compressive symptoms - dysphagia, stridor, venous obstruction)
- Thyroid nodules and thyroid cancer (differentiated thyroid carcinoma, medullary, Hurthle cell)
Preoperative Preparation
- Biochemical thyroid function assessment
- Neck ultrasound (mandatory)
- FNA biopsy of nodules as indicated
- For hyperthyroid patients: render euthyroid first with antithyroid drugs (propylthiouracil/methimazole), Lugol's iodine solution (reduces vascularity), beta-blockers
- Vocal cord evaluation: noninvasive voice assessment in all; formal laryngoscopy if voice abnormality, prior neck surgery, or posterior extrathyroidal extension present (AAES guideline)
- CT of neck for substernal extension (avoid contrast if RAI will be needed postoperatively)
- Intraoperative neuromonitoring (IONM) tube placement if planned: silicone reinforced ETT with surface/embedded electrodes in contact with vocal cords; muscle relaxation is contraindicated if IONM is used
Anesthesia
General endotracheal anesthesia is standard. If IONM is planned, a specialized neuromonitoring ETT (e.g., NIM EMG tube) is used. A laryngeal mask with spontaneous breathing has been described as an alternative allowing real-time vocal cord endoscopy, but risk of mask displacement is significant. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 1063
⭐ POSITIONING - Key Details
Proper positioning is one of the most critical determinants of exposure, surgical field quality, and postoperative comfort.
Standard Position: Supine with Neck Extension (Rose Position)
| Element | Technique | Rationale |
|---|---|---|
| Body | Supine, both arms tucked at sides | Prevents inadvertent movement; arms tucked away from surgeon's field |
| Back/torso | Raised 20 degrees (reverse Trendelenburg or back elevated) | Improves venous drainage, reduces venous engorgement in the neck |
| Shoulder roll | Soft roll placed behind the scapulae (NOT under the neck directly) | Extends the neck by elevating the upper chest, bringing the thyroid into an anterior/superior position - especially helpful in substernal goiters |
| Head | Rests on a foam or gel ring ("donut" head ring) | Prevents free rotation, supports the head, prevents cervical strain and postoperative posterior neck pain |
| Neck extension | Moderate - avoid hyperextension | Extends the neck to open the surgical field; hyperextension causes postoperative neck pain, may impair arterial/venous outflow, and risks cervical spine injury in elderly patients |
Sabiston Textbook of Surgery, p. 1523 | Current Surgical Therapy 14e, p. 899
Key Positioning Points
"The head is well supported to prevent neck hyperextension and postoperative posterior neck pain."
- The back is raised 20 degrees - this is a semi-recumbent "beach chair" modification of supine
- The shoulder roll should sit at the level of the acromion process / scapulae, NOT under the neck itself
- This elevates the chest and creates neck extension without placing pressure directly on cervical vertebrae
- The net effect: the thyroid moves anteriorly and superiorly, particularly useful in substernal goiters
- The reverse Trendelenburg component (elevated head-of-bed) reduces venous pressure in the neck, minimizing ooze
Excessive extension - problems:
- Postoperative discomfort and posterior neck pain
- May impair arterial and venous outflow to the neck (2025 PMC evidence)
- Risk of brachial plexus stretch injury if shoulders are pulled back too far
- Cervical spine injury risk in patients with cervical spondylosis or limited mobility
Inadequate extension - problems:
- Crowds the surgical field
- Reduces working space between the chin and sternum
- Makes incision placement difficult, especially in patients with short necks or large habitus
Special Populations
| Population | Modification |
|---|---|
| Elderly / cervical spondylosis | Minimal extension; careful padding; beach chair position |
| Substernal goiter | Maximize extension + raise back fully; ensures superior migration of gland |
| Short neck / obese | Greater extension needed; consider slightly superior incision placement |
| Large breasted females | Mark incision before extending neck - extension shifts skin caudally, and pre-extension marking prevents scar migration toward the clavicles |
Incision marking tip (Iowa Protocol): Mark the planned collar incision before applying the shoulder roll and extending the neck. Extending the neck after marking can cause the incision line to migrate toward or below the clavicles, resulting in a stretched, inferior scar.
Surgical Anatomy (Key Structures at Risk)
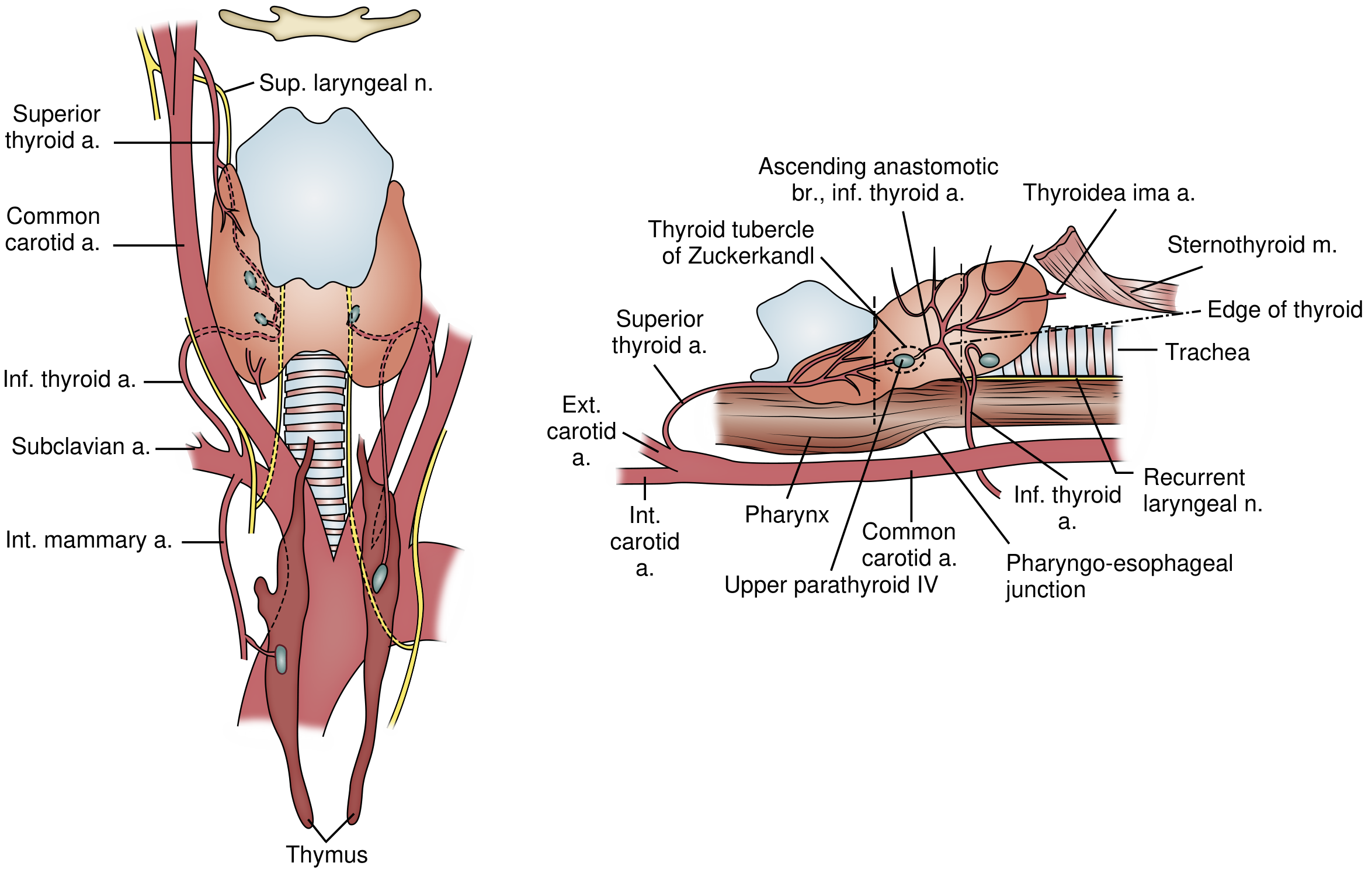
Parathyroid anatomy relative to the RLN and thyroid gland - Current Surgical Therapy 14e
Layer-by-Layer (superficial to deep)
- Dermis
- Platysma
- Sternohyoid muscle + superior belly of omohyoid
- Sternothyroid muscle
- Pretracheal fascia
- Thyroid gland
Critical Nerves
- Recurrent Laryngeal Nerve (RLN): Left loops around aortic arch, ascends in tracheoesophageal groove; right loops around subclavian artery, more oblique/lateral course. Three highest-risk injury zones: (1) posterior to inferior pole, (2) at the inferior thyroid artery crossing, (3) behind the ligament of Berry.
- External Branch of Superior Laryngeal Nerve (EBSLN): Innervates cricothyroid; controls high-pitch voice projection. Crosses the superior thyroid artery in a cephalad-to-caudad trajectory. Classified by Cernea: Type 1 crosses >1 cm above superior pole; Type 2A within 1 cm; Type 2B below the superior border (highest injury risk).
- Non-recurrent inferior laryngeal nerve: ~0.5% prevalence; associated with aberrant right subclavian artery (retro-esophageal). Lies in near-transverse course behind the thyroid. Confirm with preoperative ultrasound/CT.
Parathyroid Glands
- Superior glands: posterior to RLN plane; ~2-5 mm from nerve; more predictable
- Inferior glands: anterior to RLN plane; ~7-10 mm from nerve; more variable
- Ectopic in 15% (retroesophageal, intrathyroidal, carotid sheath, thyro-thymic ligament, mediastinum)
- Up to 25% of superior parathyroids derive blood supply from the superior thyroid artery - ligate this artery close to the gland surface, not proximally
Step-by-Step Technique (Open Total Thyroidectomy)
1. Incision
- Transverse collar incision in a Langer's skin crease or existing neck skin line
- Typically 2-3 cm above the clavicular heads (Current Surgical Therapy) or 1 fingerbreadth above the clavicles
- Length 4-5 cm, scaled to gland size and body habitus
- Mark before neck extension
- Carry incision through platysma
2. Subplatysmal Flaps
- Raise flaps: inferiorly to clavicular heads, superiorly to thyroid cartilage
- Identify anterior jugular veins (between platysma and strap muscles) - suture ligate if needed
3. Strap Muscle Division and Thyroid Exposure
- Incise the superficial layer of deep cervical fascia in the midline from sternal notch to thyroid cartilage
- Separate sternohyoid from sternothyroid by blunt dissection
- Retract strap muscles laterally off the thyroid capsule
- For large/firm glands: transect sternothyroid high (near insertion into thyroid cartilage, as ansa cervicalis innervation enters inferiorly)
- Expose and ligate the middle thyroid vein between thyroid and internal jugular vein (IJV)
4. Superior Pole Dissection (EBSLN Preservation)
- Develop the space of Reeve (avascular cricothyroid space) between superior pole and cricothyroid muscle
- Apply downward/lateral countertraction on the thyroid lobe
- Individually isolate, ligate, and divide superior pole vessels close to the thyroid surface to protect the EBSLN
- IONM can assist EBSLN identification
5. Inferior Pole and Medial Rotation
- Mobilize inferior pole; identify inferior parathyroids
- Ligate inferior thyroid veins
- Medially rotate the thyroid lobe to expose the posterior surface
6. RLN Identification and Preservation
- Spread perpendicular to the nerve axis through fatty/nodal tissue posterior to the thyroid
- Most common: nerve lies deep to inferior thyroid artery (also found anterior to or between branches)
- Expose nerve with blunt hemostatic clamp tip upward, separating from overlying structures
- Identify the tubercle of Zuckerkandl - mobilize laterally/anteromedially to expose the nerve fissure
- Trace nerve to its entry into the larynx (deep to cricothyroid)
- Berry's ligament is the final attachment - do NOT divide until nerve is clearly visualized
7. IONM Use (If Planned)
- Initial vagal baseline signal confirms ETT electrode contact
- Stimulate RLN at inferior thyroid artery level before and after dissection
- Loss of signal (LOS) = nerve stress or injury; PAUSE and assess before proceeding
- Facilitates decision on contralateral side in staged procedures
8. Contralateral Lobe
- Repeat steps on opposite side
- Identify both parathyroids on this side as well
9. Wound Closure
- Reapproximate strap muscles in midline
- Drain placement is surgeon preference (many omit for straightforward cases)
- Platysma closed with absorbable sutures
- Skin: subcuticular absorbable suture or skin glue for cosmesis
- Assess for hemostasis - neck hematoma is life-threatening (airway compression)
Complications
| Complication | Rate | Notes |
|---|---|---|
| RLN injury (temporary) | 1-5% | Majority resolve within 6 months |
| RLN injury (permanent) | < 1% (high-volume surgeons) | Higher with cancer, reoperative surgery |
| Hypoparathyroidism (transient) | Up to 30% | Hypocalcemia, paresthesias; usually resolves |
| Hypoparathyroidism (permanent) | 1-3% | Lifelong calcium/vitamin D supplementation |
| Neck hematoma | < 1% | Emergency re-exploration if airway compromised |
| EBSLN injury | 1-8% | Voice fatigue, loss of high-pitch projection |
| Thyroid storm | Rare | Risk in uncontrolled hyperthyroid patients |
High-volume surgeons (> 26 thyroidectomies/year) have demonstrably fewer complications, shorter stays, and lower costs. - Sabiston, p. 1522
Postoperative Care
- Serum calcium and PTH monitoring postoperatively
- Calcium and vitamin D supplementation empirically in many centers after total thyroidectomy
- Thyroid hormone replacement (levothyroxine) started on postoperative day 1
- Voice assessment before discharge
- The majority of total thyroidectomies can safely be performed in the outpatient setting
Alternative Approaches
- Robotic transaxillary thyroidectomy: Avoids neck incision; cosmetically superior; wider dissection required; 4-6 cm axillary incision + 8 mm medial skin incision with Da Vinci system
- Transoral (TOETVA): No visible scar; access through floor of mouth
- Minimally invasive video-assisted (MIVAT): Small midline incision + endoscopes; best for small glands
Sources:
- Current Surgical Therapy 14e (Sabiston/Cameron), pp. 898-901
- Sabiston Textbook of Surgery 21e, pp. 1522-1525
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, pp. 1040-1084
- Medscape - Thyroidectomy: Positioning and Technique
- StatPearls - Thyroidectomy
- Iowa Head and Neck Protocols - Thyroidectomy and Thyroid Lobectomy (incision marking tip)
This is a shared conversation. Sign in to Orris to start your own chat.